Introduction
The sella turcica is a saddle-shape depression in the sphenoid bone of the human skull. The anterior border of the sella turcica is represented by the tuberculum sellae and the posterior border by the dorsum sellae. The pituitary gland is surrounded by the sella turcica. Two anterior and two posterior clinoid process project over the pituitary fossa. The anterior clinoid processes are formed by the medial and anterior prolongations of the lesser wing of sphenoid bone, and the posterior clinoid process by the endings of dorsum sellae. During embryological development, the sella turcica is a key point for the migration of the neural crest cells to the fronto nasal and maxillary development fields.
The morphology of sella turcica is of importance in determining the cephalometric position of reference point sella. Variations in sella morphology have been discovered in skeletal Class III subjects1, cleft subjects2, in subjects with severe craniofacial deviations3, in dental anomalies4, and in syndromes5,6,7,8,9,10,11. Morphology of sella turcica in skeletal Class III malocclusion has been studied by various authors12,13,14,15. But the morphology of sella turcica in skeletal Class II subjects has not been reported. So this study was undertaken.
Materials and Methods
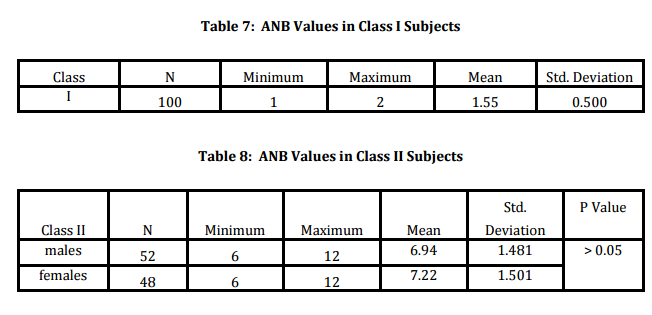
This was designed as a cross sectional study. The study population included cephalometric records of 100 skeletal Class II subjects and 100 Class I subjects, who reported to the Dept. Of Orthodontics, Govt. Dental College, Thiruvananthapuram for orthodontic treatment. This study was conducted in November 2013. The inclusion criteria were adults with no history of orthodontic or orthodontic-surgical treatment, no history of cleft lip repair, craniofacial deviations or other syndromes; For Class II subjects the inclusion criteria included ANB angle that should be more than 5 degree. The exclusion criterion was the presence of proximal caries.
A template as per description of Axelsson16 (2004) was prepared, this included the normal and the 5 variations. The cephalograms were available with patients reporting to the dept. Both Class II and Class I study population included males and females.
