Verstraete Maud1, Debucquoy Annelies1, Sagaert Xavier2, Van Cutsem Eric3 and Haustermans Karin1
1Department of Radiation Oncology, University Hospital Gasthuisberg, Belgium
2Centre for translational cell and tissue research, Catholic University of Leuven, Leuven, Belgium
3Digestive Oncology Unit, University Hospitals Gasthuisberg, Leuven, Belgium
Volume 2012 (2012),
Article ID 796042,
Advances in Cancer Research & Treatment,
31 pages,
DOI: 10.5171/2012.796042
Received date: 17 September 2012; Accepted date: 7 October 2012; Published date: 30 December 2012
Academic Editor: Angelita Habr-Gama
Cite this Article as:
Verstraete Maud, Debucquoy Annelies, Sagaert Xavier, Van Cutsem Eric and Haustermans Karin (2012), " Anti-Angiogenic Therapy Combined with Chemoradiotherapy for Patients with Localized Advanced Rectal Cancer," Advances in Cancer: Research & Treatment, Vol. 2012 (2012), Article ID 796042, DOI: 10.5171/2012.796042
In the last decade, major advances have been achieved in the treatment of rectal cancer. Results of randomized controlled trials have led to the introduction of total mesorectal excision and preoperative (chemo) radiotherapy as a standard multimodal treatment approach. By combining these different treatment modalities, patients are less likely to suffer local recurrence and are more likely to maintain sphincter function and retain a reasonably good quality of life. To further improve the treatment response, many efforts have been made to integrate targeted biological agents into the conventional therapy. Anti-angiogenic treatment has been shown in preclinical and clinical studies to possibly potentiate chemoradiosensitivity. The researchers present an overview of the mechanisms of action and a summary of published results of chemoradiotherapy with anti-angiogenic drugs in the treatment of locally advanced rectal carcinoma. At present, many obstacles still have to be conquered to use this combination in daily clinical routine. Problems of resistance, invasion and metastasis as well as timing and dosing of the combination therapy when using anti-angiogenic compounds are discussed in this review. Also, attention for better response prediction and better understanding of the complexity of anti-angiogenic therapy in combination with chemoradiation is needed to lead to future improvements in the use of these agents in the clinic.
Keywords: Rectal cancer — anti-angiogenic therapy — radiotherapy.
Introduction
Rectal cancer accounts for about 30% of all colorectal tumors, which are the second leading cause of cancer-related death in the Western world (Jemal et al., 2011). One of the important pillars in the treatment of locally advanced rectal cancer is surgery. In recent years, important advances have been made in the surgical techniques used for the resection of these tumors, the most important of which being the concept of total mesorectal excision (TME) which reduces local recurrences and perioperative morbidity (Cecil et al., 2004;Kapiteijn et al., 2001).
To further improve the outcome of the patients, the addition of radiotherapy to surgery has been extensively evaluated. The short-term treatment that delivers 25 Gy in 5 fractions during 1 week, followed immediately by surgery, is used today. Preoperative radiotherapy decreases local recurrence rates by 50 to 60% as compared with surgery alone (Anon 1990a;Anon 1990b;Anon 1997;Dahl et al., 1990;Gerard et al., 1988;Goldberg et al., 1994;Marsh et al., 1994;Reis Neto et al., 1989). The data was confirmed by long-term results of patients treated with preoperative short-term radiotherapy with a mean follow up of 12 years showing a reduction in 10-year local recurrence by more than 50% relative to surgery alone, however without an overall survival benefit (Van et al., 2011).
More recently, the addition of chemotherapy to radiotherapy has been assessed in several studies (Bosset et al., 2006;Cecil, Sexton, Moran & Heald, 2004;Crane et al., 2003;Grann et al., 2001;Minsky et al., 1992), leading to an integration of chemotherapy in the treatment schedule. Comparing preoperative chemoradiotherapy with postoperative chemoradiotherapy showed a similar overall survival in both patient groups, although the preoperative treatment was less toxic and was associated with less local recurrences (Bosset et al., 2006;Sauer et al., 2004). Based on the results of all the trials mentioned above, the current standard treatment of locally advanced rectal cancer consists of preoperative chemoradiation followed by TME surgery (Rodel, 2010).
Next to this evolution to a multimodal treatment, better tumor staging and treatment tailoring led to the major progress that has been made in the treatment of rectal cancer. Patients are less likely to suffer local recurrence and are more likely to maintain sphincter function and retain a reasonably good quality of life. However, the response to this treatment is very heterogeneous and depends on the tumor characteristics. Based on tumor size, the involvement of lymph nodes, the mesorectal fascia involvement and vascular invasion, rectal tumors can be divided to ‘good’ (no bad prognostic factors on MRI scan), ‘bad’ (those having features on MRI suggesting increased risk for distant metastases) and ‘ugly’ (those with features suggesting high risk for local recurrences and distant metastases) (Smith and Brown, 2008). Since the introduction of TME surgery (Gerard et al., 2006;Ogino et al., 2005;Sauer et al., 2004), the number of local relapses in the ‘good’ and ‘bad’ group are quite low (±8%). However, still about 20% of the patients with an ‘ugly’ tumor develop local recurrences (Smith & Brown, 2008). For this sub-group of patients, mostly consisting of extensive T3 and T4 tumors reaching to and beyond the mesorectal fascia, an intensification of the preoperative treatment is urgently needed.
This could be achieved by combining targeted agents with the conventional treatment. Angiogenesis, the physiological process involving the growth of new blood vessels from pre-existing vessels, is an obvious target, since neo-vascularisation is essential for tumor growth, progression and metastasis (Folkman, 1971;Folkman, 2002). In this review, the researchers discuss the way to integrate anti-angiogenic agents in the preoperative treatment of rectal cancer by looking back on the knowledge that has been gathered in the last decade and by looking forward to ways of overcoming current bottlenecks.
Angiogenesis: Key Players and Role in Cancer
The process of angiogenesis is a delicate balance that is operated by several receptors (VEGR, FGFR, PDGFR,…) and their corresponding ligands in concert with other contributing factors, such as matrix metalloproteinases (MMPs), chemokines , etc. In normal tissues, the collaborative action of proangiogenic factors (VEGF, FGF, angiopoetin-2) is in balance with the action of endogenous anti-angiogenic and vascular stabilizing factors (thrombospondin, angiopoeietin-1, …). In tumors, the presence of hypoxia drives the production of angiogenic factors leading to the formation of new vasculature that is functionally abnormal at macroscopic and microscopic levels. Anatomically, tumoral microvessels are dilated and tortuous with random patterns of interconnection and branching. At the cellular level, the endothelial cells of the tumor vessels have an irregular, disorganized morphology. In addition, perivascular cells, both pericytes and vascular smooth muscle cells, demonstrate abnormal structural characteristics (Goel et al., 2011).
