Introduction
Uterine Fibroids are the most common benign (non-cancerous) tumor found in women. There seems to be a relationship between fibroids and infertility; in fact these benign tumors have been associated with subfertility in 5-10 as demonstrated by Buttram Jr et all(1981), and this relationship has become more obvious because of the fact that surgical intervention does actually increase pregnancy rates. For example, myomectomy for fibroid-associated infertility has been associated with 50 % of women conceiving after the intervention, as shown by Somigliana et al (2007), making it clearerthat there is a relation between fibroids and infertility
But, despite the existence of many studies assessing the correlation between fibroids and infertility, the exact mechanisms by which these benign tumors affect the reproductive function is still unclear for both difficulty conceiving and early pregnancy loss; even if the exact way that fibroids interfere with fertility is not clear cut, there are several theories.
One of them published by Buttram et al (1981) incriminates the hyperestrogenic environment to be responsible for the anovulatory cycles. Other theories mentioned by Buttram et al (1981) and Deligdish et al (1970) said that the pathological changes of the endometrium and myometrium caused by the presence of fibroids are responsible for implantation failure. And, Richards et al (1998) have said that infertility is caused by a problem in uterine contraction which makes it difficult for spermatozoa to reach the ovocyte or make it difficult for the ovum to be able to accomplish nidation in normal way, and thus, creating infertility problem for women.
However, not only the presence of fibroids can cause infertility, but it is also related to the anatomical location; all fibroid do not cause infertility to the same extent. For example, it have been shown by Eldar-Geva et al (1998) that the submucosal fibroids are most associated with infertility followed by intramural fibroids and finally subserosal fibroids are the least associated with infertility.
The present retrospective study was performed to evaluate whether uterine fibroids may influence the reproductive function in women and cause decrease in fertility.
Methods
We did a retrospective study using the archived records of 83 patients who visited the Maternity and were treated with surgery to remove fibroids, for a period ranging from 2 May 2011 to 14 May 2012.
We have established an individual survey sheet containing the following variables: The Age of the women, The number of abortions they had in the past, the marital status, the Parity; the existence of Gyneco-obstetric history problems andfamily history of fibroids, the age of menarche; The reasons for consultation; The number of fibroids, their location and their size, the type of intervention; and the infertility problem.
Data of the questionnaire were analyzed using the software program stat-view (1998). Frequencies and percentages were calculated. ANOVA test was performed to investigate the significance in the association of the different variables and infertility. Correlations were considered significant with the observed significance level (P-value was <0.05).
Results
May 2, 2011 to may 14 2012, 2886 pregnant women attended the MCH center in Sidi Bel Abbes (west of Algeria). 83 women were recruited. The mean age was 41 ± 8.11 years (range 26-68 years).
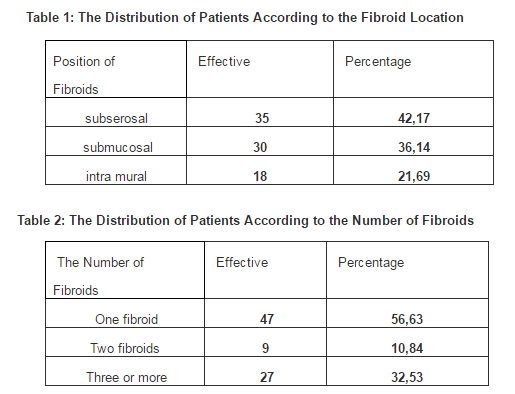
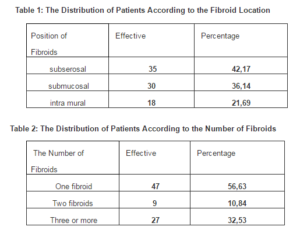
Of the 83 women affected by uterine fibroid, 35 patients had subserosal fibroids (42, 17%), while 30 had submucosal fibroids (36.14%) and 18 had intramural fibroids (21.69%) (Table 1)
The majority of patients (47 cases /56.63%) had only one fibroid. 9 patients (10.83%) had 2 fibroids and 27 patients had more than 3 fibroids (32.53%),(Table 2.).
The average age of women suffering from uterine fibroid in our study was 41 years; the number of cases gradually decreases in both younger women (9 cases for the group aged between 20-29 years), and in older women (1 case for the women with age above 59 years).