Result
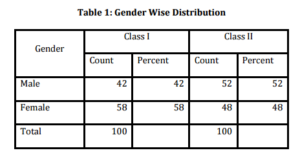
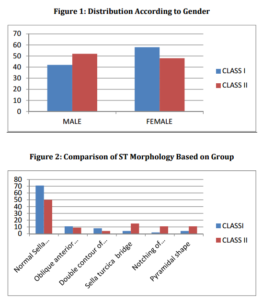
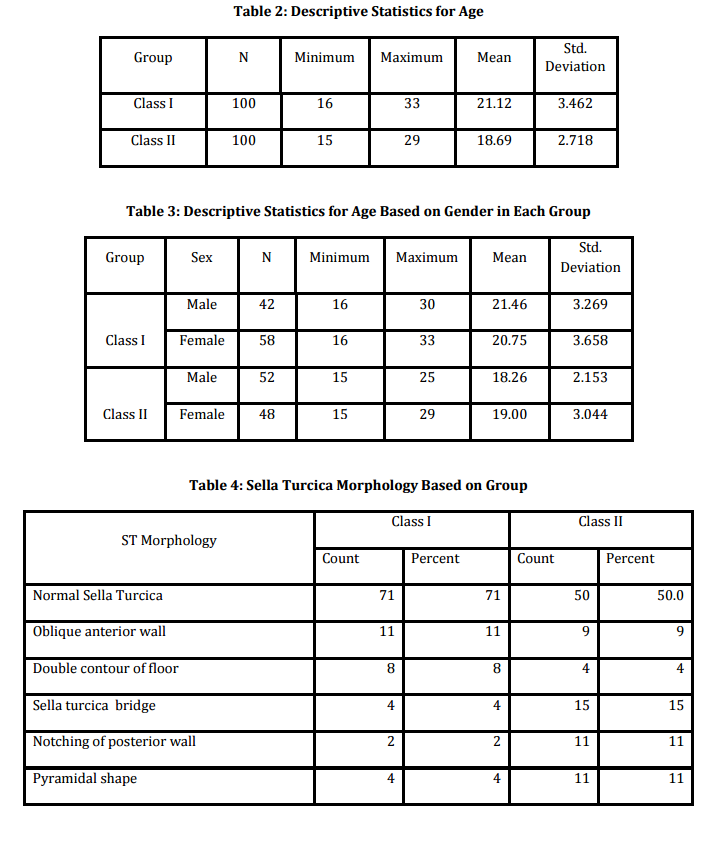
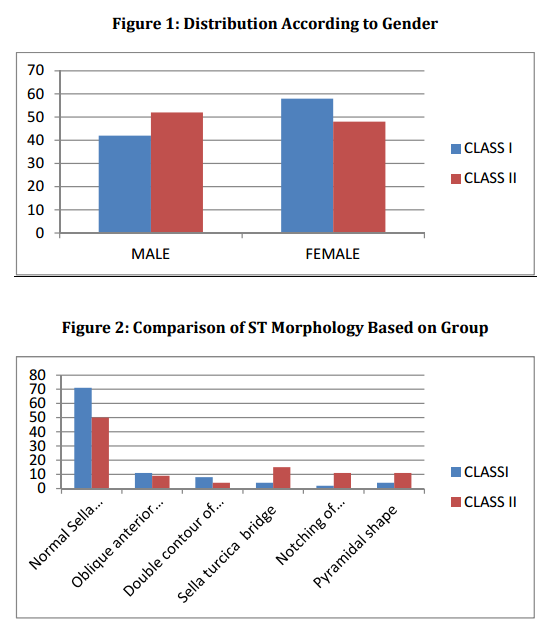
42% of Class I and 52% Class II subjects included in the study were males and 58% of Class I and 48% of Class II subjects were females [Table I] (Fig 1). The mean age of study population was 18.69±2.7 years(18.26 for males and 19 years for females) for Class II and 21.12±3.46 years (21.26 for males and 20.75 for females) for Class I subjects [Table 2 and Table 3].
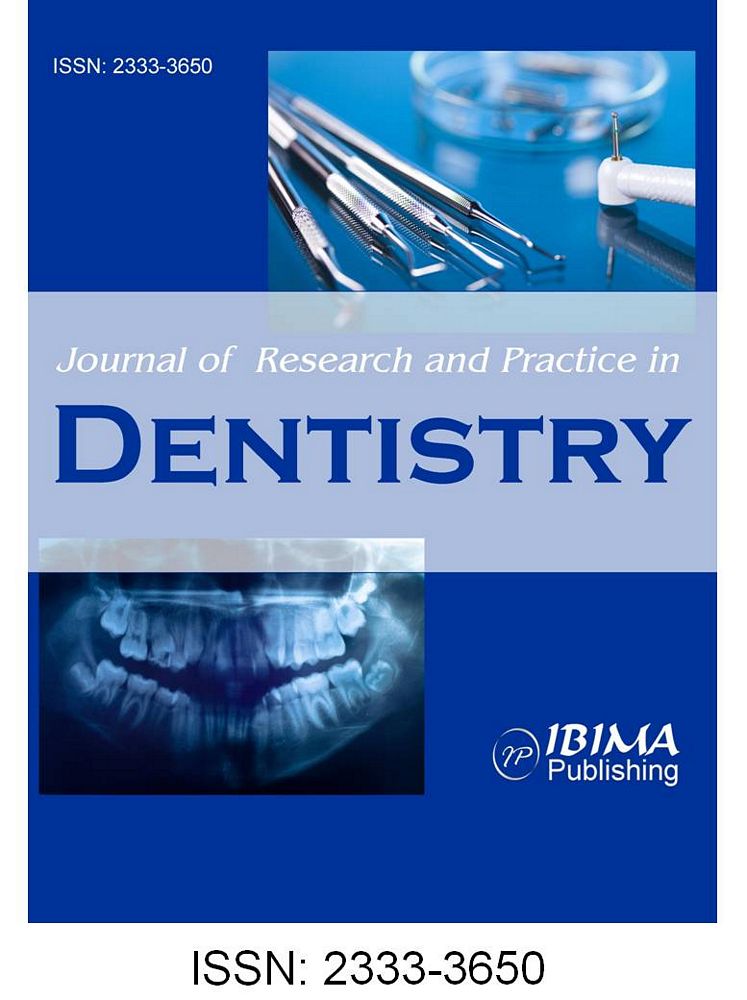
50% of Class II subjects included in the study presented with a normal sella turcica whereas 71% of the subjects in Class I malocclusion had a normal sella turcica morphology (p .05). 15% of Class II subjects presented with sella turcica bridging whereas only 4% of Class I subjects showed sella turcica bridging; this was statistically significant (p= .014). 11% of Class II subjects presented with notching of posterior wall whereas only 2% of Class I subjects included in the study had notching of posterior wall, this is statistically significant (p < .05) [Table 4 and Table 5] (Fig 2).
The proportion of oblique anterior wall, double contour of floor and pyramidal shape did not differ between skeletal Class I and skeletal Class II subjects [Table 3].
In gender wise classification, there was not a statistically significant difference in the normal sella turcica morphology between males and females [Table 6].
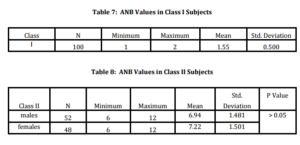
The data on ANB angle of the study population is presented in Table 7 and Table 8.
Socio Demographic Profile:


Discussion
This cross sectional study describes the morphology of sella turcica in skeletal Class II and skeletal Class I subjects. The study sample included adult patients with skeletal Class II malocclusion.
