Introduction
Good dental appearance is often equated with success in many social aspects, and an increased concern for dental appearance has been observed during adolescence (Shivakumar et al., 2009). Normal occlusion is essential for optimal oral function and the longevity of oro-dental health (Gauba et al., 1998).
Malocclusion has been described as a malrelationship between the maxillary and mandibular arches in any plane or a malposition of teeth beyond normal limits (Shivakumar et al., 2009; Tak et al., 2013). Although not life-threatening, it is the third most prevalent oral pathology, after tooth decay and periodontal disease, and therefore a public health priority (Tak et al., 2013). Those affected by malocclusion may experience a diminished self-image, affecting social and career opportunities (Cavalcanti et al., 2013; Shivakumar et al., 2009). Malocclusion has not been as thoroughly investigated as dental caries and periodontal disease, probably because the pain and misery caused by this disorder are seldom acute (Gauba et al., 1998; Shivakumar et al., 2009) but it has a greater impact on the individual in terms of social and functional limitations, psychological trauma (quality of life) and discomfort (Cavalcanti et al., 2013; Tak et al., 2013). Malocclusion affects oral health by leading to an increased prevalence of dental caries, and can cause gingival inflammation and temporomandibular joint disorders (Antunes et al., 2008; Shivakumar et al., 2009; Tak et al., 2013).
Assessment of orthodontic treatment need is a necessity for planning preventive and therapeutic orthodontic services for any population (Aikins et al., 2011; Ajayi, 2008; Tak et al., 2013).
The WHO has recommended the Dental Aesthetic Index (DAI) as a method of assessing dentofacial anomalies. The DAI, a cross-cultural index focused on socially defined dental aesthetics, is relatively simple, reproducible and valid, and a practical tool for screening orthodontic treatment need (Cavalcanti et al., 2013; Shivakumar et al., 2009; Tak et al., 2013).
Data are unavailable on prevalence of malocclusion (according to the DAI criteria) among high school students in Mangalore city. This study tries to fill that lacuna, and was carried out with the aim of assessing the prevalence of malocclusion and orthodontic treatment need among high school students in Mangalore city, Karnataka State, India.
Material and Methods
Subjects: A cross-sectional survey was conducted for a four-month period (November 2012 to February 2013). List of high schools in Mangalore city was obtained from the office of the Block Educational Officer, Mangalore City Range. The total number of schools numbered 70. From this list, four schools were selected by simple random sampling (lottery method). Permission to carry out the study was obtained from the Block Educational Officer, authorities in the selected schools and the Yenepoya University Ethics Committee.
Data Collection: A proforma was used to record demographic data (name of the student and school, age and gender) and the criteria of the DAI for each subject. In the selected high schools, all students who fulfilled the following inclusion criteria were examined: (a) male and female children present in school on the day of the survey, (b) with full complement of permanent teeth as per age, and (c) consenting to participate in the survey. Those who had undergone or were undergoing orthodontic treatment were excluded. Informed assent was obtained from all participants.
The subjects were examined by the investigator with the help of a recording clerk at their respective schools. Oral examinations were performed under adequate natural light using plane mouth mirrors and WHO Periodontal Probes, with subjects seated on chairs in classrooms or school corridors. The subjects were positioned to receive maximum illumination (sunlight) without any discomfort to the subject or investigator. The investigator underwent training, and calibration prior to the initiation of data collection and the kappa value for intra-examiner reliability were found to be 0.92.
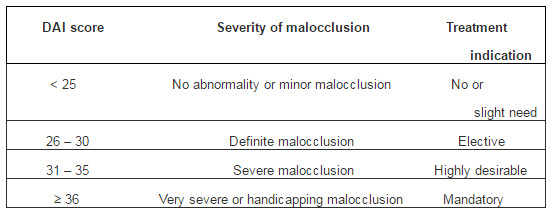
The DAI comprises the following components: missing anterior teeth, crowding and spacing in the incisal segments, diastema, largest anterior maxillary and mandibular irregularity, anterior maxillary and mandibular overjet, vertical anterior open bite, and antero-posterior molar relation. The standard DAI score is calculated using the regression equation: (missing visible teeth x 6) + crowding + spacing + (diastema x 3) + largest anterior maxillary irregularity + largest anterior mandibular irregularity + (anterior maxillary overjet x 2) + (anterior mandibular overjet x 4) + (vertical anterior open bite x 4) + (antero-posterior molar relation x 3) + 13 (WHO, 1997). Based on their DAI score, subjects were assigned to one of four categories suggesting an increasing grade of severity of malocclusion and the treatment indication as shown in Table 1.
