Introduction
Chronic lumbalgies are a heterogeneous group of disorders, which main clinical features include recurrent low back pain lasting longer than 3 months.
Today’s recommendations for the treatment of patients with chronic Lumbalgia undergo important changes generally expressed in terms of transition from passive to active treatment. Often these patients are subjected to a multidisciplinary treatment with application of a bio-psycho-social approach, which can prevent chronicity by providing rehabilitation to patients with persistent pain after the acute phase (Khalfaoui et al. 2013).
The concept of “functional rehabilitation program” in the context of chronic Lumbalgia, was introduced in the United States 20 years ago as a specific response to frequent absenteeism and disability, which are consequences of work-related spinal injuries. (Richardson & Jull 1995; Videman et al. 1995; White 1991).
Given the social importance of this disease, for the first time in Bulgaria, there was carried out a prospective study of the trunk muscle flexion capabilities, before and after application of a kinesitherapeutic program of special exercises at home in patients with chronic Lumbalgia .
Aim of the Study
The aim of this study, is to take into account the effect of a kinesitherapeutic program of special exercises for treatment of endurance of the flexor trunk muscles in patients with chronic Lumbalgia.
Patients and Methods
The study is representative, prospective, parallel one, with test-retest design and tracking with filling out questionnaires at the beginning and end of the observation (12 months). It was carried out with the participation of a representative sample of 110 patients with chronic Lumbalgia, distributed equally into two treatment groups (experimental and control) of uniform age and gender. The allocation to the control or treatment group, was based on randomization after a consultation at the counseling center in Stambolijski in cases inclusion criteria were met. They were each diagnosed and were undergoing therapy at the time, having been referred to the center by a general practitioner after consultation with a neurologist.
The study was conducted after the approval of the Local Ethics Commission at the University of Medicine, Plovdiv on April 8th 2009. All study procedures were performed in accordance with the guidelines of good clinical practices. Prior to procedures, each patient was familiarized with the design of the study, and signed an informed consent form.
The following inclusion criteria for the study were used: a signed informed consent, age 30 to 60 years; presence of X-ray of the lumbar spine and consultation with a neurologist; diagnosed chronic Lumbalgia; lack of a herniated disc, tumor, trauma, inflammation of the spine and osteoporosis, etiologically related to Lumbalgia; lack of focal neurological deficit – motor, sensory, urinary and bowel problems; lack of accompanying psychiatric disorders with a view to a better cooperation. 135 consecutive patients with chronic Lumbalgia were initially screened, 25 of which were not included in the survey due to non-compliance with the inclusion criteria. Of 110 patients included in the final stage of the study, a total of 51 patients dropped out (22 of the experimental group due to a temporary improvement or social commitments, and 29 in the control group due to lack of motivation).
Patient information was obtained by taking a history and focused review of available medical records of the therapist and neurologist. The main causes of chronic Lumbalgia in our study participants were: chronic lumbar strain (in 45.45%), spondylosis (31.82%), and lumbar discopathy (22.73%). The experimental group was trained to perform special exercises 3 times a week at home, and participants in the control group followed the recommendations of a physician for medical treatment. The participants in both groups used Diclofenac gel or Voltaren gel in cases the pain became more intense. Patients’ follow-up lasted for a year. At the beginning and end of the study, there were applied Visual Analog Scale (VAS) and Shirado-Ito test.
The isometric Shirado-Ito test assesses the isometric endurance of abdominal musculature (Ito et al. 1996). Its high test-retest reliability (Ito et al. 1996) and validity (Müller et al. 2010) have been proved. It consists of lifting the upper body while lying supine, the arms crossed, the legs flexed 90° in hip and knee joints, and the neck flexed as much as possible. The time for holding this position is measured by a chronometer and recorded in seconds. The test is terminated when the fixed position cannot be held longer or if there is pain.
Our task was to achieve functional restoration of the spinal column with the help of the kinesitherapeutic program by restoring the aspects of muscle functions motor control, and optimizing patients’ functional capabilities, after pain and disability reduction.
In the training course we advised the patients:
- To do all exercises from a comfort position of the spinal column;
- To do the mobility improving exercises with amplitude limitations and without loading;
- To do the trunk flexion from supine position after expiration, and with maintaining the neutral lumbar lordosis;
- To increase the dose of analytical exercises by one movement every day up to eight repetitions, with maintaining an isometric regime.
