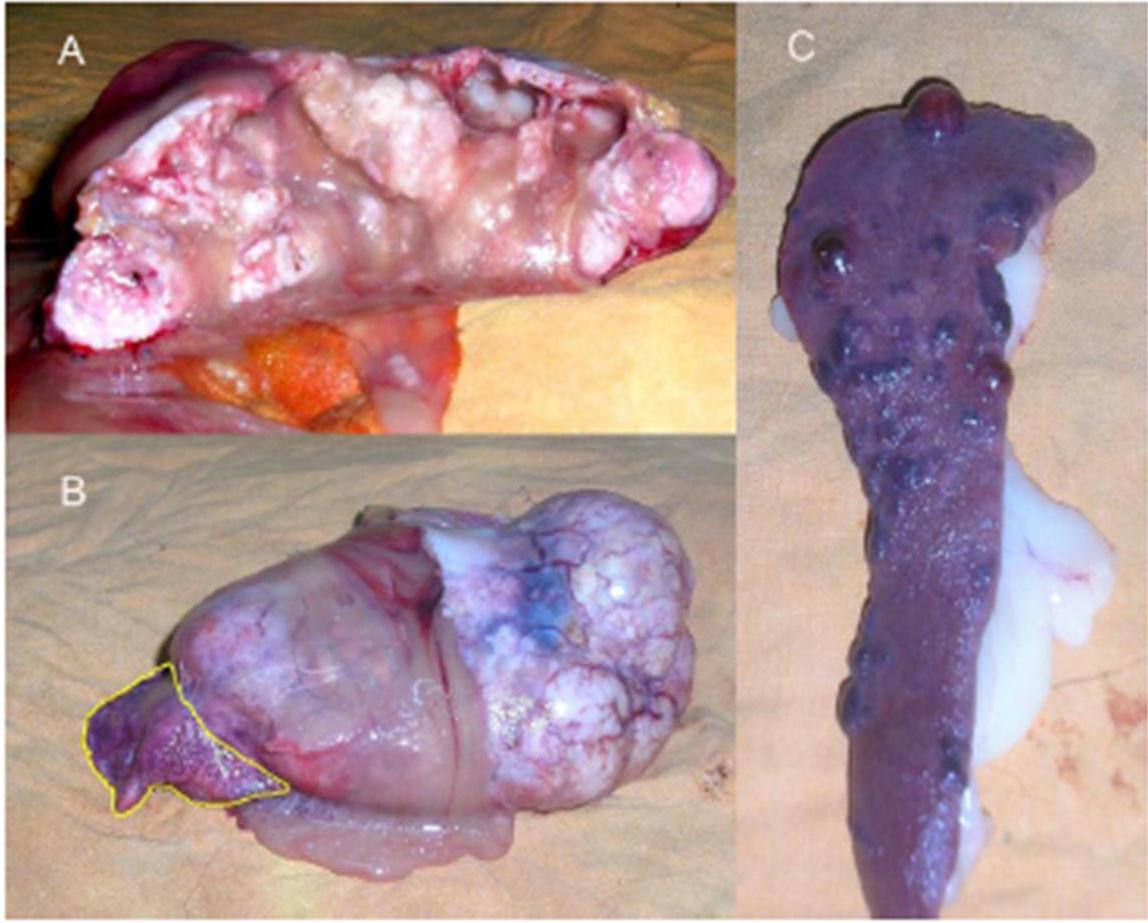
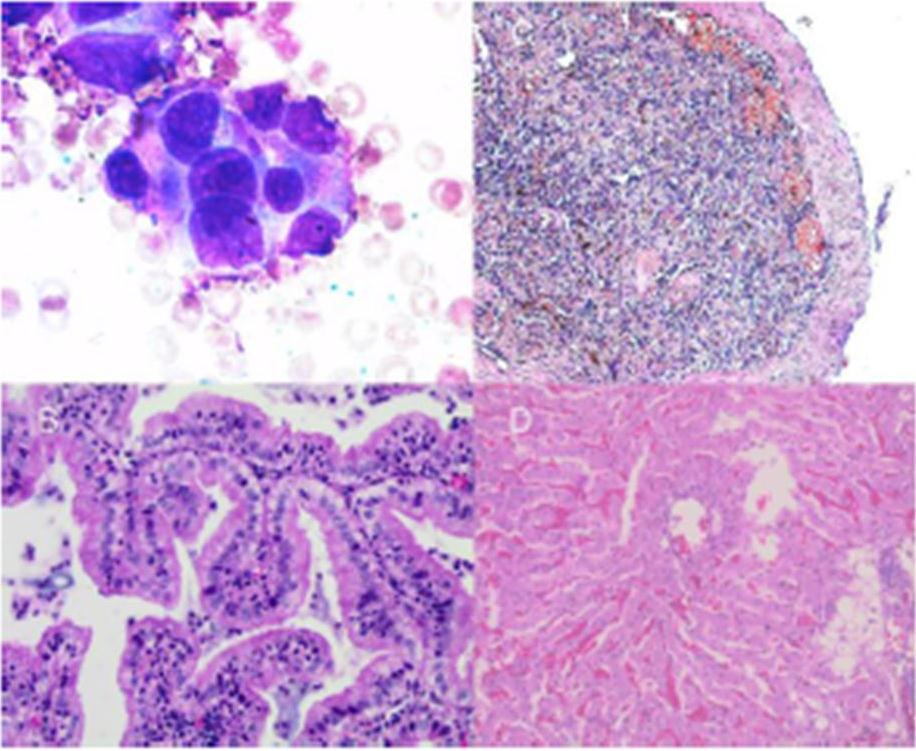
Despite having made only one cytoreductive surgery and after of drainage of the ascitic fluid accumulated in the abdominal cavity the animal improved in the first 48 hours after surgery. Within this 48 hours the animal was more active, had eaten some food and tolerated it and had minimal edema in the limbs. Postoperative chemotherapy with doxorubicin (Doxocris 50, LKM, Buenos Aires, Argentina), 30 mg/m2 IV was initiated immediately after surgery. The dog deteriorated 2 weeks after treatment and died. A complete necropsy (excluding the central nervous system) was performed. The right accessory lung lobe was replaced by a large tumor (11 x 6 x 4 cm) previously diagnosed as a papillary pulmonary adenocarcinoma (Fig. 2 B). Due to the large size of the tumor, the CVC was almost completely compressed. The spleen had multiple red-brown nodules (Fig. 1 C) ranging from 0.5 to 1.3 cm in diameter; these splenic masses were histopathologically diagnosed as chronic splenitis (Fig. 2 C). The liver had vacuolar degenerative changes (Fig. 2 D).
Discussion
BCLS is classified as primary, if the obstruction is the result of endoluminal venous lesion, such as thrombosis; or secondary, if the obstruction is caused by neighboring structures such as extrinsic compression or tumor invasion.
In this report we discuss a dog with secondary BCLS associated with a primary pulmonary adenocarcinoma. Secondary BCLS is rare in dogs, and has been reported due to liver lobe entrapment within the falciform ligament11, congenital hiatal hernia12 and selected heart diseases3, 8. In humans, other causes such as parasitic liver diseases or liver abscesses have also been reported in the literature.1
Obstruction of two or more major hepatic veins increases the sinusoidal pressure and reduces sinusoidal blood flow, producing clinical disease. The result of these hemodynamic changes is sinusoidal dilation and exudation of interstitial fluid, which diffuses through the liver capsule when the capacity of lymphatic drainage exceeds.