Morphology: Classifications of sella turcica morphology were attempted in literature. Appraisal of sella turcica morphology is a valuable aid in assessing the pathology in the pituitary gland17. Abnormal sella turcica morphology was reported in cases with severe craniofacial deviations3, various genetic disorders2, syndromes5-11 and in dental anomalies4, 18. Variations in sella turcica morphology have been reported by different authors. 75% of subjects in Silverman31’s study had a normal morphology for sella turcica and remaining 25% had an abnormal morphology. In the present study 50% of the adults with skeletal Class II showed a normal morphology of sella turcica.
Gorden19 (1922) classified the sella turcica morphology into 3 shapes, the circular, the oval or the flat/saucer shaped, their study sample included children of age ranging from 1 year to 12 years and most of them had either circular or oval shaped sella turcica. Davidoff and Epstein20 (1950) put forward the term J shaped sella while Fournier and Denizet21 (1965) used the term omega sella. Teal22 (1977) classified the sella anatomy into round, oval or flat. Bruneton et al23 (1979) studied the normal variants of sella turcica of adults.
Axelsson et al16 (2004) classified the sella turcica shapes into six types; normal sella turcica, oblique anterior wall, double contoured sella, sella turcica bridge, irregularity (notching) in the posterior part of the sella and pyramidal shape of the dorsum sellae. They analysed a sample from Oslo University Craniofacial Growth Archive (Norwegian 6-12 years) and reported that 71% of males and 65 % of females presented with a normal sella turcica morphology.
67% of the Saudi subjects in Alkofide12’s study; 80% of adults in skeletal Class III malocclusion and 70% of adults in skeletal Class I malocclusion in Iraqi adults in Hadeel et al20’s study; 65% of skeletal Class I patients and 72% of skeletal Class III patients from Islamabad in the Shah et al21’s study; and 48% of skeletal Class III and 75 % of skeletal Class I subjects included in Sathyanarayana et al24’s study in South Indian population had a normal sella turcica morphology. In the present study, 50% of skeletal Class II subjects and 71% of skeletal Class I subjects had a normal sella turcica morphology. The proportion of normal sella turcica morphology was statistically significant among skeletal Class I as compared to skeletal Class II.
