An epidural block is useful to decrease anesthetics and analgesics during surgery and to decrease postoperative pain; both have a great benefit on postoperative respiratory function in obese patients (von Ungern-Sternberg, et al, 2005). Postoperative epidural analgesia was associated with a decrease in left ventricular stroke work, systolic pressure-heart rate product, arteriovenoses oxygen content differences, and oxygen consumption, compared with values observed when patients experienced pain without epidural analgesia (Gelman, et al, 1980). Therefore, an epidural block should be used in bariatric surgery.
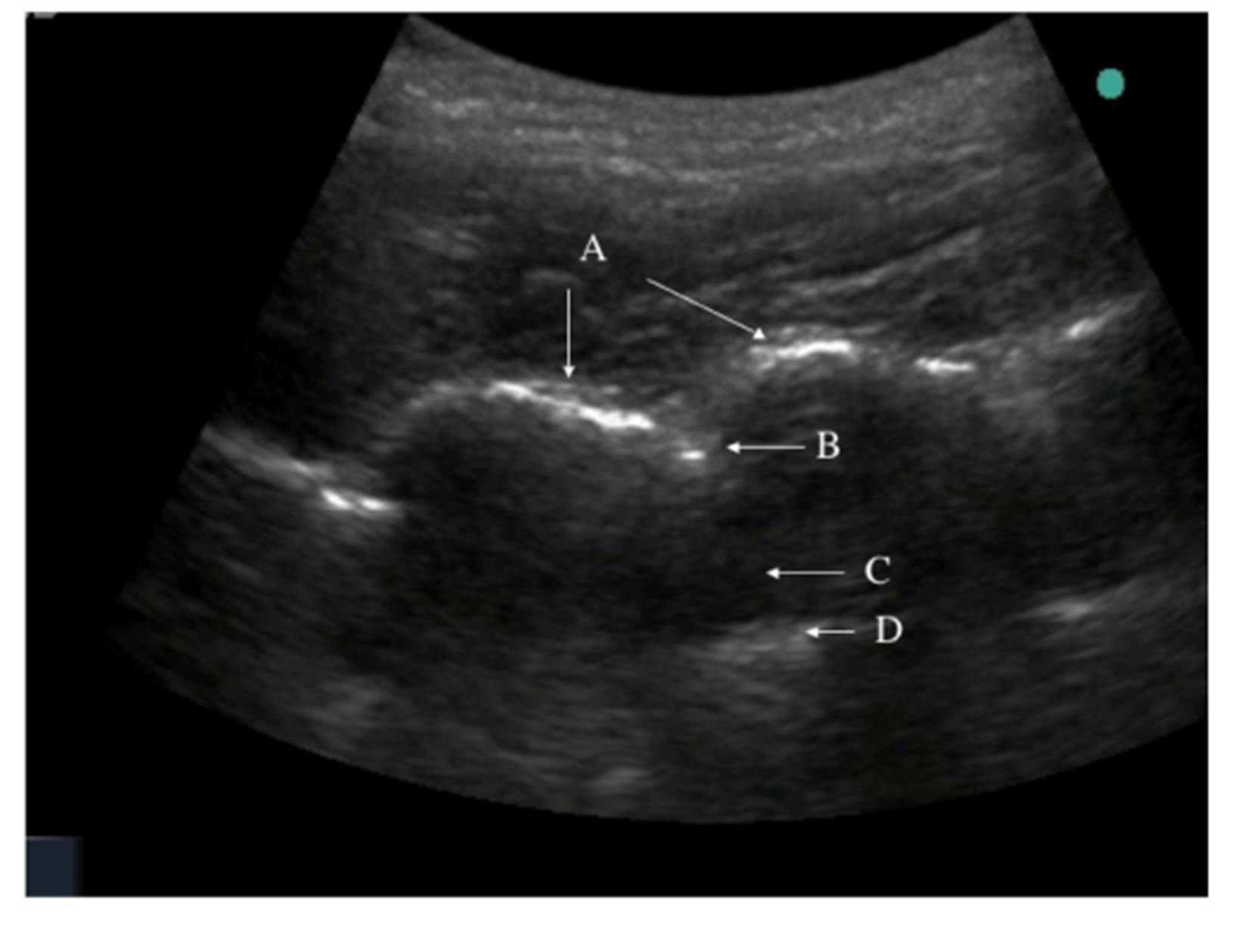
We successfully inserted an epidural catheter in all 16 bariatric patients using ultrasound. It was quite difficult to recognize spinous process manually; therefore, we used ultrasound to locate the spinous process and dura. Balki et al (2009) suggested that pre-puncture ultrasound might be useful to facilitate the placement of epidural needles in obese patients.