Table 1: Distribution of Standard DAI Scores and the Treatment Indication
Statistical Analysis: Data were analyzed using the Statistical Package for Social Sciences (SPSS) Version 17.0 program for Windows. Descriptive statistics used included calculation of means and standard deviations. Differences in proportions between the different age groups and genders were compared using the Chi squared test, and a p-value of < 0.05 was considered statistically significant.
Results
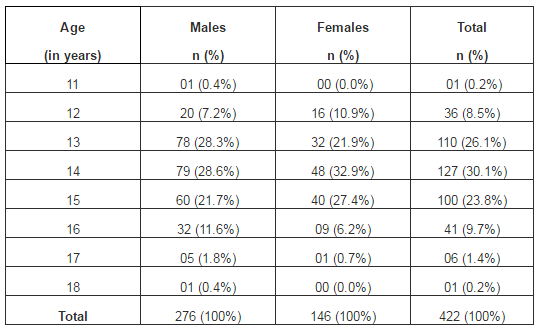
The total number of study subjects, who consented to participate and were examined, numbered 422. Twelve subjects had undergone or were undergoing orthodontic treatment and were excluded. They comprised 276 males (65.4%) and 146 females (34.6%), and ranged in age from 11 – 18 years (mean age 14.03 ± 1.19 years). Table 2 displays the distribution of study subjects based on age and gender.
Table 2: Distribution of the Study Subjects Based on Age and Gender
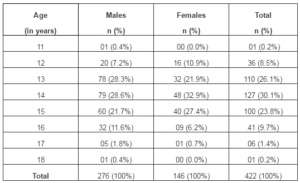
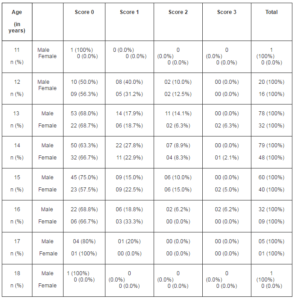
Table 3 shows the distribution of subjects according to their age, gender and DAI scores. Subjects with Scores 1, 2 and 3 were added together to calculate the prevalence of malocclusion for each age group. The prevalence of malocclusion was found to be as follows: 12 years – 47.2%, 13 years – 31.8%, 14 years – 35.4%, 15 years – 32.0%, 16 years – 31.7%, and 17 years – 16.7%. No significant differences were observed among the age groups with relation to the DAI scores (p = 0.551).
Table 3: Distribution of the Subjects According to Their Age, Gender and DAI Scores
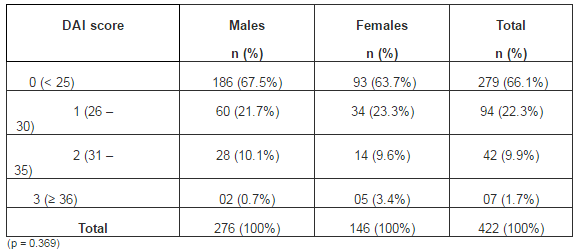
33.9% subjects presented with definite to very severe or handicapping malocclusion (Scores 1 to 3). The prevalence of malocclusion was found to be higher among females (36.3%) than males (32.5%). Overall distribution of subjects according to their gender and DAI scores is shown in Table 4.
Table 4: Distribution of the Subjects According to their Gender and DAI Scores
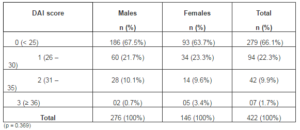
According to their DAI scores, the orthodontic treatment need of the study population was as follows: 66.1% subjects required little or no orthodontic treatment, while it was an elective option in 22.3% subjects; orthodontic treatment was highly desirable in the 9.9% presenting with severe malocclusion and mandatory in the 1.7% with very severe or handicapping malocclusion.