The kinesitherapeutic program applied in patients with chronic Lumbalgia in the experimental group included five types of training:
- Training for lumbar stability: elevation of the pelvis to maintain neutral position, axial withdrawal during co-contraction, maintaining co-contraction with elevation of one foot and abduction of the upper limb, bending the trunk forward while maintaining a neutral lumbar position, moving from sitting into an upright position while maintaining neutral lumbar position.
- Training for mobility: suppling in flexion position, suppling in extensional position, axial withdrawal from a bent knee position, abductor muscle active tension, adductor muscle active tension, active tension of the ischiocrural muscle group.
- Flexor workout: exercise for strengthening the abdominal muscles from side leg position as well as exercise for co-contraction m.obliquus abdominis externus, m.obliquus abdominis internus, m.transversus abdominis and m.quadratus lumborum with lateral support with bent knees, co-contraction training for the anterior oblique system involving the anterior abdominal fascia, placed under tension, stabilizing the sacroiliac joint by tension m.obliquus abdominis externus, m.obliquus abdominis internus, and the opposite adductors of the hip; dynamic workout m.obliquus abdominis externus, m.obliquus abdominis internus and adductor of the hip; dynamic strength training m.obliquus abdominis externus and m.obliquus abdominis internus.
- Extensors workout: exercises for extension of the spine from a prone position with hands support and holding for 30 sec. in extensional position; strength training of the gluteal muscles from a prone position, co-contraction for strength of m.gluteus maximus and m.latissimus dorsi.
- Training for sensory-motor reprogramming: exercises for the trunk rotators with abduction of the upper limb, to improve the stabilizing function of the spine from its original seating position on a Swiss-ball; exercises for upper limb flexion, and extension of homolateral lower limbs from side leg position on a Swiss-ball for improving the proprioception of the spinal column structures, exercises to maintain the neutral position by moving the Swiss-ball on the wall.
Monitoring and evaluation of the results of kinesitherapeutic program, was carried out by an experienced physiotherapist who was blinded to the information about the patient allocation to the experimental or control group.