Ascites was classified as modified transudate, among other variables, due to the presence of red and inflammatory cells in the abdominal cavity. Regard of the cause, accumulation of fluid within the abdomen leads to additional fluid retention by the kidneys due to stimulatory effect on blood pressure hormones, firstly aldosterone. The sympathetic nervous system is also activated, and renin production is increased due to decreased perfusion of the kidney. Extreme disruption of the renal blood flow can lead to hepatorenal syndrome. Other complications of ascites include spontaneous bacterial peritonitis, due to decreased antibacterial factors in the ascitic fluid such as complement.
Thus, the ultrasonographic finding of liver congestion, pain in region of liver and ascites are the main signs of this disease presentation. Portal pressure increases and perfusion of the liver via portal vein is decreased. The combined effect of these changes in hepatic circulation on liver parenchyma is hypoxic damage of hepatocytes.
BCLS should be included in the list of differential diagnoses when animals present with: (1) Abrupt onset of ascites and painful hepatomegaly; (2) Massive ascites with relatively preserved liver functions; (3) Sinusoidal dilation in liver biopsy without heart disease; (4) Fulminant hepatic failure associated with hepatomegaly and ascites; (5) Unexplained chronic liver disease; (6) Hepatic thrombosis.
Liver biopsy exhibit marked hepatic congestion, liver cell waste and fibrosis predominantly located in the centrilobular area.1 The congestion can be seen in association with heart failure and/or restrictive pericardial disease. Liver biopsy is very important in differentiation of BCLS from veno-occlusive disease, which is characterized by nonthrombotic obstruction of hepatic venules by subendothelial swelling due to hurt of sinusoidal wall. Veno-occlusive disease could occurs also following administration of some toxic agents.13 Because obstruction of small hepatic veins without the involvement of large ones is included in the definition of BCLS, liver biopsy is fundamental for differentiation from veno-occlusive disease. Bone marrow biopsy is helpful for diagnosis of primary myeloproliferative disorder.14, 15
An odd feature of long-standing BCS is the development of multiple large regenerative nodules, some of them resembling chronic splenitis, as shown in Fig. 1 C. These nodules are a response to a focal loss of portal perfusion and hyperarterialization in areas with preserved hepatic or spleen vascularization.2, 16 This injury has been widely described in human patients with BCS, but has not yet been described in the veterinary literature. In our case, we found those lesions in the spleen (total of 17 nodules).