51.81% of the women affected by uterine fibroid were nulliparous and the percentage of multiparous women affected by fibroid was lower 31.33%,
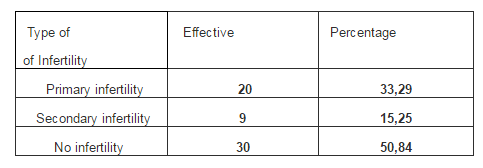
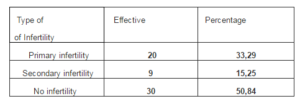
Concerning infertility in our series, 14.46 % of consultations were done by women suffering from infertility problem; 29 patients (49.16%) had infertility problem, 33.89% had primary infertility, and 15.25% had secondary infertility (Table 3).
Table 3: The Distribution of Patients According to the Type of Infertility
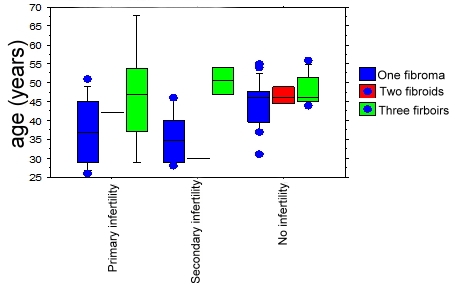
Concerting the relation between infertility age and the number of fibroids, we found that women with a median age of 47 and having more than 3 fibroids were the ones suffering the most from infertility (Figure 1).
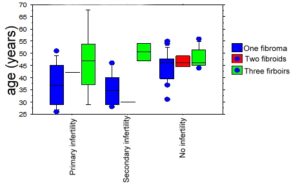
Figure 1: Comparison of the Distributions of the Type of Infertility Based on the Age and Number of Fibroids
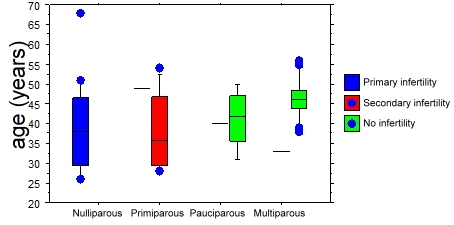
The presence of submucosal fibroids was most associated with a decrease in fertility causing primary infertility in women with the median age of 35, followed by the subserosal fibroids (Figure 2).
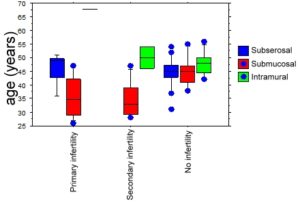
Figure 2: Comparison of the Distributions of Infertility in function of Age and Positions of the Fibroid
Submucosal fibroid was also found primary in women suffering from secondary infertility with a median age of 32.5, followed by intra mural fibroid (Figure 2).
Secondary infertility was also found in primiparous patients affected by uterine fibroid with a median age of 32. 5, andmultiparity was associated with a decrease in the incidence of fibroids. (Figure 3).
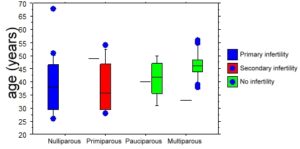
Figure 3: Comparison of Distributions of Parity According to the Age and the Type of Infertility
About miscarriage, we found that the large number of pregnancy loss occurred in women who were affected by one uterine fibroid associated with secondary infertility
Concerning the family history of the women suffering from fibroids, only 3.61% of women presented some family history of fibroids:
– 2 patients whose mothers had fibroids.
– 1 patient whose sister has been affected by fibroids
The age of menarche was also associated with fibroids, the proportion of patients whose age at menarche was early (11-13 years) is significantly higher (77.11%), with a peak at the age of 13 years, (50.60%), and only (22.89%) in women withage at menarche was ≥ 14 years suffered from fibroids .
Discussion
In our study, 49.16% of our patients complained about fertility problem The association between fibroids and infertility was found by Elizabeth A et al (2009) in their systematic review of 347 articles. They showed that a presence of fibroids no matter their locations was always associated with a higher bad outcome for pregnancy when compared to control subjects.
Concerning the location of the fibroids and its relation to infertility in our study, we found this order: submucosal, subserosal and intramural.
But the information concerning the location of the fibroids and their relation to infertility seems to be conflicting and this is what was found in a research study by Eldar-Geva et al (1998) and Dessolle et al (2001). However, concerning submucosal and intramural fibroids, some studies done by Garcia et al (1984) and Giatras et al (1999) have shown that they affect the installing and continuation of pregnancy because of the distortion of the uterine cavity that they are responsible for.