The vascular endothelial growth factor (VEGF) family and its receptors are the best characterized signaling pathway in tumor angiogenesis. The VEGF family embraces different members including VEGF-A, VEGF-B, VEGF-C, VEGF-D and placental growth factor (PlGF). The first member is the best characterized and most often referred to as VEGF, as the researchers do also in this review. VEGF was first cloned and identified as a secreted angiogenic mitogen in 1989 (Leung et al., 1989). In 1992, Shweiki et al., demonstrate that VEGF is induced by hypoxia and may mediate hypoxia-initiated angiogenesis (Shweiki et al., 1992). Four years later, VEGF was shown to be indispensable for developmental angiogenesis (Carmeliet et al., 1996; Ferrara et al., 1996). VEGF binds to two transmembrane tyrosine kinase receptors, VEGFR1 (also known as FLT1) and VEGFR2 (also known as KDR) expressed on vascular endothelial cells. The binding of VEGF to these receptors initiates a cascade of signaling pathways that mediate endothelial cell migration, proliferation, survival and permeability. VEGFR2 is the principal receptor that promotes the pro-angiogenic functioning of VEGF. The role of VEGFR1, with PlGF as a main ligand, is not so straight-forward. VEGFR1 may function as a decoy receptor to prevent VEGF to bind to VEGFR2, but may also have a role in hematopoiesis and recruitment of monocytes and other bone-marrow derived cells helping to promote angiogenesis. Next to its role as a mitogen and survival factor for endothelial cells in a paracrine manner, VEGF can also function in an autocrine way. Tumor cells have shown to express VEGF and functional VEGF receptors, thereby creating an autocrine loop, mediating a direct survival effect on tumour cells (Bachelder et al., 2001;Calvani et al., 2008;Dias et al., 2000). Also in colorectal cancer, autocrine VEGF has shown to have an essential growth and survival function on colorectal tumour cells (Samuel et al., 2011). VEGF is a major angiogenic factor in all solid tumors. Also in colorectal cancer, VEGF plays a prominent role in tumor-related angiogenesis and is associated with worse survival and higher rates for distant metastasis (Cascinu et al., 2002;Chin et al., 2000;Lee et al., 2000;Nanashima et al., 1998), making it a promising target for therapeutic intervention in cancer treatment, alone and in combination with chemo- or radiotherapy.
The fibroblast growth factors (FGF) acting through their cognate receptors (FGFRs) are also important in tumor angiogenesis. The FGF family consists of at least 22 members with FGF-1 (acidic FGF) and FGF-2 (basic FGF) being the prototype members. They bind and activate their FGFRs in the presence of heparin proteoglycans. This starts a signal transduction cascade leading to diverse biological responses, including cell differentiation, proliferation and matrix dissolution, initiating a process of mitogenic activity critical for the growth of endothelial cells, fibroblasts and smooth muscle cells, all necessary for the development of functional vasculature. FGF-2 is expressed by numerous tumor types and exerts its proangiogenic activity by interacting with tyrosine kinase receptors, heparan-sulfate proteoglycans, and integrins expressed on the endothelial cell surface. FGF receptor 2 (FGFR2) was also found to be overexpressed in the invasive front of colorectal cancer (Matsuda et al., 2011).
Angiopoietins, platelet-derived growth factor (PDGF) and the Dll4/Notch signalling are known to have a role in development and differentiation of the vessel wall. PDGF-B/PDGFR-β is important for the recruitment of pericytes and maturation of the vasculature (Lindahl et al., 1997). Also angiopoietins are required for the formation of mature blood vessels (Thurston, 2003). Delta-like 4 ligand (DLL4) is a third major regulator of vascular maturation during development and tumor angiogenesis and is in direct cross-talk with VEGF (Patel et al., 2006;Phng and Gerhardt, 2009). VEGF upregulates DDL4 in tip cells and on his turn interacts with its receptor Notch in stalk cells. As a negative feedback loop, DLL4/Notch downregulates VEGFR2 expression in Notch expressing endothelial cells, reducing VEGF-induced angiogenesis. DLL4/Notch signaling in endothelial cells seems to be context dependent. In situations of hypoxic stress, hypoxic signals (such as VEGF) cooperate with Notch to escape from this stress, with the latter having a role in the endothelial tip-stalk cell specification (Fraisl et al., 2009b). Under hypoxic stress, VEGF activates endothelial cells to express the ligand DLL4. When VEGF is released, both the induction of angiogenesis and the production of DLL4 are required to coordinate the response into the formation of functional vasculature. It has been shown that under reduced Notch signaling, no functional vessel patterning and perfusion can occur and hypoxia persists, even when VEGF is present and induces vessel formation (Li et al., 2007;Thurston et al., 2007). Surprisingly, recently it was shown that DLL4 protein expression in tip cells is only weakly modulated by VEGR2-expression. Notch inhibition had no significant impact on VEGFR2-expression; however VEGFR3 was strongly modulated by Notch, allowing angiogenesis without VEGFR2-signaling (Benedito et al., 2012). Another main contributor to angiogenesis are the matrix metalloproteinases (MMPs). They help to degrade the vessel wall allowing endothelial cells to escape into the interstitual matrix to further stimulate angiogenesis.
Cancer associated fibroblasts contribute to angiogenesis by release of stromal cell derived factor-1 (SDF-1) (or named chemokine (C-X-C motif) ligand 12 (CXCL12)). SDF-1 leads to the recruitment of endothelial progenitor cells (EPCs) from the bone marrow through a CXCR4 (chemokine (C-X-C motif) receptor 4) dependent mechanism (Zheng et al., 2007). Activation of the chemokine CXCL12 (SDF-1α)-CXCR4 pathway is implicated in the homing of cancer cells to target metastatic organs. This leads to promotion of cancer cell survival and invasion, recruitment of “distal stroma” (i.e., myeloid bone marrow-derived cells) to indirectly facilitate tumor recurrence and metastasis, and promotion of angiogenesis directly or in a paracrine manner (Duda et al., 2011;Xu et al., 2009).
Rationale for Combining Anti-Angiogenic Drugs with Chemoradiotherapy
Many mechanisms for the anti-tumor activity of angiogenesis-targeted therapy have been proposed (Ellis and Hicklin, 2008). The mechanism by which anti-angiogenic therapy enhances the activity of chemotherapy and radiation is not fully understood, but many hypotheses are put forward (O’Reilly, 2006;Wachsberger et al., 2003;Willett et al., 2006) (Figure 1).