The collected primary information was checked, encoded, and entered into a computer database for statistical analysis. Data were processed using SPSS 13.0. Results for quantitative variables (age, pain intensity, and endurance) were expressed as mean ± SE (Standard Error) and results for qualitative variables (gender, risk factors) as percentages. Age, gender, risk factors, as well as the assessments of the VAS, and Shirado-Ito test were compared by means of Pearson’s correlation coefficient (r ), c2 – test, t – test, u – test, and Fisher’s criterion (F) were used to analyze the correlation between age, gender, risk factors, pain intensity, and the assessments of Shirado-Ito test. Multiple regression analysis was applied to estimate the simultaneous impact of age, gender, risk factors, and pain intensity on the Shirado-Ito test results. The level of significance was set at P < 0.05.
Results
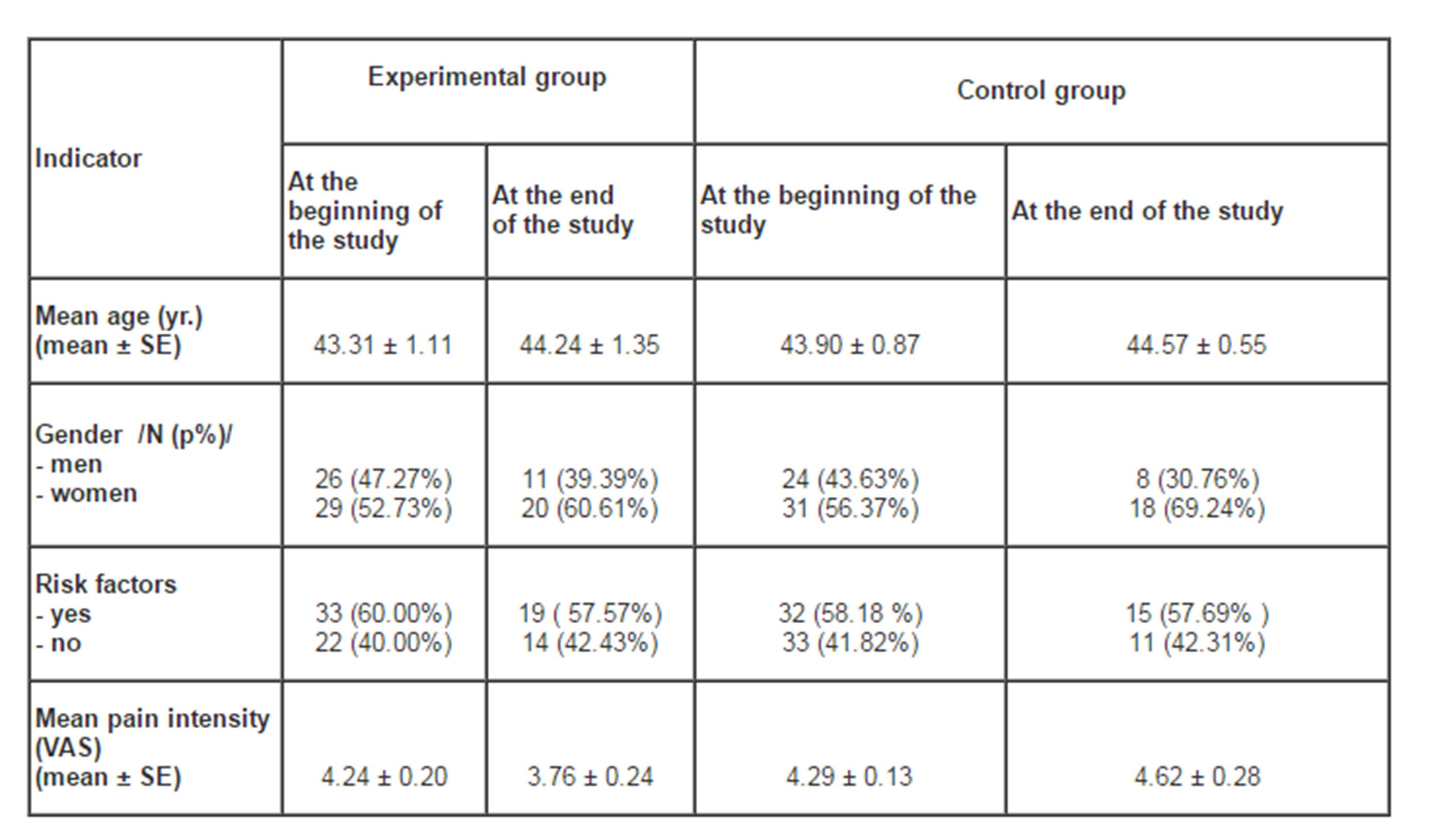
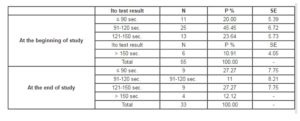
Table 1 shows the characteristics of the individuals in the two groups in terms of age, gender, pre-existing risk factors for chronic Lumbalgia, and mean pain intensity. The described risk factors include: strenuous physical activity, repetitive motion with rotations of the body, spinal column burdening in upright and seated position, being overweight.
Table 1: Age, gender, presence of risk factors and mean pain intensity in patients from the experimental and control groups at the beginning and end of the study
At the beginning of the study there were ascertained no significant differences between the participants in the experimental and control groups in terms of mean age P > 0.05 (u = 0.41), gender P > 0.05 (ï£2 = 0.15) and present risk factors, P > 0.05 (ï£2 = 0.04). No correlation was found between the participants’ gender, and the presence of risk factors P > 0.05 (ï£2 = 3.51) as well as between age and the presence of risk factors P > 0.05 (ï£2 = 2.81).
There was ascertained no statistically significant difference in the experimental group between the Ito test results at the beginning and end of the study P > 0.05 (u = 0.75) — Table 2. However, these results show a certain positive effect in the reduction of complaints.
Table 2: Comparison of Ito test results from the experimental group at the beginning
and end of the study
The control group test results show a statistically significant difference between the beginning and end of the study P < 0.05 (u = 2.05). The mean endurance is decreased from 110.81 ± 6.33 sec. to 106.62 ± 5.20 sec. which is also in support of the positive effect of the kinesitherapeutic program.
At the end of study the mean endurance of patients in the experimental group is 112.91 ± 6.12 sec., and of participants in the control group — 106.62 ± 5.20 sec. No statistically significant difference was found between either group at the end of the study Ð > 0.05 (u = 0.78).