Discussion
With dental appearance, an increased concern among adolescents, malocclusion may impact the affected individuals by imposing social and functional limitations, psychological trauma and oral discomfort (Cavalcanti et al., 2013; Tak et al., 2013). Epidemiological data on disease prevalence are a prime requisite in planning health care for any population group. Data on the prevalence of malocclusion (according to the DAI criteria) among high school students in Mangalore city were unavailable. Therefore, this study was carried out to assess prevalence of malocclusion and orthodontic treatment need among high school students in Mangalore city, India.
The study population was larger than studied by Ahammed et al (2013) and Babu and Gopu (2011); however, Aikins et al (2011), Ajayi (2008), Cavalcanti et al (2013), Dacosta (1999), Gábris et al (2006) and Tak et al (2013) evaluated larger population groups. Since the schools surveyed were selected by random sampling, the results of this study have good external validity.
The male predominance seen in this study population was mirrored in studies carried out on similar age groups in India (Babu and Gopu., 2011; Shivakumar et al., 2009; Suma et al., 2011; Tak et al., 2013), Iran (Borzabadi-Farahani et al., 2011), Brazil (Cavalcanti et al., 2013) and Nigeria (Ajayi, 2008). In India, this male predominance in epidemiological studies can be attributed to the skewed sex ratio (Government of India, 2011). The epidemiological investigations carried out in Nigeria (Aikins et al., 2011; Dacosta, 1999) and Hungary (Gábris et al., 2006) reported higher number of female participants.
Definite to very severe or handicapping malocclusion (Scores 1 to 3) was present among 33.9% subjects. This finding was echoed by Gauba et al (1998) in their study on rural children in Ambala, India (29.2%) according to Angle’s classification system (1899) and Tak et al (2013) in 12-15-year-olds of Jaipur, India (33.3%) using the DAI. Surveys using the DAI criteria by Ahammed et al (2013) (16.4%), Borzabadi-Farahani et al (2011) (21.9%), Shivakumar et al (2009) (19.9%) and Suma et al (2011) (17.2%), found lower levels of malocclusion but Babu and Gopu (2011) (71.6%), Cavalcanti et al (2013) (58.1%) and Gábris et al (2006) (70.4%) found a higher prevalence. Studies carried out in Nigeria using the Angle’s classification by Ajayi (2008) and Dacosta (1999), and the ICON by Aikins et al (2011) have found 84.1%, 87.8% and 38.1% prevalence, respectively.
The prevalence of malocclusion was found to be higher among females (36.3%) than males (32.5%). Similar findings were reported by Gauba et al (1998) and Suma et al (2011), while Ahammed et al (2013), Aikins et al (2011), Borzabadi-Farahani et al (2011), Shivakumar et al (2009) and Tak et al (2013) reported higher malocclusion scores among male subjects. However, Borzabadi-Farahani et al (2011), Babu and Gopu (2011) and Cavalcanti et al (2013) found no correlation of treatment need with gender. As in this study, Shivakumar et al (2009) found that there were no significant differences in the DAI scores, either when evaluated for gender or age.
The surveys by Ahammed et al (2013), Aikins et al (2011) and Babu and Gopu (2011) found that the prevalence of malocclusion increased with age, while Tak et al (2013) reported a significant reduction in the severity of DAI scores with age. In this study, the prevalence of malocclusion in the different age groups ranged from 47.2% among 12-year-olds to 16.7% among 17-year-olds. The sole 11-year-old and 18-year-old male subjects presented with no orthodontic treatment need. Babu and Gopu (2011) found a prevalence of 67.5% among 13-year-olds, 76.3% among 14-year-olds and 84.6% among 15-year-olds, which was more than twice the values found in this investigation.
Study Limitations: Since this study was carried out to assess the prevalence of malocclusion and orthodontic treatment need (according to the DAI criteria) among high school students in Mangalore city about which data were unavailable, a limitation was that those who had undergone or were undergoing orthodontic treatment were excluded. This may lead to an underestimation of the actual treatment need of the population being studied.
The authors anticipate that this survey will pave the way for a large-scale epidemiological study to validate the findings and provide a clear picture of the existing situation. This data will also help oral health care professionals plan and execute appropriate measures, such as dental screening, education and treatment programs, to overcome this oral condition.
Conclusion
Malocclusion and orthodontic treatment need were found to be present in 33.9% of the population surveyed. The prevalence of malocclusion was found to decrease with age.