The research of Maria et al (2006) found that infertility can also be caused if the fibroids develop close to the tubaric ostium, making the transport of the spermatozoa or the embryo more difficult and therefore causing infertility.
In our study, uterine fibroids were associated with miscarriage that has been shown by a number of studies where they found that the number of miscarriages is higher in women with fibroids. This can be due to the fact that if the fibroids are close to the placenta, this can eventually cause spontaneous miscarriage as demonstrated by Muram et al (1980) and Rosati et al (1989). However, according to Li TC et al (1999), the rate of miscarriage caused by fibroids is not exact and it is very high in the literature.
Multiparity was associated with a decreased incidence of fibroids compared with nulliparous women. The same results were reported by Bulletti et al (1999) and Richards et al (1998). Fibroids are believed to be common in nulliparous or relatively infertile women as mentioned by Howkins and Bourne (1989), and in another study, Howkins and Bourne (1985) showed that in fact 60% of myomata occurred in women who had no previous pregnancy or had given birth only once.
However, some studies done by Jyoti C et al (2012) and Ibrar et all (2010) have shown that Multiparous patients are found to have fibroids more frequently than nulliparous women.
Fibroids are usually found in reproductive age groups. These tumors are most frequently seen clinically between the ages of 30 and 45; although they may start developing in the early twenties as mentioned by Masani (1982). In the present study, the highest incidence (48.19%) was observed between 40-49 years. This finding correlates well with the observations made by the study of Shakira et Subhana (2008) and Reddy et Malathy (1963).
In our study, only 3.61% of patients had family history of fibroids. The relationship between family history of fibroids and the occurrence of infertility has been shown in other research studies, like the study done by Alam et al (2001), Snieder et al (1998) and Reddy DB and Malathy PM (1963).
Conclusion
The relationship between fibroids and infertility is still subject to a large debate, and we still do not know exactly if they indeed cause infertility or it is a simple association. However, in our study, we found that 49.16% of our patientscomplained about fertility problem, showing that the association between fibroids and female infertility is not uncommon. For now, it would be interesting to investigate the different ways by which fibroids can cause fertility problems, either by creating problem in the fertilization processes or by being responsible for early pregnancy loss.
References
1-Buttram, Jr. V. C. & Reiter, R. C. (1981). “Uterine Leiomyomata: Etiology, Symptomatology, and Management,” Fertil Steril, 36 (4): 433—445.
Publisher – Google Scholar
2- Somigliana, E., Vercellini, P., Daguati, R. et al. (2007). “Fibroids and Female Reproduction: A Critical Analysis of the Evidence,” Human Reproduction Update, 13(5): 465—476.
Publisher – Google Scholar
3-Buttram, V. C. & Reiter, R. (1981). ‘Uterine Leiomyomata: Aetiology, Symptomatology, and Management,’ Fertil Steril, 36 (4): 433—443.
4-Deligdish, L. & Loewenthal, M. (1970). “Endometrial Changes Associated with Myomata of Uterus,” Journal of Clinical Pathology, 23:676—680.
Publisher – Google Scholar
5-Richards, P. A, Richards, P. D. G. & Tiltman, A. J. (1998). “The Ultrastructure of Fibromyomatous Myometrium and Its Relationship to Infertility,” Human Reproduction Update, 4:520—525
Publisher – Google Scholar
6-Eldar-Geva, T., Meagher, S., Healy, D. L., MacLachlan, V., Breheny, S. & Wood, C. (1998). “Effect of Intramural, Subserosal and Submucosal Uterine Fibroids on the Outcome of Assisted Reproductive Technology Treatment,” Fertil Steril,70 (4):687—691.
Publisher – Google Scholar
7-. Elizabeth, A. Pritts, M., William, H. Parker, D. & David, L. (2009). “Fibroids and Infertility: An Updated Systematic Review of the Evidence,” Fertility and Sterility, 91(4): 1215- 1223
Publisher – Google Scholar
8-Dessolle, L., Soriano, D., Poncelet, C. (2001). “Determinants of Pregnancy Rate and Obstetric Outcome after Laparoscopic Myomectomy for Fertility,” Fertil Steril, 76:370—374.
Publisher – Google Scholar
9-Garcia, R. C. & Tureck, R. W. (1984). “Submucosal Leiomyomas and Infertility,” Fertil Steril, 42: 16—19.