Figure1. VEGF Signaling Pathways Involved in Tumor Angiogenesis
First, it could be attributed to a process of ‘normalization’ of tumor vasculature (Jain, 2001;Jain, 2005). The majority of radiation-induced damage results from generation of highly reactive oxygen species. Consequently, reduced oxygen is known to limit the DNA damage effect caused by radiation, resulting in hypoxic cells being three times more radio-resistant compared to normoxic cells. Hypoxia, a hallmark of solid tumors, drives the production of angiogenic factors, including VEGF, within the tumor (Shweiki et al., 1992). The production of VEGF results in an ‘angiogenic’ switch, thereby allowing the tumor to grow exponentially (Bergers and Benjamin, 2003). Having this said, combining anti-angiogenic agents with chemoradiation seems rather counterintuitive. However, Jain came up with the ‘normalization’ hypothesis as a mechanism of action of anti-angiogenic agents (Jain, 2005). In contrast to normal vasculature, the excessive local production of angiogenic factors results in physically abnormal and inefficient blood vessels with defective endothelium, basement membrane and pericyte coverage (Carmeliet and Jain, 2000). These aberrant blood vessels do not sufficiently provide the cells with oxygen, leading to regions of hypoxia, which are irresponsive to treatment. As a response to the hypoxic tumor cells, angiogenesis is further stimulated initiating a positive feedback loop. In this context, the ‘normalization’ hypothesis can explain how anti-angiogenic agents can break this loop and improve the efficacy of chemo –and radiotherapy (Jain, 2005). When administering anti-angiogenic agents, the balance between pro-and anti-angiogenic factors is restored, thereby transiently remodeling or ‘normalizing’ the abnormal tumor vasculature. The normalization of the blood vessels is further achieved by inhibition of MMPs involved in degrading extracellular matrix (Egeblad and Werb, 2002). VEGFR2 blocking seems to alter the basement membrane homeostasis, either by degrading an abnormal pathological thick basement membrane or synthesizing a basement membrane reducing tumorgenicity and metastasis (Winkler et al., 2004). VEGFR2 inhibition also results in an increase in pericyt coverage of tumor vessels by upregulation of Angiopoietin-1 implying vessel maturation and improved vascular function (Winkler et al., 2004). Due to this normalization, perfusion increases, improving the delivery of radiosensitizing oxygen and chemotherapeutics. By decreasing the abnormal vascular permeability, interstitual fluid pressure (IFP) decreases, also improving delivery of cytotoxic therapies.
Due to the changes that occur after anti-angiogenic treatment– including decrease in interstitial fluid pressure (IFP)– improved vessel function and a decrease in tumor hypoxia, the effect of both chemotherapy and radiotherapy could be increased. In the case of chemotherapy, the clinical evidence supporting normalization as a mechanism for improved drug delivery is indirect, coming from the trials showing benefit from combination therapy of colorectal, lung and breast cancer. Randomized phase III clinical evidence for synergistic benefit combining anti-angiogenics and radiation treatment is lacking to date. Murine studies support the concept, showing not only synergism but also schedule dependence (Goel et al., 2011). Similar results were reported from some small phase I and II studies (cfr. infra). First evidence was given by Dickson et al., showing in a xenograft model, that normalization indeed improves intratumoral delivery and anti-tumoral activity of chemotherapeutics when given together with bevacizumab (Dickson et al., 2007). Evidence was also given by Dings et al., who showed that anti-angiogenic drugs indeed transiently increase overall tumor oxygenation via vessel normalization, which leads to an increased effect of radiotherapy (Dings et al., 2007).
Next to the normalization of the blood vessels, angiogenic targeted therapy may also sensitize tumors by increasing the radiosensitivity of tumor-associated endothelial cells and tumor cells (Garcia-Barros et al., 2003;Willett et al., 2006). In normal conditions, VEGF functions as a survival factor for both endothelial cells and tumoral cells by protecting them from apoptosis (Harmey and Bouchier-Hayes, 2002). Consequently, tumor cell resistance may increase to conventional chemotherapy and radiotherapy, which showed to increase VEGF in tumor cells (Gorski et al., 1999). However, blocking intracellular VEGF may be an important strategy to render tumor cells more susceptible to treatment. By blocking VEGF, tumors can turn more sensitive to chemotherapy and radiotherapy, which kills tumor cells by inducing apoptotic cell death. In addition, anti-angiogenic agents may inhibit the regrowth of tumors after radiation by decreasing the number of circulating endothelial cells (CECs) and endothelial progenitor cells (EPCs) that are induced by chemoradiation (Bertolini et al., 2006;Willett et al., 2004). Preventing recruitment of these endothelial progenitor cells may increase the indirect killing of cancer cells (Ellis & Hicklin, 2008).
A third additional pathway involved in anti-angiogenesis and interactions with chemoradiotherapy is the phenomenon of the so-called angiogenic regeneration. Giatromanolaki et al. show that the vascular grade is an independent prognostic factor for local relapse and survival in patients with locally advanced squamous cell head and neck cancer (SCHNC) treated with chemotherapeutics. Patients with an intermediate vascular grade show a better response. This could be a consequence of the interplay between drug-and oxygen-availability and cancer cell repopulation (Giatromanolaki et al., 1999). Immunohistochemical staining on biopsies of SCHNC before and after irradiation, revealed that tumors with no complete response after radiotherapy had a higher macrovascular density and an increased percentage of cancer cells with nuclear expression of thymidine phosphorylase (angiogenic factor) than tumors before radiotherapy (Koukourakis et al., 2001). This research led to the idea that intensified angiogenic growth during radiotherapy could be associated with failure of radiotherapy. Consequently, blocking this angiogenic regeneration with anti-angiogenic drugs in combination with the irradiation might give a better therapy response.
Another possible mechanism of anti-VEGF therapy, aside from its vascular effect, may be a direct effect on cancer cells themselves leading to down-regulation of genes involved in radiation damage repair. mRNA expression analysis on biopsies from patients with colorectal cancer treated with bevacizumab and radiotherapy showed an effect on specific cancer pathways and not on hypoxia target genes or endothelial markers (Koukourakis et al., 2009). Especially enzymes involved in DNA repair were found to be downregulated by bevacizumab, which might be of importance in the sensitization of cancer cells to irradiation.
Anti-Angiogenic Agents
Knowledge of the crucial role for cancer growth and metastasis and insights into the molecular mechanisms in the process of angiogenesis, have led to the development and clinical use of anti-angiogenic agents in cancer therapy (Carmeliet, 2005). Several classes of anti-angiogenic agents have been developed, including neutralizing monoclonal antibodies, small-molecule tyrosine kinase inhibitors (TKI) of growth factor receptors and soluble receptor constructs. For different key players in the angiogenic process, the production of inhibitors is ongoing either to administer on their own or in combination with VEGF inhibitors in order to overcome resistance.