The experimental group results obtained at
the beginning of the study are closely dependent on: pain intensity P < 0.001 (r = -0.83), presence of risk factors P < 0.001 (r
= -0.42), and age P < 0.001 (r = -0.43). At the end of the study the experimental group results are closely dependent on: pain intensity P < 0.001 (r = -0.65), presence of risk factors P < 0.01 (r = -0.47), age P < 0.01 (r = -0.44), and gender of study participants P < 0.05 (r = +0.40).
A comparison by gender with the mean Ito test results in the experimental group at the beginning of the study, showed no significant results between men and women P > 0.05. A comparison by gender with the mean Ito test results in the experimental group at the end of the study, showed that men (124.05 ± 7.12 sec.) endure longer periods compared to women (95.77 ± 9.49 sec.) Ð < 0.05 (u = 2.42).
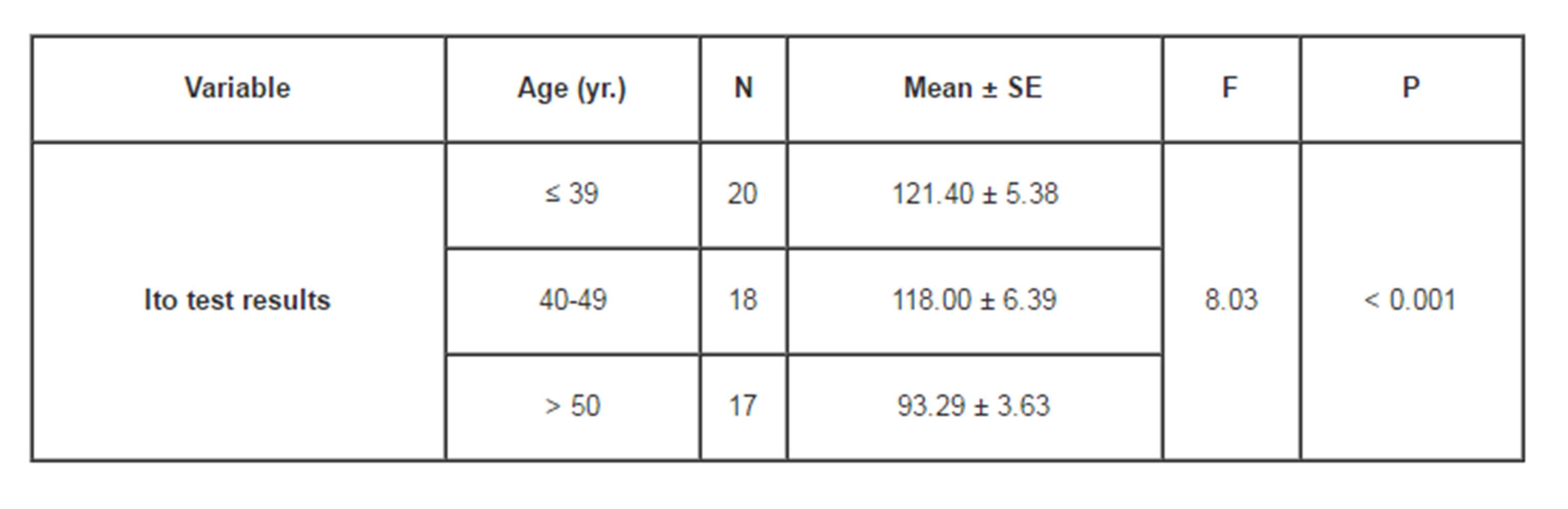
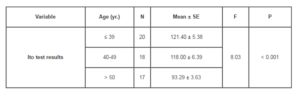
The comparison by age with the Ito mean test results, in the experimental group, demonstrated that patients over 50 years of age had a much lower endurance at the beginning of study P < 0.01 (r = -0.34) – Table 3.