References
Ahammed, A. R. Y., Shetty, V., Panda, A. K., Gunda, S., Pradhan, D., Husain, N. & Gugwad, S. (2013). “Prevalence of Malocclusion among 12 to 15 Years Age Group Orphan Children Using Dental Aesthetic Index,” Journal of Contemporary Dental Practice, 14 (1) 111-114.
Publisher – Google Scholar
Aikins, E. A., Dacosta, O. O., Onyeaso, C. O. & Isiekwe, M. C. (2011). “Orthodontic Treatment Need and Complexity among Nigerian Adolescents in Rivers State, Nigeria,” International Journal of Dentistry, Article ID 813525.
Publisher – Google Scholar
Ajayi, E. O. (2008). “Prevalence of Malocclusion among School Children in Benin City, Nigeria,” Journal of Medicine and Biomedical Research, 7 (1&2) 58-65.
Publisher – Google Scholar
Antunes, J. L., Peres, M. A., Frias, A. C., Crosato, E. M. & Biazevic, M. G. (2008). “Gingival Health of Adolescents and the Utilization of Dental Services, State of São Paulo, Brazil,” Revista de Saúde Pública, 42 (2) 191-199.
Publisher – Google Scholar
Babu, V. & Gopu, H. (2011). “Assessment of Orthodontic Treatment Needs according to Dental Aesthetic Index,” Journal of Dental Sciences and Research, 2 (2) 1-5.
Publisher – Google Scholar
Borzabadi-Farahani, A., Eslamipour, F. & Asgari, I. (2011). “Association between Orthodontic Treatment Need and Caries Experience,” Acta Odontologica Scandinavica, 69 2-11.
Publisher – Google Scholar
Cavalcanti, A. L., Dos Santos, J. A., Aguiar, Y. P. C., Xavier, A. F. C. & Moura, C. (2013). “Prevalence and Severity of Malocclusion in Brazilian Adolescents Using the Dental Aesthetic Index (DAI),” Pakistan Oral & Dental Journal, 33 (3) 473-479.
Publisher
‘Census of India, 2011,’ Ministry of Home Affairs, Government of India. [31/12/2013] Available: http://censusindia.gov.in/Data_Products/Library/ Provisional_Population_Total_ link /PDF_Links/chapter6.pdf
Dacosta, O. O. (1999). “The Prevalence of Malocclusion among a Population of Northern Nigeria School Children,” West African Journal of Medicine, 18 (2) 91-96.
Publisher – Google Scholar
Dental Council of India. (2004). ‘National Oral Health Survey & Fluoride Mapping 2002-2003 Karnataka,’ New Delhi, India.
Gábris, K., Márton, S. & Madléna, M. (2006). “Prevalence of Malocclusions in Hungarian Adolescents,” The European Journal of Orthodontics, 28 (5) 467-470.
Publisher – Google Scholar
Gauba, K., Ashima, G., Tewari, A. & Utreja, A. (1998). “Prevalence of Malocclusion and abnormal Oral Habits in North Indian Rural Children,” Journal of the Indian Society of Pedodontics and Preventive Dentistry, 16 (1) 26-30.
Publisher – Google Scholar
Shivakumar, K. M., Chandu, G. N., Reddy, V. V. S. & Shafiulla, M. D. (2009). “Prevalence of Malocclusion and Orthodontic Treatment Needs among Middle and High School Children of Davangere City, India by Using Dental Aesthetic Index,” Journal of the Indian Society of Pedodontics and Preventive Dentistry, 27 (4) 211-218.
Publisher – Google Scholar
Suma, S., Chandra Shekar, B. R. & Manjunath, B. C. (2011). “Assessment of Malocclusion Status in Relation to Area of Residence among 15 Year Old School Children Using Dental Aesthetic Index,” International Journal of Dental Clinics, 3 (2) 14-17.
Publisher – Google Scholar
Tak, M., Nagarajappa, R., Sharda, A. J., Asawa, K., Tak, A., Jalihal, S. & Kakatkar G. (2013). “Prevalence of Malocclusion and Orthodontic Treatment Needs among 12-15 Years Old School Children of Udaipur, India,” European Journal of Dentistry, 7 45-53.
Publisher – Google Scholar
World Health Organization. (1997). ‘Oral Health Surveys: Basic Methods,’ 4th ed. Geneva, Switzerland.
Google Scholar