The success rate of epidural puncture at the first attempt was 63.3 % in obese parturients with BMI of 34.9 kg/m2, and needle depth of 6.48 cm in the study by Qian et al (2012). Our success rate at the first attempt was 14/16 (87.5 %) with mean BMI of 45.5 kg/m2 and needle depth of 9.1 cm. The lower success rate of the study by Qian et al. might be because their patients were pregnant.
Ultrasound depth may be 14% shorter to 17% longer than the needle depth in the study by Sahota et al (2013). However, Rasoulian et al. reported that the ultrasound depth tended to underestimate the needle depth as shown by the bias of 3.21 mm, perhaps due to tissue compression by the probe or the intrinsic thickness of the ligamentum flavum (Rasoulian, et al, 2011). Tran et al. (2009) also reported that the bias between the needle depth and ultrasound depth (4.8 mm) could be attributed to the thickness of the ligamentum flavum (typically 5 mm). The blunt Tuohy needle generates high pressure during passage through tissue (max. 180 mmHg), especially in the ligamentum flavum (> 400 mmHg) (Grau, et al, 2001). This can cause a tissue deformation, which accounts for a difference between the needle depth and ultrasound depth. Our study showed that the corrected ultrasound depth was shorter about 0.8 to 2.5 cm than the needle depth, which was a greater difference than other studies (Grau, et al, 2001; Rasoulian, et al, 2011; Sahota, et al, 2013; Tran, et al, 2009). We measured the depth to the ligamentum flavum, which had 3 to 5 mm thickness, and we might compress the probe to get clearer view than other studies because we had more obese patients. These might be the reason of our greater difference between the needle depth and ultrasound depth compared to other studies (Grau, et al, 2001; Rasoulian, et al, 2011; Sahota, et al, 2013; Tran, et al, 2009).
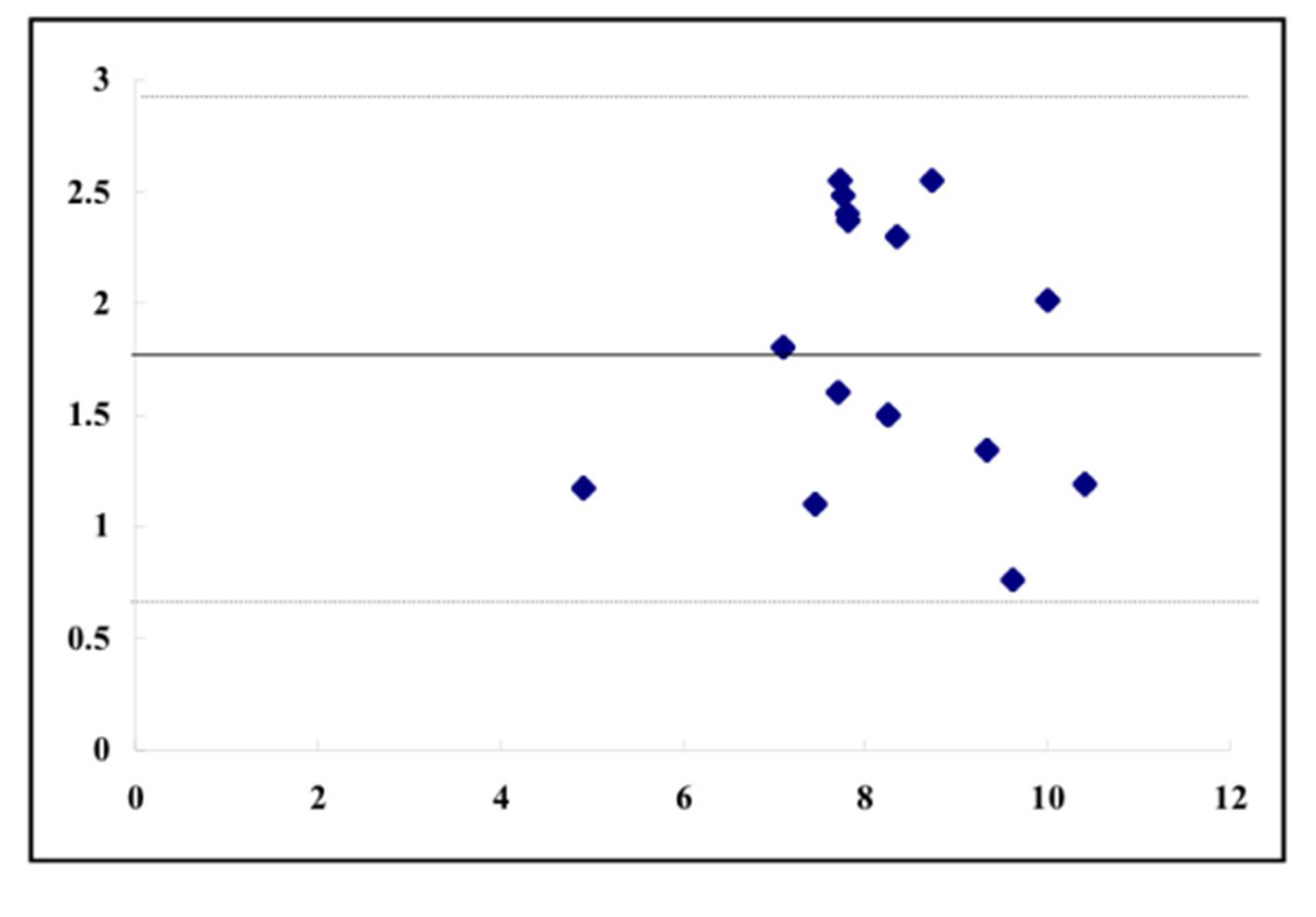
Balki et al. (2009) showed that in obese parturients, ultrasound depth and needle depth of the lumbar epidural had a strong correlation with the Pearson correlation coefficient of 0.85 and concordance correlation coefficient of 0.79. The needle depth was 6.6 ± 1.0 cm and ultrasound depth was 6.3 ± 0.8 cm in their study. Ultrasound depth is highly correlated to the needle depth observed during lumbar epidural placement (Tran, et al, 2009), while it is considered that the discussion is still necessary for thoracic epidural placement. Rasoulian et al. (2011) reported that during thoracic epidural catheterization, the limits of agreement are wide, which limits the predictive value of ultrasound-based measurements. Our study showed r2 value 0.81 and bias 1.8 cm with limits of agreements 0.63 cm and 2.94 cm when corrected ultrasound depth was used. Therefore, the ultrasound depth could not be a surrogate measurement of the needle depth.