Conclusion
Although no data are available on incidence of this disease in veterinary medicine, there is no doubt that this is a very serious illness despite its rare appearance. To our knowledge, this is one of a few cases of lung adenocarcinoma associated with BCLS, yet no other case has been highlighted in the literature review.
Acknowledgements
This study was funded by grants from the National Agency for Scientific and Technological Promotion (Argentina) and Quilmes National University. G.A.H., D.F.A., D.E.G. are members of CONICET (Argentina). We also thank the valuable collaboration of Dr. Sergio Ferraris in the sonographic diagnosis of this case.
Abbreviations:
BCS: Budd-Chiari syndrome
BCLS: Budd-Chiari like syndrome
CVC: caudal vena cava
References
1. Aydinli, M. & Bayraktar, Y. (2007). “Budd-Chiari Syndrome: Etiology, Pathogenesis and Diagnosis,” World Journal of Gastroenterology 2007; 13(19):2693-2696.
Publisher – Google Scholar
2. Valla, D. C. (2003). “The Diagnosis and Management of the Budd-Chiari Syndrome: Consensus and Controversies,”Hepatology. 2003; 38:793-803.
Publisher – Google Scholar
3. van der Linde-Sipman, J. S. & Stokhof, A. A. (1974). “Triple Atria in a Pup,” Journal of The American Veterinary Medical Association. 1974; 165:539-541.
Publisher – Google Scholar
4. Stern, A., Fallon, R. K., Aronson, E. et al. (1986). “Cor Triatriatum Dexter in a Dog,” The Compendium on continuing education for the practicing veterinarian. 1986;8: 401-414.
Publisher – Google Scholar
5. Miller, M. W., Bonagura, J. D., Dibartola, S. P. et al. (1989). ‘Budd-Chiari Syndrome in Two Dogs,’ Journal of the American Animal Hospital Association. 1989; 25:277-283.
6. Tobias, A. H., Thomas, W. P., Kittleson, M. et al. (1993). “Cor Triatriatum Dexter in Two Dogs,” Journal of The American Veterinary Medical Association. 1993; 15:202(2):285-290.
Publisher – Google Scholar
7. Lombard, C. W. & Goldschmidt, M. H. (1980). “Primary Fibroma in the Right Atrium of a Dog,” Journal of Small Animal Practice. 1980; 21(8):439-448.
Publisher – Google Scholar
8. Atkins, C. E., badertscher, R. R., Greenlee, P. et al. (1982). ‘Diagnosis of Intracardiac Fibrosarcoma Using Two Dimensional Echocardiography,’ Journal of the American Animal Hospital Association. 1982; 20: 289-293.
9. Besso, J., Thollot, I. & Bretonc, C. (1993). ‘Un Casd’ascite Chez un Chien par Obstruction de la Venacave Caudale (Ascites in a Dog Due to Obstruction of the Caudal Vena Cava),’ Le Point Veterinaire. 1993; 25:59-66.
10. Schoeman, J. P. & Stidworthy, M. F. (2001). “Budd-Chiari-like Syndrome Associated with an Adrenal Phaeochromocytoma in a Dog,” Journal of Small Animal Practice. 2001; 42(4):191-194.
Publisher – Google Scholar
11. Langs, L. L. (2009). “Budd-Chiari-Like Syndrome in a Dog Due to Liver Lobe Entrapment within the Falciform Ligament,” Journal of the American Animal Hospital Association. 2009; 45(5):253-256.
Publisher – Google Scholar
12. Baig, M. A., Gemmill, T., Hammond, G. et al. (2006). “Budd-Chiari-Like Syndrome Caused by a Congenital Hiatal Hernia in a Shar-Pei Dog,” Veterinary Record. 2006; 159(10):322-323.
Publisher – Google Scholar
13. Gupta, S., Barter, S., Phillips, G. W. et al. (1987). “Comparison of Ultrasonography, Computed Tomography and 99mTc Liver Scan in Diagnosis of Budd-Chiari Syndrome,” Gut. 1987;28(3):242-247.
Publisher – Google Scholar
14. Anger, B. R., Seifried, E., Scheppach, J. et al. (1989). “Budd-Chiari Syndrome and Thrombosis of Other Abdominal Vessels in the Chronic Myeloproliferative Diseases,” Klinische Wochenschrift. 1989; 67:818-825.
Publisher – Google Scholar
15. De Stefano, V., Teofili, L., Leone, G. et al. (1997). “Spontaneous Erythroid Colony Formation as the Clue to an Underlying Myeloproliferative Disorder in Patients with Budd-Chiari Syndrome or Portal Vein Thrombosis,” Semin Thromb Hemost. 1997; 23(5):411-418.
Publisher – Google Scholar
16. Renzulli, M., Lucidi, V., Mosconi, C. et al. (2011). “Large Regenerative Nodules in a Patient with Budd-Chiari Syndrome after TIPS Positioning while on the Liver Transplantation List Diagnosed by Gd-EOB-DTPA MRI,” Hepatobiliary & Pancreatic Diseases International. 2011; 10(4):439-442.
Publisher – Google Scholar