Numerous angiogenic agents targeting VEGF ligands, VEGF receptors or VEGF receptor tyrosine kinases have been developed and are under investigation. Bevacizumab (Avastin®), a humanized monoclonal antibody to VEGF, is the most clinically advanced anti-angiogenic drug used in rectal cancer and is currently the only anti-angiogenesis antibody that has been approved by the FDA and the European Medicines Agency for the treatment of metastatic colorectal cancer. Bevacizumab inhibits VEGF, preventing binding to its receptors, thereby inhibiting the VEGF/VEGFR signaling pathway (Ferrara et al., 2004). In the absence of VEGF, endothelial cells are unable to survive, grow and proliferate, causing regression of existing vessels and inhibition of new vessel formation (Ellis & Hicklin, 2008;Ferrara et al., 2003). VEGFR may also be expressed on cancer cells. Therefore, anti-VEGF agents can directly interfere with their survival or enhance their sensitivity to other therapies (Jain, 2005). However at this time, the use of bevacizumab as a standard radiosensitizer had not been proven yet to have additional benefit for response in treatment for patients with locally advanced rectal cancer. Other antibodies blocking VEGF receptors are in various stages of clinical development. Ramucirumab (IMC-1121b) is a human mAB against VEGFR-2. Clinical activity was seen in a phase I setting, and is being tested in a phase II trial for advanced colorectal cancer (Spratlin et al., 2010). Another mAb under investigation is Icrucumab (IMC-18F1), which targets VEGFR-1 (Schwartz et al., 2010). A VEGF-trap to one of the VEGF ligands is also a way of preventing the ligands to bind their receptors. Aflibercept (AVE0005) is a VEGF receptor decoy fusion protein, binding to the VEGF-A and PlGF ligands (Holash et al., 2002). To the researchers’ knowledge, there are no clinical data in rectal cancer available for these antibodies and the VEGF trap.
In contrast with the VEGF-trap or VEGFR-targeting antibodies, to which drug resistance can develop due to targeting of a single angiogenic pathway, small molecules have the advantage of being more promiscuous in target inhibition. Therefore, also many tyrosine kinase inhibitors (TKI) targeting VEGFR kinases, as well as downstream intracellular signaling processes such as the RAS/RAF/MEK/ERK pathway leading to cellular proliferation were developed (Ivy et al., 2009). Between the many TKI developed examples tested in colorectal cancer are Sorafenib (BAY 43-9006), Sunitinib (SU11248), Cediranib (AZD2171), Axitinib (AG-013736), Regorafenib (BAY73-4506) and Brivanib (BMS-582664) (Hubbard and Grothey, 2010). However, until now, the role of TKIs in the management of colorectal cancer has not yet been established. To the researchers’ knowledge, in rectal cancer there is no clinical data available with these drugs.
Probably, the future use of VEGF inhibiting agents in clinical practice lies in combining them with other therapies, such as chemotherapy, radiotherapy or other targeted therapies. Many preclinical studies could show a cooperative anti-tumoral effect of TKI and fusion molecules with irradiation and support the concept of combining anti-angiogenic agents with radiotherapy. For instance, evidence for a synergistic effect of anti-angiogenic drugs and radiotherapy was given in vitro and in xenograft mice models for Vatalinib (PTK787) (Hess et al., 2001;Riesterer et al., 2011), SU6668 and SU5416 (Ansiaux et al., 2006;Griffin et al., 2002;Lu et al., 2004;Schuuring et al., 2005;Timke et al., 2008), Cediranib (Cao et al., 2006;Williams et al., 2007), Sorafenib (Heravi et al., 2012;Kuo et al., 2012;Plastaras et al., 2007;Suen et al., 2010), Sunitinib (Schueneman et al., 2003;Zhang et al., 2011) and Aflibercept (Wachsberger et al., 2007). Also, characteristics of normalization of the tumor vasculature after administration of TKIs in xenograft models were found (Kamoun et al., 2009;Ohta et al., 2009;Taguchi et al., 2008).
However, clinical trial evidence for synergistic benefit combining anti-angiogenic agents and irradiation is lacking to date, since so far no phase III trial could confirm a net benefit. More research and clinical trials combining antiangiogenic agents with irradiation are therefore warranted.
Experimental evidence suggests that targeting of FGF-2 and other FGFs or FGFRs might overcome the resistance to anti-VEGF(R) therapy (Knights and Cook, 2010). Murakami et al. found that basal FGF stimulation of endothelium is required for maintenance of VEGFR-2 expression and the ability to respond to VEGF stimulation. Consequently, a combination of FGF and VEGF signaling inhibition may have more profound effect on the vasculature, as the rebound in vascular growth is not likely to occur in the absence of VEGR2 expression (Murakami et al., 2011). In mice models, resistance after anti-angiogenic treatment with VEGF antibodies was shown to diminish when also the FGF signaling was inhibited (Casanovas et al., 2005). Therefore, highly potent FGFR TKIs, which are selective over VEGFRs might offer more opportunities for combined treatment with irradiation.
Other potential targets that might enhance the effects of VEGF(R) inhibition include PlGF, angiopoietins, mTOR, integrins and CXCR4. Combination treatment with VEGFR inhibitors and inhibitors of one of the above mentioned targets all showed in vivo an enhanced effect of VEGF targeted therapy (Fischer et al., 2007;Fokas et al., 2012;Goel et al., 2011;Jiang and Liu, 2008;Koh et al., 2010;Xu et al., 2009).
Targeting DDL4/Notch signaling also has been proven to have an important impact on tumor angiogenesis and growth (Fischer et al., 2011;Funahashi et al., 2008;Ridgway et al., 2006;Wu et al., 2010). Blocking DLL4 creates more vessels but non-functional ones (Noguera-Troise et al., 2006). So since DLL4 acts on tumor vasculature in a different way from that of VEGF, targeting both DLL4 and VEGF may be complementary and has the potential to overcome resistance to anti-VEGF therapy. Tumors that continue growing in presence of anti-VEFG treatment undergo a marked reduction in growth when DDL4 is blocked (Noguera-Troise et al., 2006;Ridgway et al., 2006) . Recently, Li et al. show that combined blocking of DLL4-Notch signaling may enhance the efficacy of VEGF inhibitors, particularly in DLL4-upregulated tumors, and thus provide a rational base for the development of novel strategies to overcome antiangiogenic resistance in the clinic (Li et al., 2011). It was also shown in colorectal xenograft models, that blocking Notch following irradiation caused tumor growth delay by promoting non-functional angiogenesis and extensive tumor necrosis (Liu et al., 2011). Combining Notch blockers following irradiation could therefore be a promising approach to reduce recurrence in patients.