18.6% of subjects in Becktor et al3’s study and 16.7% of subjects in Jones et al25’s study showed sella turcica bridging which was more than double the incidence of bridging previously reported.
Busch26, Muller27 and Platzer28 reported the prevalence of sella turcica bridge with a frequency of 1.75 to 6 % in the ‘normal’ population. Becktor et al3’s and Jones et al25’s study was on patients with severe craniofacial deviations who required combined surgical orthodontic treatment. In the present study 4% of skeletal Class I subjects had sella turcica bridging.
Abdel Kader et al29 (2007) showed significantly higher incidence of sella turcica bridging in subjects from Saudi Arabia with skeletal Class III malocclusion when compared to skeletal Class II and skeletal Class I malocclusion. The present study showed 15% of the Class I subjects with sella turcica bridging.
Marcotty et al1, in their investigations on Caucasian individuals, found 16.8% of skeletal Class III patients and 9.4% of skeletal Class I patients to have sella turcica bridging. Shah et al14 reported no incidence of sella turcica bridging in Islamabad orthodontic patients.
In a recent study by Sathyanarayana et al24 in South Indian population, 15% of subjects in skeletal Class III subjects and 5% of skeletal Class I subjects were reported to have sella turcica bridging. In the present study 15% of subjects with skeletal Class II malocclusion had sella turcica bridging (Table 5).
Also many authors had concluded that, the prevalence of sella turcica bridging is higher in subjects with dental anomalies, cleft lip and palate and various other anomalies.
Axelsson et al16 in their study on subjects from Oslo University Craniofacial Growth Archive reported 23 % of males and 3% of females to have an oblique anterior wall morphology. Sathyanarayana et al24 reported 7% of skeletal Class III subjects and 3% of skeletal Class I subjects (in South Indian population) and Hadeel et al30 reported 3.3% of skeletal Class III subjects and 4% of skeletal Class I subjects included (Iraqi adult population) to have oblique anterior wall morphology of sella turcica. In the present study 9% of skeletal Class II and 11% of skeletal Class I subjects presented with an oblique anterior wall. The proportion of oblique anterior wall morphology of sella turcica did not differ significantly between skeletal Class I and skeletal Class II malocclusion groups included in the study.
In the study on double contour of floor morphology of sella turcica, Alkofide12(study on orthodontic patient population from Saudi Arabia) reported 9.4% of the study sample, Shah et al14 reported 1.6% of skeletal Class III subjects and 5% of skeletal Class I subjects of study sample (Islamabad), Sathyanarayana et al24 reported 7% of skeletal Class III subjects and 3% of skeletal Class I subjects (South Indian population), Hadeel et al30 reported 10% of skeletal Class III subjects and 14% of skeletal Class I subjects( Iraqi adults), Alkofide12 reported 8.9% of orthodontic patient population (Saudi Arabia) and Axelsson et al16 reported 3% of females included in the study (Oslo University Craniofacial Growth Archive) to have double contour of floor. In the present study, 8% of Class I and 4% of Class II presented with double contour of floor.
2.8% of orthodontic population ( Saudi Arabia) in Alkofide12’s study, 5% of females in Axelsson et al16’s study, 10% of skeletal Class III subjects and 8.3% of skeletal Class I subjects included in Shah et al14’s study, 7% of skeletal Class III subjects and 2% of skeletal Class I subjects ( South Indian population) in Sathyanarayana et al24’s study, 3.3% of skeletal Class III and 4% of skeletal Class I subjects in Hadeel et al30’s study presented with a pyramidal shape morphology of dorsum sella. In the present study 11% of skeletal Class II and 4% of skeletal Class I subjects presented with a pyramidal shape of sella turcica.
In the present study 11% of skeletal Class II subjects showed notching of the posterior part of sella turcica. 17% of Skeletal Class III subjects and 12% of Skeletal Class I subjects in Sathyanarayana et al24’s study (South Indian population), 3.3% of skeletal Class III subjects and 6% of skeletal Class I subjects Hadeel et al30’s study, 10% of skeletal Class III subjects and 13.3% of skeletal Class I subjects of Shah et al’s study (Islamabad), 11.1% of the orthodontic patient population (Saudi Arabia) in Alkofide12’s study and 11% of females (Oslo University Craniofacial Growth Archive) in Axelsson et al16’s study had irregularities of posterior part of dorsum sella.