Publisher – Google Scholar
10-Giatras, K,, Berkeley, A. & Noyes, N. (1999). “Fertility after Hysteroscopic Resection of Submucosus Myomas,” The Journal of the American Association of Gynecologic Laparoscopists;6:155—158.
Publisher – Google Scholar
11-Maria, L., Federica, R., Riccardo, A. & Vittorio, U. (2006). “Effects of the Position of Fibroids on Fertility,”Gynecological Endocrinology, 22(2): 106—109
Publisher – Google Scholar
12-Muram, D, Gillieson, M. & Walters, J. H. (1980). ‘Myomas of the Uterus in Pregnancy: Ultrasonographic Follow-up,’Am J Obstet Gynecol, 138: 16—19.
Google Scholar
13-Rosati, P., Bellati, U. & Exacoustos C. (1989). “Uterine Myoma in Pregnancy: Ultrasound Study,” International Journal of Gynecology & Obstetrics, 28: 109—117.
Publisher – Google Scholar
14-Li, T. C,, Mortimer, R. & Cooke, I. D. (1999). “Myomectomy: A Retrospective Study to Examine Reproductive Performance before and After Surgery,” Human Reproduction, 14: 1735—1740.
Publisher – Google Scholar
15-Bulletti, C, D., De Ziegler, Polli, V. & Flamigni, C. (1999). “Le Rôle Des Léiomyomes Dans L’infertilité,” The Journal of the American Association of Gynecologic Laparoscopists, 6:441-445.
Publisher – Google Scholar
16-Richards, P. A., Richards, P. D. G. & Tiltman, A. J. (1998). “L’ultra structure du Myomètre Fibromyomatouse et sa Relation avec l’infertilité, ” Human Reproduction Update, 4:520-525
Publisher – Google Scholar
17- Howkins & Bourne. (1989). ‘Textbook of Gynecology,’ 10th edition, New delhi; Churchill Livingstone; p 399-427.
18- Howkins and Bourne. (1985). ‘Shaw’s Textbook of Gynecology.,’ 9th Ed. Bombay; B.I.Publications Pvt Ltd; P. 564-605.
19- Jyoti, C. , Vipul, P., Kinnar, S., .Jadav, R., Chaudhary, S. M. & Pensi, C. A. (2012). “Uterine Leiomyoma: Clinical Profile At Civil Hospital, Ahmed,” National Journal of Integrated Research in Medicine, 3: 50-53
Publisher – Google Scholar
20- Ibrar, F., Riaz, S., Dawood, N. S. & Jabeen, A. (2010). “Frequency of Fibroid Uterus in Multipara Women in a Tertiary Care Centre in Rawalpindi,” J Ayub Med Coll Abbottabad ;22(3):155-7.
Publisher – Google Scholar
21- Masani, K. M. (1982). ‘New Growths of Cervix and Uterus. Fibromyomata,’ In: Textbook of Gynecology. 8thEdition. Bombay; PopularPrakashan: P. 355-357.
Google Scholar
22- Shakira, P. & Subhana, T. (2008). “A Clinicopathological Review of Elective Abdominal Hysterectomy,” Journal of Surgery Pakistan (international) 13(1):26-29.
Publisher – Google Scholar
23-Reddy, D. B. & Malathy, P. M. (1963). “’Fibromyoma Uterus,’ J of obstet & gynecol of India, 13: page 54.
24- Vikhlyaeva, E. M., Khodzhaeva, Z. S. & Fantschenko, N. D. (1995). “Familial Predisposition to Uterine Leiomyomas,” International Journal of Gynaecology Obstetrics, 51,127—131
Publisher – Google Scholar
25- Alam, N. A., Bevan, S., Churchman, M., Barclay, E., Barker, K., Jaeger, E. E., Nelson, H. M., Healy, E., Pembroke, A. C., Friedmann, P. S. et al. (2001) “Familial Prevalence of Fibroids Localization of a Gene (MCUL1) for Multiple Cutaneous Leiomyomata and Uterine Fibroids to Chromosome 1q42.3-q43,” The American Society of Human Genetics,68, 1264—1269.
Publisher – Google Scholar
26- Snieder, H., MacGregor, A.J. & Spector, T.D, (1998). “Genes Control the Cessation of a Woman’s Reproductive Life: A Twin Study of Hysterectomy and Age at Menopause,” The Journal of Clinical Endocrinology & Metabolism, 83; 1875—1880
Publisher – Google Scholar