A more modern approach to normalization could be promoting endothelial cell quiescence for example by PHD2 knockdown. Cellular oxygen sensing is performed by HIF-prolyl hydroxylases (PHD), which controls HIF-1α to respond to hypoxia. Activation of HIF-1α in tumor cells upregulates VEGF production, promoting vessel abnormalisation. Haplodeficiency of PHD2 induces vasculature normalization, improving tumor oxygenation and perfusion, without affecting primary tumor growth and developing metastasis (Mazzone et al., 2009). Due to complexity of the HIF signaling system with multiple hydroxylases, no inhibitor specific for distinct PHD isoforms is currently available (Miyata et al., 2011). Since there is a growing interest in this oxygen sensor as drug target, search for inhibitors is ongoing (Fraisl et al., 2009a), with some promising results (Dao et al., 2009;Kwon et al., 2011;Nangaku et al., 2007;Teli and Rajanikant, 2012). Further research efforts on generating specific PHD inhibitors is desirable.
Clinical Trials
The array of preclinical evidence supporting the normalization hypothesis, coupled with clinical trial data, e.g., in metastatic colorectal cancer (Cao et al., 2009;Kozloff et al., 2009;Loupakis et al., 2010;Saltz et al., 2008;Tebbutt et al., 2010;Welch et al., 2010), have prompted a number of clinical studies to determine if vascular normalization occurs in rectal cancer patients and whether the combination of anti-angiogenic treatment with chemoradiation might be beneficial. Until now, bevacizumab is the only anti-angiogenic agent that has been tested in combination with chemoradiation in rectal cancer in the clinic. The studies, explained below, are listed in table I.
Table 1. Clinical Trials with Bevacizumab for Patients with Locally Advanced Rectal Cancer
Willett et al. reported a first phase I trial in 2004 with bevacizumab as a single agent given 14 days prior to 5FU-based chemoradiotherapy (CRT) in 6 patients with locally advanced stage II/III rectal cancer. The mechanism of action of bevacizumab in combination with CRT was investigated by means of imaging with dynamic perfusion CT and 18F-FDG-PET, tumor interstitial pressure measurements, tumor vascular density measurements and measuring circulating biomarkers. The data proved direct anti-vascular effect of bevacizumab on rectal cancer, showing decreased tumor perfusion, microvascular density, IFP and less CECs and EPCs following a single dose of bevacizumab. Also, increased pericyt coverage of tumor vasculature supported the normalization hypothesis (Willett et al., 2004). A continued phase I study showed safety of bevacizumab at a dose of 5mg/kg in combination with 5FU and irradiation (Willett et al., 2005). Again, evidence of vascular normalization and antivascular mechanisms was given. Because of these dose-limiting toxicities, only 5 patients were enrolled at the 10 mg/kg dose. Two consecutive patients, receiving 10mg/kg bevacizumab, developed dose-limiting toxicities of diarrhea and colitis during the combined treatment but resumed and completed radiation therapy and fluorouracil after recovery. Other noted side effects were pulmonary embolus day 1 postoperatively (n=1), ileostomy obstruction with stent-related ileal perforation 10 days following resection (n=1), and transiently increased systolic blood pressure by 20 mmHg 12 days after the first injection of BV (n=1). In 2009, Willett et al. updated their results in a phase II study in a cohort of 32 patients with LARC. Neoadjuvant bevacizumab with 5FU and radiation therapy showed to be safe and active. An improved survival was demonstrated with 100% local control and overall survival after 5 years (Willett et al., 2009). A year later, they published the long term outcome of bevacizumab with chemoradiation compared with standard chemoradiation of this phase II study. A favorable trend for patients treated with bevacizumab was observed, with acceptable acute and post-operative toxicity and promising long-term efficacy (Willett et al., 2010). Safety and encouraging response rates of irradiation with fluoropyrimidine and bevacizumab in patients with LARC were also demonstrated in a phase I study (Czito et al., 2007) and a phase II study (Kennecke et al., 2012) with neoadjuvant bevacizumab, IR, capecitabine and oxaliplatin. In the study of Czito et al., bevacizumab at a loading dose of 15 mg/kg with additional infusions of 10 mg/m2 caused dose-limiting toxicity (primarily diarrhea) when attempting “full-dose” capecitabine and oxaliplatin with this regimen (capecitabine 825 mg/m2/bid during the course of radiation, and oxaliplatin 50 mg/m2 weekly). However, the same regimen of bevacizumab was well-tolerated at the lowest dose level (capecitabine 625 mg/m2/bid during radiation days, and oxaliplatin 50 mg/m2 weekly), and was declared the recommended phase II dose in the study. In the study of Kennecke et al., the most common grade 3/4 pre-operative toxicities were diarrhoea (24%), pelvic pain (10%) and fatigue (10%). The most common grade 3/4 post-operative toxicities were pain, fatigue and infection (all 13%). Crane et al. showed in a phase II study that adding bevacizumab to neoadjuvant IR and capecitabine, gives encouraging pathological complete response (pCR) rates (32%) without increase in acute toxicity. However, the impact of bevacizumab on perineal wound and anastamotic healing due to concurrent bevacizumab requires further attention. A perioperative complication rate of 32% was observed. In particular, 4 of 6 patients who underwent abdominoperineal resection had either a minor or major complication (two delayed perineal wound healing, two anastomotic leaks and a superficial wound infection) (Crane et al., 2010). Recently, 3 other phase II studies tested the feasibility and tolerability of this regimen (neoadjuvant bevacizumab, capecitabine and RT) for LARC. The adverse event profile observed by Velenik et al. was comparable to the study of Crane et al., but the pCR rate was lower. In total, 62.3% of the patients developed perioperative complications. The most frequent were delayed wound healing (30.0%), infection/abscess (20.0%) and anastomotic leakage (11.7%) (Velenik et al., 2011). The trial of Resh et al. terminated early because 50% of the patients experienced grade 3 toxicity (Resch et al., 2012). Major side effects were intestinal bleeding (grade 3, 25%), diarrhea (grade 3, 25%), perianal and abdominal pain (grades 3 and 4, 25%) and anemia (grade 3, 12.5%). The schedule of neoadjuvant therapy was shown to be safe and active in the study of Gasparini et al., but no improvement of ypCR and long term control over standard neoadjuvant fluoropyrimidine based RT was found (Gasparini et al., 2012). The most frequent side effects were grade 1-2 diarrhea, proctitis, rectal bleeding and hypertension. Other encouraging results were observed from a phase I/II trial combining hypofractionated split-course accelerated radiotherapy with capecitabine and bevacizumab, supported with amifostine for patients with locally advanced inoperable/recurrent colorectal tumors. The regimen was proven feasible and resulted in a high rate of durable complete responders (68.5%) (Koukourakis et al., 2009). There was low acute toxicity, with moist perineal desquamation (2/22 patients, diarrhea grade 2 to 3 (5/22 patients), and severe proctalgia (2/22 patients). One patient died from Fournier’s gangrene before treatment completion. In a later phase I/II study, the same hypofractionated radiochemotherapy scheme based on capecitabine was combined with bevacizumab for patients with preoperative radiotherapy in rectal cancer (Koukourakis et al., 2011b). The regimen showed acceptable tolerance, however acute toxicity in the group receiving bevacizumab was higher compared to the group without. The acute toxicities were grade 2/3 diarrhea (36.8%), abdominal pain and grade 2/3 proctalgia (21.1%), however regressed completely within 2 weeks. Perioperative complications including delayed wound healing or wound infection were not noted, with the exception of one fatal case of pulmonary embolism. The pathological complete response rate in patients treated with bevacizumab was 36.8% compared with 21.4% to the group not treated with bevacizumab.