Table 3: Comparison of the mean Ito test results by age from the experimental group at the beginning of the study
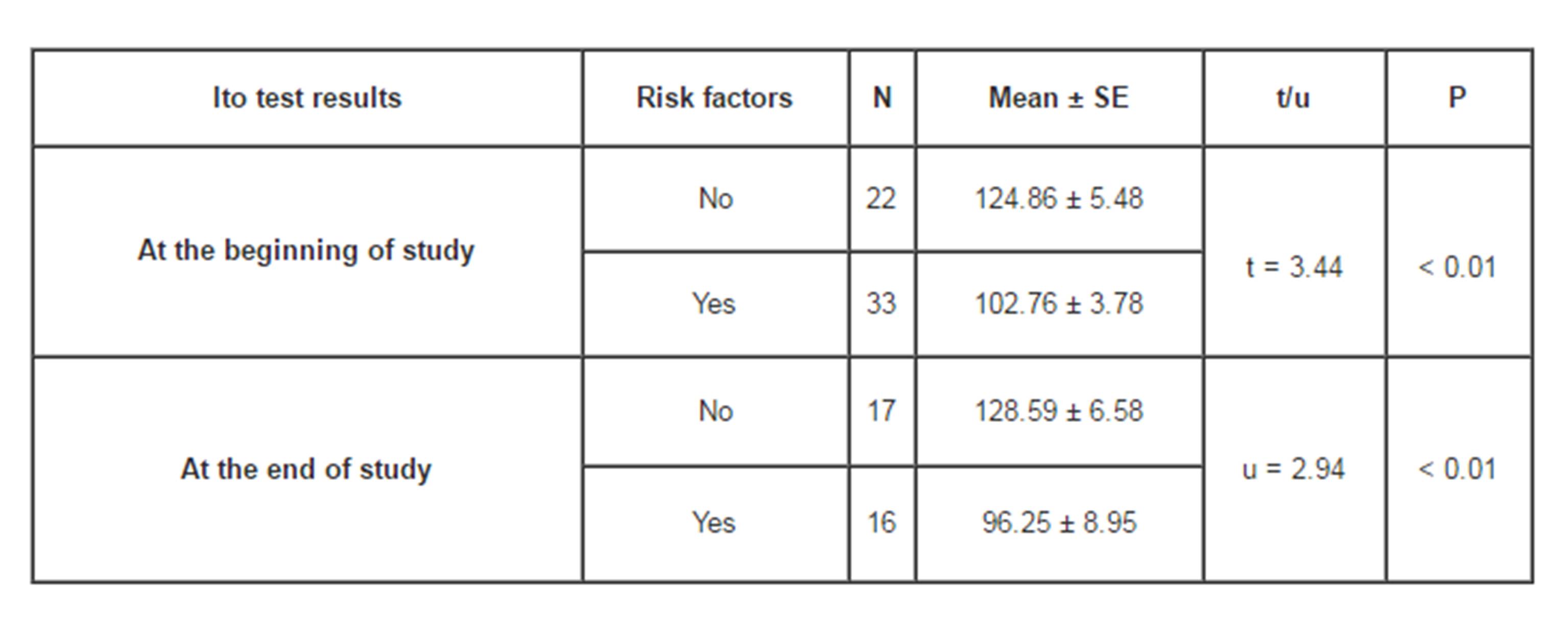
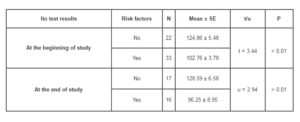
The comparison of the presence of risk factors for chronic Lumbalgia with the Ito mean test results in the experimental group, showed that in the presence of risk factors, patients endured less time at the beginning and end of the study P < 0.01 (Table 4).
Table 4: Comparison of the mean Ito test results by the presence of risk factors from the experimental group at the beginning and end of the study
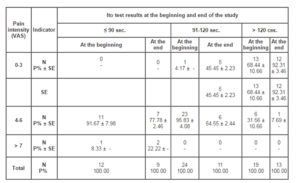
Pain intensity influenced the Ito test results of the patients in the experimental group at the beginning and end of the study, while patients with severe pain had reduced endurance of the trunk flexors P < 0.001 (r = -0.65) – Table 5.
Table 5: Ito test results of patients from the experimental group at the beginning and end of the study according to pain intensity by VAS
The multiple stepwise regression at the beginning of the observation showed that in simultaneous presence in the model of all the above factors (pain intensity, age, gender and risk factors), the most significant effect for the Ito test results was exerted by pain intensity, gender and age of the experimental group P < 0.001 (F = 64.98). These three factors explained 79% of the variation of the results. Similar results were seen with the same analysis at the end of the study P <0.001 (F = 20.47), when these three factors explained 68% of the variation of the results.