Conclusion
The present study showed 71% of Class I and 50% of Class II subjects to have normal sella turcica morphology. The variation in proportion of normal sella turcica was statistically significant among Class I as compared to Class II. Bridging of sella turcica and the notching of posterior wall were seen to be significantly more among Class II subjects than among Class I subjects.
References
1. Meyer-Marcotty, P., Reuther, T. & Stellzig-Eisenhauer, A. “Bridging of the Sella Turcica in Skeletal Class III Subjects,”The European Journal of Orthodontics (2010); 32(2):148-53.
Publisher – Google Scholar
2. Alkofide, EA. “Sella Turcica Morphology and Dimensions in Cleft Subjects,” Cleft Palate Craniofac Journal (2008); 45(6):647-53.
Publisher – Google Scholar
3. Becktor, J. P, Einersen, S. & Kjae,r I. “A Sella Turcica Bridge in Subjects with Severe Craniofacial Deviations,” The European Journal of Orthodontics, (2000); 22(1):69-74.
Publisher – Google Scholar
4. Leonardi, R., Barbato, E., Vichi, M. & Caltabiano, M. “A Sella Turcica Bridge in Subjects with Dental Anomalies,” The European Journal of Orthodontics (2006); 28(6):580-5.
Publisher – Google Scholar
5. Russell, B. G. & Kjaer, I. “Postnatal Structure of the Sella Turcica in Down Syndrome,”. American Journal of Medical Genetics (1999); 87(2):183-8.
Publisher – Google Scholar
6. Weinstein, M., Tyrrell, B. & Newton, T. H. “The Sella Turcica in Nelson’s Syndrome,” Radiology (1976); 118(2):363-5.
Publisher – Google Scholar
7. Axelsson, S., Storhaug, K. & Kjaer, I. “Post-Natal Size and Morphology of the Sella Turcica in Williams Syndrome,” The European Journal of Orthodontics (2004); 26(6):613-21.
Publisher – Google Scholar
8. Childers, N. K. & Wright, J. T. “Dental and Craniofacial Anomalies of Axenfeld-Rieger Syndrome,” Journal of Oral Pathology & Medicine (1986); 15(10):534-9.
Publisher – Google Scholar
9. Koshino, T., Konno, T. & Ohzek,i T. “Bone and Joint Manifestations of Rieger’s Syndrome: A Report of a Family,”Journal of Pediatric Orthopaedics (1989); 9(2):224-30.
Publisher – Google Scholar
10. Meyer-Marcotty, .P, Weisschuh, N., Dressler, P., Hartmann, J. & Stellzig-Eisenhauer, A. “Morphology of the Sella Turcica in Axenfeld-Rieger Syndrome With PITX2 Mutation,” Journal of Oral Pathology & Medicine (2008); 37(8):504-10.
Publisher – Google Scholar
11. Venable, H. P.”Empty Sella Syndrome,” Journal of the National Medical Association (1977); 69(4):243-7.
Publisher – Google Scholar
12. Alkofide, E. A. “The Shape and Size of the Sella Turcica in Skeletal Class I, Class II, and Class III Saudi Subjects,” The European Journal of Orthodontics (2007); 29(5):457-63.
Publisher – Google Scholar
13. Cutovic, T., Pavlovic, J. & Kozomara, R. “Analysis of Dimensions of Sella Turcica in Patients with Mandibular Prognathism,” Vojnosanit Pregl (2008); 65(6):456-61.
Publisher – Google Scholar
14. Mahmood Shah, A., Bashir, U., Tasleemilyas. “The Shape and Size of the Sella Turcica in Skeletal Class I, II & III in Patients Presenting at Islamic International Dental Hospital, Islamabad,” Pakistan Oral & Dental Journal June (2011); 31(1):104-10.
Publisher – Google Scholar
15. Marsan, G. & Oztas, E. “Incidence of Bridging and Dimensions of Sella Turcica in Class I and III Turkish Adult Female Patients,” World Journal of Orthodontics (2009); 10(2):99-103.
