Introduction
The objective of root canal filling procedures should be the total three-dimensional filling of the root canals and all accessory canals. The complexity of the root canal system is well documented with accessory canals which are present in practically all teeth. Many of them are very small and calcified however some accessory canals are of considerable size, creating a two way passage of bacteria and tissue degradation products between the root canal space and periodontal tissue. Localized periodontal problems have been associated with bacteria and infected tissue debris enclosed in lateral canals of necrotic teeth (1)
DeDeus (2) demonstrated 27% of 1140 teeth examined had lateral canals mostly located in apical third. Rubach & Mitchell (3) observed lateral canals in 45 % of the teeth investigated. Lowman et al.(4) reported 55% of maxillary molars and 63 % of mandibular molars had accessory canals in the coronal and middle third of the root canals. Root canal filling procedures should be directed toward the filling of significant lateral canals as well as filling of main root canal (5). The necrotic tissue and bacteria residing in the lateral canals are difficult to remove by biomechanical preparation and this influences the quality of root filling as well as the outcome of the root canal therapy. The capacity of an endodontic filling technique to seal the canal irregularities is an important clinical parameter (5).
Several obturation techniques have been introduced in order to increase the adaptation of gutta-percha to irregularities of root canal. Lateral compaction of gutta-percha is one of the most accepted root canal obturation techniques. However, its ability to conform to the internal surface of the root canal has been questioned (6) . Studies have shown that plasticized gutta-percha can easily be moved into the canal irregularities, replicating the irregularities of the root canal system (5, 7). There are a number of methods using plasticized gutta-percha. These include warm lateral condensation, warm vertical condensation, coated carrier systems, injection systems and thermomechanical compaction. There are only a few studies comparing the effectiveness of all kinds of warmed gutta-percha techniques to fill the lateral canals (6, 8).
The aim of this study was to evaluate the filling of artificially prepared lateral canals using six different gutta-percha obturation techniques.
Materials and Methods
For this study, sixty extracted human single rooted teeth were used. Root canals were cleaned and instrumented to a # 50 file using step-back technique. The canals were irrigated with 5.25 % sodium hypochloride in every chance of file size and at the completion of instrumentation. Six lateral canals were created in the coronal, middle and apical thirds in each root using #15 engine driven reamer. The teeth were randomly divided into six groups of 10 and obturated using different techniques.
Group 1: Lateral condensation of gutta-percha with Kerr sealer (Kerr Pulp Canal Sealer, USA) was used. A gutta-percha master cone (Hygenic Corp, Akron,Ohio) was inserted into the canal at working length. AD 11 spreader was used to condense accessory gutta-percha cones and this procedure was repeated until spreader could no longer penetrate beyond the coronal third of the canal. Then, excess gutta-percha was removed with hot instrument after completed canal obturation.
Group 2: Microseal (Tycom,USA) An appropriate size of master cone was selected until tug back was confirmed. The appropriate spreader was used to condense the master cone of gutta-percha 1.0mm. short of working length. Appropriate compactors was selected regard to manifacturer instruction The sealer was placed into the canal and coated master gutta-percha cone was seated. The spreader was applied to the root canal alongside the master cone to appropriate length for compaction. The spreader was removed and compactor was inserted with heated gutta-percha which was taken from warmed cartidge. The gutta-percha coated compactor was carried to the void previously created in the canal by the spreader.
The compactor was placed as close to working length as possible .With the application of resisting force to the compactors’s backing-out motion, rotation of the compactor started at a speed of 6000 rpm. The compactor was removed 2 s.later, but rotation did not stop until the compactor was removed fully from the root canal. This procedure was repeated until no more space for spreader insertion.Then excess gutta-percha removed from the Access cavity.
Group 3. No# 40 Quick-Fill obturator (JS Quick-Fill, JS Dental Mfg, Inc., USA) which was two size smaller than the last file was coated with the sealer was used. The obturator was positioned in the canal until a slight resisitance was felt. Rotation was started until gutta-percha plasticized and slight pressure was applied apically until reaching working length. The shank of the carrier was cut by using an inverted cone bur.
Group 4: #50 Soft Core obturator (CMS Dental Aps.,Dentmark) was used according to information obtained from a “size verifier.” The root canal was coated with the sealer and the obturatior was heated.The plasticized Soft Core device was inserted to the apical stop. Excess plastic core was cut using a small inverted cone bur.
Group 5: The root canals were obturated using the System B technique ( SorbonEndo, CA, USA) for down pack and Obtura II (Obtura Corp,USA) for back filling according to the manifacurers information. The canals were coated with the sealer and a medium large non standardized gutta-percha cone was inserted into the canal within 0.5mm.of the working length. A medium large insert tip was used to condense guttapercha. The System B unit was prest to 200 Cº during apical condensation of the primary gutta-percha cone (down pack) when condensing condensing the apical portion, Obtura II was used for back filling.