The group of Dipetrillo evaluated recently in a phase II study the feasibility and pathologic complete response rate of induction bevacizumab with 5FU, leucovorin and oxaliplatin (FOLFOX) 6 regimen followed by concurrent neoadjuvant bevacizumab, oxaliplatin, 5FU and radiation for patients with rectal cancer (Dipetrillo et al., 2012). The pathologic complete response rate (20%) of this regimen was similar to other 5FU chemoradiation regimens, but the trial was terminated early because of toxicity after 26 treated patients. During chemoradiation, grade 3/4 toxicity was experienced by 76% of the patients, with diarrhea (44%), neutropenia (20%) and pain (16%) being the most common side effects. In addition, the high incidence of postoperative wound complications (36%) (including infection (16%), delayed healing (12%), leak/abscess (8%), sterile fluid collection (8%), ischemic colonic reservoir (4%) and fistula (4%)) is concerning and needs further attention.
In conclusion, most regimens showed to be safe and active when 5mg/kg bevacizumab was adminstered prior to and concurrent with chemoradiotherapy. Although the treatment schemes of all these studies are comparable, the percentage of patients with a pCR varied between 14% and 40%, stressing the importance of a good selection of patients for this combination treatment. The toxicity of this combination treatment was acceptable in all but two studies (Dipetrillo et al., 2012;Resch et al., 2012). The preoperative toxicity in the study of Dipetrillo et al. could be explained by the long induction treatment with bevacizumab and chemotherapy before the start of chemoradiation. The toxicity of the Resch trial is less obvious since the only aberrant factor in the study if Resch et al. is the radiation treatment scheme of 45Gy in 25 fractions compared with the scheme of 50.4Gy in 28 fractions in the other studies. In several trials, bevacizumab seemed to have an important impact on postoperative complications and consequently merits particular notice in future trials. Differences in occurrence of wound complications could be observed between the studies. A possible risk factor for wound-healing complications may be the interval between the last dose of bevacizumab and surgery. Moreover, differences in patient selection, variations in the half-life of bevacizumab between patients, differences in surgical technique and practice, and chance alone (since some studies have a small patient numbers), could be possible explanations for the variation between the studies (Crane et al., 2010).
So to date, although response rates and safety results of anti-angiogenic therapies as radiosensitizers seem promising, a lack of phase III data in rectal cancer patients makes it currently not recommendable to use it outside clinical trials. Also, the heterogenous response of the patients calls for the identification of biomarkers.
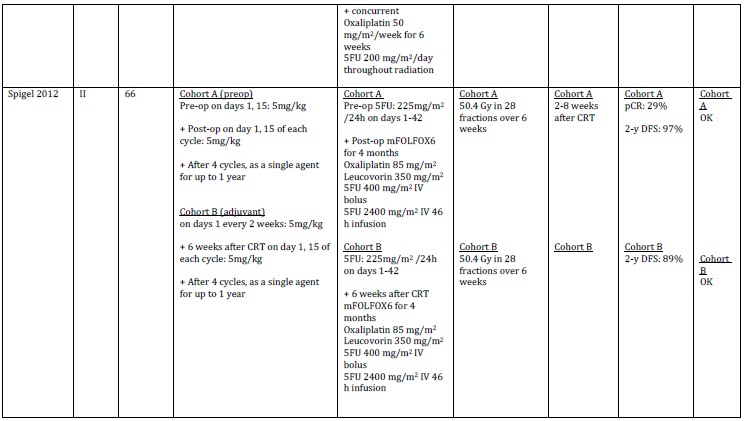
In contrast to the above mentioned trials, recently a phase II trial administred bevacizumab in an adjuvant setting. Spigel et al. investigated the use of bevacizumab with chemoradiation (5-FU) in preoperative (cohort A) and adjuvant settings (cohort B) for patients with stage II/III rectal cancer. After surgery (in the preoperative setting) or chemoradiation (in the adjuvant setting), 5-FU, leucovorin, oxaliplatin (mFOLFOX6) and bevacizumab were administered for 4 months and then bevacizumab was given alone for up to 1 year. They demonstrated that bevacizumab could be safely incorporated into modern chemoradiation schedules in either the preoperative or adjuvant setting. Toxicities were expected and were manageable. Frequent grade 3/4 toxicity included diarrhea (A cohort, 14%; B cohort, 29%), neutropenia (A cohort, 14%, B cohort, 23%), mucositis (A cohort, 23%, B cohort, 0%) and fatigue (A cohort, 6%, B cohort, 10%). The most serious toxicities were wound dehiscence (1 patient cohort B), pelvic infection (1 patient cohort A), bowel perforation (1 patient cohort A) and fistula formation (1 patient cohort B). In the preoperative setting, the pCR rate was 29%. One- and 2-year DFS (disease-free survival) for the preoperative/adjuvant treatment were 85%/not reached and 97%/89%, respectively (Spigel et al., 2012). However, before using bevacizumab in the adjuvant setting, a better understanding of the working mechanisms of bevacizumab and more clinical trials with bevacizumab in this setting are needed.
Obstacles to Conquer for Using Anti-Angiogenic Agents
In order to attain better responses with this combined treatment, different obstacles will have to be conquered. One important hurdle to overcome is the development of resistance or tumor escape to anti-angiogenic agents. Two modes of resistance exist: evasive resistance, an adaptation to circumvent the specific angiogenic blockade and intrinsic resistance both caused by several mechanisms extensively explained in different reviews (Bergers and Hanahan, 2008;Crawford and Ferrara, 2009;Ebos et al., 2009b;Shojaei and Ferrara, 2008).