In conclusion, ultrasound was useful to insert a thoracic epidural catheter in obese patients receiving bariatric surgery, but ultrasound measurement of the depth to an epidural space could be used to know the needle insertion depth.
Acknowledgements
We used no fund in this clinical study and have no conflict of interest.
References
1. Adams, J.P., & Murphy, P.G. (2000). “Obesity in anaesthesia and intensive care,” British Journal of Anaesthesia, 85 (1) 91-108.
Publisher – Google Scholar.
2. Balki, M., Lee, Y., Halpern, S., et al. (2009). “Ultrasound imaging of the lumbar spine in the transverse plane: The correlation between estimated and actual depth to the epidural space in obese parturients,” Anesthesia & Analgesia 108 (6) 1876-1881.
Publisher – Google Scholar.
3. Gelman, S., Laws, H.L., Potzick, J., et al. (1980). “Thoracic epidural vs balanced anesthesia in morbid obesity: An intraoperative and postoperative hemodynamic study,” Anesthesia & Analgesia, 59 (12) 902-908.
Publisher – Google Scholar.
4. Grau, T., Leipold, R.W., Conradi, R., et al. (2001). “Ultrasound control for presumed difficult epidural puncture,” Acta Anaesthesiologica Scandinavica, 45 (6) 766-771.
Publisher – Google Scholar.
5. Nishiyama, T., Kohno, Y., & Koishi, K. (2012). “Anesthesia for bariatric surgery,” Obesity Surgery, 22 (2) 213-219.
Publisher – Google Scholar.
6. Qian, W., Cheng, Y., & Tian-long, W. (2012). “Ultrasound facilitates identification of combined spinal-epidural puncture in obese parturients,” Chinese Medical Journal, 125 (21) 3840-3843.
Google Scholar.
7. Rasoulian, A., Lohser, J., Najafi, M., et al. (2011). “Utility of prepuncture ultrasound for localization of the thoracic epidural space,” Canadian Journal of Anesthesia, 58 (9) 815-823.
Publisher – Google Scholar.
8. Sahota, J.S., Carvalho, J.C.A., Balki, M., et al. (2013). “Ultrasound estimates for midline epidural punctures in the obese parturient: Paramedian sagittal oblique is comparable to transverse median plane,” Anesthesia & Analgesia, 116 (4) 829-835.
Publisher – Google Scholar.
9. Tran, D., Kamani, A.A., Lessoway, V.A., et al. (2009). “Preinsertion paramedian ultrasound guidance for epidural anesthesia,” Anesthesia & Analgesia, 109 (2) 661-667.
Publisher – Google Scholar.
10. von Ungern-Sternberg, B.S., Regli, A., Reber, A., et al. (2005). “Effect of obesity and thoracic epidural analgesia on perioperative spirometry,” British Journal of Anaesthesia, 94 (1) 121-127.
Publisher – Google Scholar.