Group 6: # 50 Thermafil obturator (Tulsa Dental, OK, USA) was used. Each canal was coated with the sealer and selected obturator was heated in a Thermaprep oven. The plasticized obturator was inserted into the canal within 0.5 mm. of the working length. Then the shank of each carrier was cut by using an inverted cone bur.
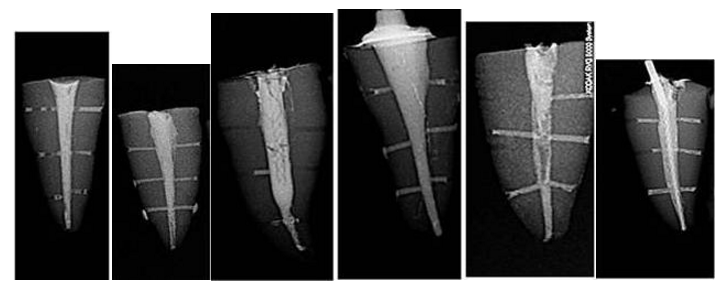
Kerr Pulp Canal sealer is used in all obturation techniques. Radiographs of the obturated canals were taken mesiodistally and scored according to the extension of filling of lateral canals (Figure 1a.b.c.d.e.f). Data were statistically analyzed using Kruskal Wallis non-parametric test (p<0.05)
Fig1. Radiographic Image of Obturated Lateral Canals of Each Group
Results
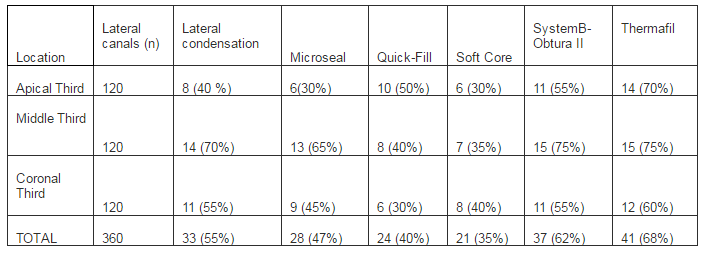
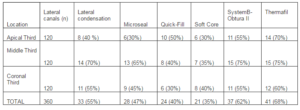
Mean percentage of complete filling with gutta-percha and sealer in lateral canals are presented in Table 1. Statistically more lateral canals were obturated by Thermafil and System B/Obtura than other techniques (p0.05). Also, statistically more lateral canals were filled in middle thirds of the canal than apical and coronal thirds in all techniques.
Table 1: Mean Percentage of Complete Filling with Gutta-Percha and Sealer in Lateral Canals
Discussion
A variety of previous studies evaluated different obturation techniques and materials for their ability to effectively fill the lateral canals. These studies used whether natural teeth with simulated lateral canals (7, 8, 9) or resin blocks with artificial lateral canals in attempt to standardize the experimental groups (6, 11, 12). Resin blocks provide a standardized sample of sufficient size and eliminate the variable effects of instrumentation (11). However, resin blocks have some limitations such as lack of a smear layer. Also, the surface texture and condition of resin could positively or negatively influence the flow properties of gutta-percha or sealer.
Few studies were performed to investigate dimension, shape and localization of lateral canals. Since, studies have shown limited amount of lateral canals (varied from 27 to 45%), simulated lateral canals were created to standardize and obtain sufficient number of samples in the present study. The diameter of the lateral canal was created by using engine driven reamer size 15, which was compatible with size of lateral canals (0.15mm) reported in previous study (13). Using this approach, it is possible to have the same lateral canals diameter and angle in relation to axis of the main canal.
Radiographic evaluation, clearing techniques or both methods have been used to identify the amount of filling achieved in lateral canals in natural teeth (7, 9, 10, 14). Clark & Eldeeb (15) reported that filled lateral and accessory canals on cleared teeth did not always appear on radiographic images. Almedia et al.(16) indicated that radiographs were not able to show lateral canal filling in approximately 8 % of cases. Matherne et al. (17 ) demonstrated the superiority of CBCT over conventional radiography in detecting supplemental canals. However, Tanomaru-Filho et al. (10) observed no significant difference between results of radiographic and visual analyses of cleared specimens. In the present study, radiographs were used to evaluate the amount of the filling of lateral canals.
Smear layer could influence the sealing properties of root canal fillings (18,19) investigated the effect of irrigating solution of filling of lateral canals and found teeth irrigated with %15 EDTA filled more lateral canals than the teeth irrigated with sodium hypochloride. However, irrigation with EDTA was shown to have no effect on the filling quality of root canal ramifications in several studies (20-22). In the present study, after the lateral canals were drilled, smear layer was created in order to mimic the clinical conditions and smear layer was not removed.