An important explanation is the upregulation of compensatory pro-angiogenic signalling or pre-existing multiplicity or redundant pro-angiogenic signals which can compensate for loss of VEGF signaling. A number of studies have highlighted that chronic inhibition of VEGF stimulates alternative angiogenic signals (Broxterman et al., 2003). One proposed mechanism of tumor escape from anti-VEGF therapy is the up-regulation of FGFs, such as FGF-2. Through selection of resistant clones, tumor cells can become less sensitive to hypoxia or nutrient deprivation. Another mechanism may involve the tumor-microenvironment. Stromal cells, including fibroblasts, inflammatory cells and pericytes, are thought to contribute to tumor resistance to anti-VEGF (Shojaei & Ferrara, 2008). Agents targeting alternative angiogenic pathways, including FGFR, PlGF, angiopoeitins, DLL4/Notch, CXCRs and many others could possibly resolve some of the resistance development (Teicher, 2011).
In addition, VEGF independent mechanisms may cause sustained tumor angiogenesis. These include the activation of the chemokine CXCL12 (SDF1α)-CXCR4 pathway or the DLL4-Notch signaling. Xu et al. showed that bevacizumab can upregulate a number of pro-inflammatory pathways in patients with rectal cancer and that increased serum levels of SDF1α and upregulated tumor levels of CXCR4 are significantly associated with an increase in the incidence of distant metastases 3 years after resection (Xu et al., 2009). Concerning the DLL4 pathway, mice with overexpression of DLL4 showed resistance to bevacizumab in vivo. The large vessels induced by DLL4-Notch signaling increased tumor blood supply and were no longer dependent on VEGF signaling. They also observed activation of other pathways of tumor resistance driven by DLL4-Notch signaling, including the FGF2-FGFR pathway (Li et al., 2011).
Several groups also suggested increased aggressiveness, invasiveness and metastasis by anti-angiogenic therapy. VEGF inhibition is thought to promote a switch of cancer cells to a more metastatic and invasive phenotype which increases distant metastasis and limits patient survival (Ebos and Kerbel, 2011). In various metastatic assays, metastatic tumor growth was accelerated and overall survival was decreased in mice receiving an inhibitor of tumor angiogenesis (Ebos et al., 2009a;Paez-Ribes et al., 2009). Withdrawal of VEGF treatment was also shown to lead to rapid re-growth of tumor vessels and tumor growth (Mancuso et al., 2006). Chronic exposure of colorectal cancer cells to bevacizumab was demonstrated to promote compensatory pathways that mediate tumor cell migration (Fan et al., 2011).
Going hand in hand with the above mentioned problems, careful attention is warranted for timing and dosing of combination therapies. The timing of onset and offset of the vessel normalization has not been defined in humans and thus maximum benefit by synchronizing CRT with vascular normalization may not have been fully achieved yet. Optimal scheduling, by finding a good balance between therapeutic inefficacy and excessive vascular regression preventing adequate oxygen and drug delivery, will create a window of opportunity wherein oxygen and chemotherapy will have maximum access to cancer cells, improving therapy (Jain, 2005). Maybe scheduling anti-VEGF treatment prior to the CRT gives the advantage of allowing normalization to set in.
The use of VEGF-targeted therapy can bring along some complications since VEGF signaling has a pivotal role also in physiological processes (Carmeliet et al., 1996;Ferrara et al., 1996). VEGF does not only mediate endothelial-cell function, but also plays a role in the function of pericytes, immune-effector cells (Heine et al., 2011), haemopoietic precursor cells (Podar and Anderson, 2005) and the central nervous system (Lambrechts and Carmeliet, 2006). VEGF has a critical role in wound healing, liver regeneration and endothelial integrity. Therefore, complications due to a reduction in VEGF availability are not surprising. The most frequently described side effects are arterial hypertension, gastrointestinal perforations, wound healing complications, serious bleeding, arterial and venous thromboembolic events, renal toxicity and influences on liver parenchyma (Hompes and Ruers, 2011). The effect of anti-angiogenic agents on perioperative wound complications needs important attention when patients undergo surgery. Since bevacizumab has a half-life of 20 days [range 11–50 days], an appropriate interval of time is needed between surgical procedures and treatment for surgery to be safe (Bose et al., 2010).
Since the response of individual tumors to therapy is not uniform and it is not clear yet who benefits from this class of drugs, better response prediction allowing a selection of patients benefiting from anti-angiogenic treatment is needed (La Thangue and Kerr, 2011).
In rectal cancer, some biomarkers have been put forward. One main category of markers was directly involved in the VEGF pathway. Plasma soluble VEGFR-1 was suggested to be a potential dual biomarker of response and toxicity for neoadjuvant treatment with bevacizumab containing chemoradiation (Duda et al., 2010). Moreover, pre-treatment CD-34 vessel density, post-treatment Ki-67 labeling index and VEGFR-2 cancer cells expression significantly correlated with residual tumor area in a phase II study of neoadjuvant bevacizumab plus capecitabine and concomitant RT in patients with locally advanced rectal cancer (Gasparini et al., 2012).
Since not all tumors are angiogenic and different aniogiogenic pathways may be active in different tumors, the sensitivity to anti-angiogenic drugs may also depend on these differences. Giatromanolaki examined recently the predictive and prognostic role of the vascular density in colorectal carcinomas (Giatromanolaki et al., 2012). The standard and active vascular density on material from the CONFIRM trials, investigating vatalanib, was assessed by immunohistochemistry for CD31 pan-endothelial cell marker and phosphorylated/active form of the VEGFR2 receptor. Tumors with high pVEGFR2 positive vascular density showed a poorer response to FOLFOX chemotherapy compared with those with high vascular density. On the other hand, patients with an activated VEGFR angiogenic pathway show a substantial benefit when receiving vatalanib in combination with chemotherapy, suggesting that vatalanib only has an anti-angiogenic effect when the VEGFR pathway is active on the tumor vasculature. Therefore, assessment of VEGFR activated vasculature may be a potent marker for efficacy of angiogenic inhibitors. The same group also analyzed the role of LDH (lactate dehydrogenase) serum levels and LDH5 tissue expression levels (also regulated by HIFs) in colorectal carcinomas from the CONFIRM trials (Koukourakis et al., 2011a). LDH levels were associated with resistance to standard chemotherapy and worse PFS. However, addition of vatalanib improved response and PFS in patients with high LDH5 expression, showing a potential value for LDH levels in predicting benefit from chemotherapy and anti-angiogenic compounds. Intratumoral mRNA expression of genes regulated by HIF1α was also analysed on tumor specimen from the CONFIRM-1 trial. Elevated mRNA expression of LDHA, GLUT-1 and VEGFR1 were associated with response to chemotherapy with vatalanib, elevated LDHA and VEGFR1 mRNA levels were associated with improved PFS in patients treated with chemotherapy and vatalanib, and increased HIF1α and VEGFR2 mRNA levels were associated with decreased survival in patients receiving chemotherapy but not in patients who additionally received vatalanib (Wilson et al., 2012). The data suggesting that intratumoral mRNA expression of genes involved in angiogenesis/HIF pathway may predict outcome to VEGFR-inhibitors.