Discussion
Conflicting results from different studies on the effectiveness of kinesitherapeutic programs (incl. in comparison with physiotherapy) in patients with chronic Lumbalgia; indicate the need for further studies to evaluate the effect of combined exercise in these patients, and to clarify the role of many factors contributing to this pathology (Calmels et al. 2004) . The aim of our study was to gauge the effect of a kinesitherapeutic program of special exercises, in order to influence the endurance of trunk muscle flexion in patients with chronic Lumbalgia. In the analysis of the initial and final Ito test results in the experimental group, we found no statistically significant difference, but we did find some positive effect, evidenced by the reduction in complaints. In the control group, the median endurance decreased from 110.81 sec. to 106.62 seconds, which supports the favorable role of the kinesitherapeutic program applied in the experimental group. It includes training for endurance through flexion exercises from occipital leg position with detached blades, lateral flexion and extension exercises, working for the muscles of obliquus anterior, posterior and lateral pneumatic system. We find in the literature confirmation of the positive effect of this practice in a study by Hides et al. 2001, which compares the two groups of patients with chronic Lumbalgia, probing mm. multifidi by ultrasound. The first group of patients is placed on a bed at rest for three days, and then is subjected to a combination of drug therapy and exercise. The second group comprises people who perform training for endurance, and work out to maintain isometric co-contraction of the m. transversus abdominis and mm. multifidi at small degrees of voluntary muscle contraction, keeping the position of the neutral lordosis. Co-contraction of m. transversus abdominis and mm. multifidi is maintained during the exercises for lower limbs. Four weeks into the treatment, the researchers found a rapid and complete recovery of muscle mm. multifidi in the second group (Hides et al. 2001). Cavarec and Cantenot 2013 have also achieved endurance enhancement of the trunk flexor muscles, after a program of isometric exercises with swissball and lumbar lordosis maintenance (Cavarec and Cantenot 2013). According to McGill 1998, the best choice for abdominal exercises in the phase of active rehabilitation exercises is the occipital leg position with detached blades with free feet. This position lends itself best to training abdominal muscles, and doing the obliquus. The lateral support position with bent knees is to train the abdominal wall (m. obliquus abdominis internus, m. obliquus abdominis externus, m. transversus abdominis and m. quadratus lumborum) with minimal compression of the spine. Occipital leg position with detached blades with dynamic crossing is the only position adapted to train the obliquus (McGill 1998). For training the lateral abdominal muscles, Nachemson recommends isometric training and occipital leg position with detached blades with dynamic crossing with maintenance of isometrics of 5-10 seconds. When the patient gets stronger, the number of repetitions and the duration of the isometric mode can be increased (Nachemson 1970; Nachemson 1992).
The results obtained in the experimental group of our study are closely dependent on the intensity of pain, age, presence of risk factors and the sex of the test subjects at the beginning and end of the observation, as the correlation for the first three indices is reversed, greater on the first variable and moderate for the next three. In multiple stepwise regression analysis, we show that the results of the test are formed under the complex influence of pain intensity, age and sex of participants, as the model explains about 79 % of the variability of the results in early testing, and 68% of the variation in the end testing.
The pain intensity influences the results of Ito test patients from the experimental group, as the number of those with less severe, pain in the retention time of flexion of the body is significantly reduced as compared to that of subjects with less painful symptoms. In support of this assertion we can refer to the study of Arokoski et al. 2004, in which, through a bilateral EMG level L5 paraspinal muscles m. rectus abdominis and m. obliquus externus, the authors demonstrate that patients show different patterns of activity of the body muscles in different painful symptomatology, while trunk flexion is significantly reduced during the period of increased pain intensity. The registered signal is averaged and normalized to the maximum EMG amplitude obtained at maximal voluntary muscle contraction (Arokoski et al. 2004).
When examining the correlation between age and Ito test results, we found that patients over the age of 50 stay less time in trunk flexion. This is due to the fact that, with advancing age, there are structural and morphological changes that occur in all organ systems. In the literature we find no studies to support our conclusion.
In comparing the presence of risk factors to the Ito average test results in the experimental group, we show that in the presence of risk factors, patients endure less time at the beginning and end of the observation. Therefore, the presence of risk factors is very important to keep the flexion position of the spine. In his study, Kirkaldy-Willis defines the various psycho-social factors, and concluded that risk factors do not act in isolation, but in a complex that is crucial for the approach to long-term reduction of pain in the waist and groin (Kirkaldy-Willis 1982).