Previous studies, investigating the effect of obturation techniques, have given conflicting results. According to Weine (23) the type of obturation technique does not have an important effect on the obturation of the lateral canals. However, Goldberg et al. (7) found thermoplasticized gutta-percha techniques were more efficient than lateral condensation in filling lateral canals. Similarly, Kulild et al. (24 found that warm vertical condensation technique replicated artificially created defects beter than cold lateral condensation technique. The results in the present study were consistent with those studies (7, 24). Thermafil and System B+Obtura techniques were found to be more effective than lateral condensation technique regarding the filling artificially created lateral canals.
The use of sealer may allow beter filling of the root canal system because of its lubricating properties. Lateral canals may be obturated primarily with the sealer after vertical and lateral condensation techniques (6, 25). Almedia et al. (16) investigated filling ability of different sealers (AH plus, Epiphany, Endomethasone, Pulp Canal Sealer, Sealapex) in lateral canals and found that all sealers flowed into 0.1mm artifical canals by using lateral condensation technique. Pecora et al (26) showed that penetration of a zinc-oxide eugenol sealer into the lateral canals was dependent on the physical properties and the correct manipulation of the sealer. Reader et al. (6) found that the plasticized gutta-percha techniques resulted in significantly greater amounts of gutta-percha in lateral canals, wheras lateral and warm lateral condensation techniques produced lateral canals filled with significantly more sealer in resin blocks. Warm vertical condensation technique fill accessory canals in the cervical and middle thirds with gutta-percha and sealer, as well as in the apical deltas mostly with cement (5). DuLac et al. (8) investigated the effect of different gutta-percha techniques on filling lateral canals with sealer or gutta-percha by using resin blocks. They found lateral, warm lateral and carrier based techniques had significantly more sealer in the middle lateral canal than the thermoplasticized gutta-percha techniques On the other hand, the carrier based obturation technique placed significantly more gutta-percha in the apical lateral canals than other techniques. Kerr Pulp Canal Sealer was chosen for the present study due to its good physical properties (plasticity, slow setting time, dimentional stability on setting). The sealer might have occupied space in irregularities, allowing beter filling of the lateral canals. Radiographic findings may lead to misleading interpretations in relation to the filling of lateral canals with gutta-percha or selaer or both. Because the results were determined after radiographic evaluation, it was not intended to investigate the type of filling in the present study.
Conclusion
Thermafil and System B/Obtura techniques found to be superior to other techniques in filling lateral canals.
Acknowledgement
This study is supported by Marmara University’s Scientific Research Projects Committee
References
1.Stallard, R. E. (1972). “Periodontic-Endodontic Relationships,” Oral Surgery, Oral Medicine, Oral Pathology, 34; 314—26.
Publisher – Google Scholar
2. De Deus, Q. D. (1975). “Frequency, Location, and Direction of the Lateral, Secondary, and Accessory Canals,” Journal of Endodontics, 1(11):361-6.
Publisher – Google Scholar
3. Rubach, W. C. & Mitchell, D. F. (1965). “Periodontal Disease, Accessory Canals and Pulp Pathosis,” The Journal of periodontology, 36:34-8.
Publisher – Google Scholar
4. Lowman, J. V., Burke, R. S. & Pelleu, G. B. (1973). “Patent Accessory Canals: Incidence in Molar Furcation Region,” Oral Surgery, Oral Medicine, Oral Pathology, 36(4): 580-4.
Publisher – Google Scholar
5. Schilder, H. (1967). “Filling Root Canals in Three Dimensions,” Dental Clinics of North America, 723-44.
Publisher – Google Scholar
6. Reader, C. M., Himel, V. T., Germain, L. P. & Hoen, M. M. (1993). “Effect of Three Obturation Techniques on the Filling of Lateral Canals and the Main Canal,” Journal of Endodontics, 19(8):404-8.
Publisher – Google Scholar
7. Goldberg, F., Artaza, L. P. & De Silvio, A. (2001). “Effectiveness of Different Obturation Techniques in the Filling of Simulated Lateral Canals,” Journal of Endodontics, 27(5):362-4.
Publisher – Google Scholar
8. Dulac, K. A., Nielsen, C. J., Tomazic, T. J., Ferrillo, P. J. Jr & Hatton, J. F. (1999). “Comparison of the Obturation of Lateral Canals by Six Techniques,” Journal of Endodontics, 25(5):376-80.
Publisher – Google Scholar
9. Venturi, M., Di Lenarda, R., Prati, C. & Breschi, L. (2005). “An in Vitro Model to Investigate Filling of Lateral Canals,” Journal of Endodontics, 31(12):877-81.