Publisher – Google Scholar
16. Axelsson, S., Storhaug, K. & Kjaer, I. “Post-Natal Size and Morphology of the Sella Turcica. Longitudinal Cephalometric Standards for Norwegians between 6 and 21 Years of Age,” The European Journal of Orthodontics (2004); 26(6):597-604.
Publisher – Google Scholar
17. Kjaer, I., Keeling, J. W., Reintoft, I., Nolting, D. & Fischer Hansen, B. “Pituitary Gland and Sella Turcica in Human Trisomy 21 Fetuses Related to Axial Skeletal Development,” American Journal of Medical Genetics (1998); 80(5):494-500.
Publisher – Google Scholar
18. Leonardi, R., Farella, M. & Cobourne, M. T. “An Association between Sella Turcica Bridging and Dental Transposition,” The European Journal of Orthodontics (2011); 33(4):461-5.
Publisher – Google Scholar
19. Gordon, M. B BAL. “A Roentgenographic Study of the Sella Turcica in Normal Children,” Endocrinology,
(2013).
Publisher – Google Scholar
20. Epstein, B. S. & Davidoff, L.M. “Advanced Atrophy and Enlargement of the Sella Turcica with Destruction of the Sphenoid,” The American Journal of Roentgenology and Radium Therapy (1951); 66(6):884-93.
Publisher – Google Scholar
21. Fournier A.M, Denizet D.”Omega-Shaped Sella Turcica,” Marseille Médical (1965); 102(6):503-9.
Publisher – Google Scholar
22. Teal, J. S. “Radiology of the Adult Sella Turcica,” Bulletin of the Los Angeles Neurological Societies (1977); 42(3-4):111-74.
Publisher – Google Scholar
23. Bruneton, J. N., Drouillard, J.P., Sabatier, J.C., Elie, G.P. & Tavernier, J.F. “Normal Variants of the Sella Turcica: Comparison of Plain Radiographs and Tomograms in 200 Cases 1,” Radiology (1979); 131(1):99-104.
Publisher – Google Scholar
24. Sathyanarayana, H.P. Kailasam, V. & Chitharanjan, A. B. “The Size And Morphology of Sella Turcica in Different Skeletal Patterns among South Indian Population: A Lateral Cephalometric Study,” Journal of Indian Orthodontic Society (2013);47(4):266-71.74.
Publisher – Google Scholar
25. Jones, R. M., Faqir, A., Millett, D. T., Moos, K. F. & McHugh, S. “Bridging and Dimensions of Sella Turcica in Subjects Treated by Surgical-Orthodontic Means Or Orthodontics Only,” Angle Orthodontist (2005); 75(5):714-
Publisher – Google Scholar
26. Busch, W. “Die Morphologie der Sella turcica und ihre Beziehungen zur Hypophyse,” Virchows Archiv (1951); 320:437—58.
Publisher – Google Scholar
27. Müller, F. “Die Bedeutung der Sellabrückefür das Auge,” Klinische Monatsblätter für Augenheilkunde (1952); 120: 298—302.
Google Scholar
28. Platzer, W. “Zur Anatomie der Sellabrücke und Ihrerbeziehungzur A. Carotisinterna,” Fortschritte auf Demgebiet Der Roentgenstrahlen und der Nuklearmedizin (1957) 87:613—16.
Google Scholar
29. Abdel-Kader, HM. “Sella Turcica Bridges in Orthodontic and Orthognathic Surgery Patients. A Retrospective Cephalometric Study,” Australian Orthodontic Journal (2007); 23(1):30-5.
Publisher – Google Scholar
30. Yassir, Y.A, Yousif , H. A. & Nahidh, M. “Size and Morphology of Sella Turcica in Iraqi Adults,”. Mustansiria Dental Journal 30-23:(17);(2010).
Google Scholar
31. Silverman, F. N. “Roentgen Standards Fo-Size of the Pituitary Fossa from Infancy through Adolescence,” The American Journal of Roentgenology (1957); 78(3):451-60.
Publisher – Google Scholar



{kind=link}