At the beginning of the observation we found no significant difference in the results when compared by gender, but at the end of the observation we ascertained that men endured longer – an average of 124 seconds. In the literature we find evidence of a relationship between gender and flexion endurance of the body in patients with chronic Lumbalgia. Ito et al. point close to the obtained results in men after administration of a kinesitherapeutic program (Ito et al. 1996).
Limitations of the Study
The limitations of our study refer to the reduced number of participants, and the relatively large number of patients who did not complete the tests. Another limitation was that the participants were only from Plovdiv. However, these limitations do not downplay the results of the first such study in Bulgaria. There are forthcoming studies with a larger number of patients with chronic Lumbalgia from different regions of Bulgaria.
Conclusion
The application of specific exercises in patients with chronic Lumbalgia, proved useful with the information obtained to effectively recover aspects of motor control. The reported positive effect of the administered kinesitherapeutic program consists of improved muscle flexion capabilities of the body. Non-implementation of such a program is associated with worsening of the functional status of patients. Our results motivate the introduction and implementation of the described kinesitherapeutic program in the clinical practice in Bulgaria to improve the quality of life, and reduce disability in people with chronic Lumbalgia.
References
1. Arokoski, J.P., Valta, T., Kankaanpää, M. and Airaksinen, O. (2004) “Activation of lumbar paraspinal and abdominal muscles during therapeutic exercises in chronic low back pain patients”, Arch Phys Med Rehabil., 85(5) 823-32.
Publisher – Google Scholar
2. Calmels P., Jacob J.F., Fayolle-Minon I., Charles C., Bouchet J.P., Rimaud D. and Thomas T. (2004) “Use of isokinetic techniques vs standard physiotherapy in patients with chronic low back pain. Preliminary results”, Ann Readapt Med Phys., 47(1) 20-7.
Publisher – Google Scholar
3. Cavarec, F. and Cantenot G. (2013) “Three methods for trunk muscles isometric musculation: A comparative study”. Kinésitherapie, la Revue, 13(135) 41-48.
4. Hides, J., Jull, G. and Richardson C. (2001) “Long-term effects of specific stabilizing exercises for first episode low back pain”, Spine, 26(11) e243-e248.
Publisher – Google Scholar
5. Ito, T., Shirado, O., Suzuki, H., Takahashi M., Kaneda K. and Strax T.E. (1996) “Lumbar trunk muscle endurance testing: an inex¬pensive alternative to exercise program evaluation”, Arch Phys Med Rehabil., 77(1) 75-79.
Publisher – Google Scholar
6. Khalfaoui, S., Mounach, A., Arabi, H., Ismaili, S.A., Menabbou, M., Jemmouj, A., Tricha, M., Taouli, N., El Abbassi, E.M. (2013) “Place des différentes méthodes de rééducation dans la prise en charge de la lombalgie commune chronique”, Rev Mar Rhum, 24, 32-38.
Google Scholar
7. Kirkaldy-Willis, W. (1982) “Instability of the lumbar spine”, Clin. Orthop., (165) 110-123.
Google Scholar
8. McGill, S. (1998) “Low back exercises: evidence for improving exercise regimens”, Phys. Ther., 78(7) 754-765.
Google Scholar
9. Müller, R., Strässle, K. and Wirth, B. (2010) “Isometric Abdominal Muscle Endurance: an EMG Study on the Criterion Validity of the Ito Test”, J Electromyogr Kinesiol., 20(5) 845-850.
Publisher – Google Scholar
10. Nachemson, A. (1970) “The lumbar spine: an orthopaedic challenge”, Spine, 1 (48) 59-71.
11. Nachemson, A. (1992) “Newest knowledge of low back pain: a critical look”, Clin. Orthop Relat Res., (279) 8-20.
Google Scholar
12. Richardson, C. and Jull, G. (1995) “Muscle control-pain control.What exercises would you pres-cribe?”, Man. Ther., 1(1) 225-312.
Publisher – Google Scholar
13. Videman, T., Sarna, S. and Bathe, M. (1995) “The long-term effects of physical loading and exercise lifestyles on back-related symptoms, disability and spinal pathology among men”, Spine, 20(6) 699-709.
Publisher – Google Scholar
14. White, A. (1991) Stabilization of the lumbar spine. In White, A., Anderson, R (2001) Conservative care of low back pain. Baltimore, Williams & Wilkins, Kine-actualite, 41, 78-85.