Publisher – Google Scholar
10. Tanomaru-Filho, M., Sant’Anna, A. Jr, Berbert, F. L., Bosso, R. & Guerreiro-Tanomaru, J. M. (2012). “Ability of Gutta-Percha and Resilon to Fill Simulated Lateral Canals by Using the Obtura II System,” Journal of Endodontics, 38(5):676-9.
Publisher – Google Scholar
11. Wolcott, J., Himel, V. T., Powell, W. & Penney, J. (1997). “Effect of Two Obturation Techniques on the Filling of Lateral Canals and the Main Canal,” Journal of Endodontics, 23(10):632-5.
Publisher – Google Scholar
12. Karabucak, B., Kim, A., Chen, V. & Iqbal, M. K. (2088). “The Comparison of Gutta-Percha and Resilon Penetration into Lateral Canals with Different Thermoplastic Delivery Systems,” Journal of Endodontics, 34(7):847-9.
Publisher – Google Scholar
13. Vertucci, F. J. & Anthony, R. L. A. (1986). “A Scanning Electron Microscope Investigation of Accessory Foramina in the Furcation and Pulp Chamber Flor of Molar Teeth,” Oral Surgery, Oral Medicine, Oral Pathology, 62(3):319-26.
Publisher – Google Scholar
14. Venturi, M., Prati, C., Capelli, G., Falconi, M. & Breschi, L. (2003). “A Preliminary Analysis of the Morphology of Lateral Canals after Root Canal Filling Using a Tooth-Clearing Technique,” International Endodontic Journal, 36(1):54-63.
Publisher – Google Scholar
15. Clark, D. S. & Eldeeb, M. E. (1993). “Apical Sealing Ability of Metal versus Plastic Carrier Thermafil Obturators,” Journal of Endodontics, 19(1):4-9.
Publisher – Google Scholar
16. Almeida, J. F., Gomes, B. P., Ferraz, C. C., Souza-Filho, F. J. & Zaia, A. A. (2007). “Filling of Artificial Lateral Canals and Microleakage and Flow of Five Endodontic Sealers,” International Endodontic Journal, 40(9):692-9.
Publisher – Google Scholar
17. Matherne, R. P., Angelopoulos, C., Kulilid, J. C. & Tira, D. (2008). “Use of Cone Beam Compurted Tomography to Identify Root Canal Systems in Vitro,” Journal of Endodontics 34:87-89.
Publisher – Google Scholar
18. Gencoglu, N., Samani, S. & Günday, M. (1993). “Evaluation of Sealing Properties of Thermafil and Ultrafil Techniques in the Absence or Presence of Smear Layer,” Journal of Endodontics, 19(12):599-603.
Publisher – Google Scholar
19. Goldberg, F., Massone, J. E. & Spielberg, C. (1986). “Effect of Irrigation Solutions on the Filling of Lateral Root Canals,” Dental Traumatology, 2: 65-6.
Publisher – Google Scholar
20. Villegas, J. C., Yoshioka, T., Kobayashi, C. & Suda, H. (2002). “Obturation of Accessory Canals after Four Different Final Irrigation Regimes,” Journal of Endodontics, 28(7):534-6.
Publisher – Google Scholar
21. Bertacci, A., Baroni, C., Breschi, L., Venturi, M. & Prati, C. (2007). “The Influence of Smear Layer in Lateral Channels Filling,” Clinical Oral Investigations, 11(4):353-9.
Publisher – Google Scholar
22. Fachin, E. V. F., Scarparo, R. K. & Massoni, L. I. S. (2009). “Influence of Smear Layer Removal on the Obturation of Root Canal Ramifications,” Journal of Applied Oral Science, 17(3):240-3.
Publisher – Google Scholar
23. Weine, F. S. (1984). “The Enigma of the Lateral Canal,” Dental Clinics of North America, 28(4):833-52.
Publisher – Google Scholar
24. Kulild, J., Lee, C., Dryden, J., Collins, J., Feil, P. (2007). “A Comparison of Five Gutta-Percha Obturation Techniques to Replicate Canal Defects,” Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 103:E28-E32.
Publisher – Google Scholar
25. Bowman, C. J. & Baumgartner, J. C. (2002). “Gutta-Percha Obturation of Lateral Grooves and Depressions,”Journal of Endodontics, 28(3):220-3.
Publisher – Google Scholar
26. Pecora, J. D., Ribeiro, R. G., Guerisoli, D. M. Z., Barbizam, J. V., Marchesan, M. A. (2002). “Influence of the Spatulation of Two Zinc Oxide-Eugenol-Based Sealers on the Obturation of Lateral Canals,” Pesquisa Odontológica Brasileira, 16(2):127-30.
Publisher – Google Scholar