Some data proposes a role for circulating endothelial cells (CECs) and circulating progenitor cells (CPCs) as prognostic marker reflecting active angiogenesis. Also in rectal cancer patients, it was shown that bevacizumab can decrease the number of viable CECs and CPCs (Duda et al., 2006;Willett et al., 2004;Willett et al., 2005).
Finding germline or somatic tumoral mutations may also help to identify a subpopulation of rectal cancer patients being sensitive or resistant to the effects of bevacizumab. Ghadimi et al. were the first to show that prediction of response to neoadjuvant CRT by gene expression profile is possible (Ghadimi et al., 2005) . Two other groups followed to show that micro-array analysis is successful to predict complete response of rectal tumors to preoperative CRT (Kim et al., 2007;Rimkus et al., 2008). However, recently those 3 previously identified classifiers could not be validated, which led to the conclusion that the utility of microarrays in predictive medicine is not yet in reach for rectal cancer and that alternatives to microarray should be considered (Brettingham-Moore et al., 2011). As an alternative, array comparative genomic hybridization (aCGH) to detect genomic imbalances like genomic copy number changes could provide useful predictive information on response to neoadjuvant CRT in rectal cancer (Molinari et al., 2011).
The heterogeneous response to VEGF inhibitors may also be related to inherited variations in genes coding for products involved in angiogenesis. Research of single-nucleotide polymorphism (SNPs) in genes of VEGF and their association with clinical outcome could be promising. Kim et al. demonstrated a possible prognostic value of VEGF genetic variations in CRC focusing on SNPs (Kim et al., 2008). Associations were shown between two SNPs in the VEGFR-2 gene and CD105-positive microvessels in patients with CRC, indicating an impact on neoangiogenesis. Moreover, an association between the SNPs and survival was demonstrated, providing evidence for a possible functional importance of SNPs in the VEGFR-2 gene (Hansen et al., 2010). Formica et al. were the first studying the predictive value of SNPs in the VEGF system in relation to chemotherapy with bevacizumab in colorectal cancer. They evaluated 40 mCRC patients treated with first-line fluorouracil and leucovorin in combination with irinotecan plus bevacizumab. They concluded that investigation of germline vascular VEGF gene polymorphisms may help to identify patients who are more sensitive to anti-VEGF agents (Formica et al., 2011). The Nordic ACT trial investigated the predictive value of SNPs. They found that the VEGFR-1 319 C/A SNP is a potential predictive marker for first-line treatment with bevacizumab plus chemotherapy in patients with mCRC (Hansen et al., 2011). Hansen et al. demonstrated that the VEGFR-1 319 C/A SNP was related to response in 218 patients with mCRC treated with first-line combination chemotherapy plus bevacizumab. Patients with the A allele appeared to have increased response rates (T.Hansen, 2011). In the treatment of rectal cancer patients with anti-angiogenic agents, no predictive value for SNP’s has been identified and validated so far. However, most recently Lambrechts et al. presented a novel and promising marker predictive of bevacizumab treatment outcome by a systematic screening of common genetic variability in key VEGF signalling pathway genes (Lambrechts et al., 2012). They identified a genetic locus in the VEGFR-1 tyrosine-kinase domain that is associated with PFS and OS in pancreatic cancer patients (AViTA trial) and with PFS in renal-cell carcinoma patients (AVOREN trial) receiving bevacizumab. This association was found to be specific for patients receiving bevacizumab since no significant effects were seen in placebo-treated patients. The effect of this marker was also functionally validated at the biological level. A synonymous SNP affecting tyrosine 1213 in the VEGFR-1 tyrosine-kinase domain was identified as the functional variant underlying the association. This SNP causes a shift in codon usage, leading to increased VEGFR-1 expression and downstream VEGFR-1 signalling. Prospective studies are waiting to validate the predictive diagnostic value of this novel biomarker in various cancer types receiving antiangiogenic therapies.
Although a lot of attempts have been done, at present there are no optimized, standardized or validated biomarkers of response, toxicity or resistance for anti-angiogenic therapy available (Jain et al., 2009;Murukesh et al., 2010;Pohl et al., 2011). Therefore, strong biomarker research needs to be conducted to allow us to use anti-angiogenic agents in the best way.
Conclusion
A strong rationale to combine anti-VEGF therapy with chemoradiation in patients with rectal cancer came from positive results in preclinical models and mCRC patients. Although targeting VEGF in combination with chemoradiotherapy represents an effective treatment for patients with rectal cancer in certain settings, significant benefits could not be realized yet for all patients in terms of DFS and OS. Further understanding of the mechanisms of action and resistance will be necessary to develop further advantages in adding anti-angiogenic treatment to the conventional treatment. Finding biomarkers and genetic variations for better response prediction, optimizing dose and schedule of bevacizumab regimens, and finding ways to overcome resistance, will be the key focus in the future to pursuit a more personalized and adapted therapy for patients with rectal cancer.
In response to irradiation, VEGF is upregulated in tumors through activation of the PI3K/AKT/mTOR pathway, promoting the HIF1α-VEGF pathway (Gorski et al., 1999). When VEGF binds its receptor VEGFR-2, several pathways are activated. In the ECs, the primary target of VEGF, the activated signaling pathways result in growth and proliferation of vascular ECs, EC survival, vascular permeability, vasodilatation and EC migration, all helping with the orchestration of angiogenesis. VEGF also acts in an autocrine manner mediating a direct survival effect on the tumor cells by protecting them from apoptosis. Secretion and activation of MMPs, involved in degradation of ECM, is also mediated by VEGF. Pericytes, important for vessel maturation, are regulated by angiopoeitin-1, under influence of VEGF. VEGF also contributes to recruitment of EPC and stromal cells. However, angiogenesis stimulated by all these different mechanisms, leads to a structural and functional abnormal tumor vasculature, impairing the efficacy of radiochemotherapy. Inhibition of VEGF by bevacizumab can block these effects leading to vessel normalization and diminished tumor growth which leads to less hypoxia and better response to radiochemotherapy. Blocking VEGF may also render tumor cells more susceptible to chemoradiotherapy which kills the cell by apoptosis.
Karin Haustermans and Annelies Debucquoy are supported by a fundamental clinical mandate and a post-doctoral research mandate of the FWO respectively. Maud Verstraete is supported by the IWT. This work is supported by Varian Biosynergy.
Holash, J., Davis, S., Papadopoulos, N., Croll, S. D., Ho, L., Russell, M., Boland, P., Leidich, R., Hylton, D., Burova, E., Ioffe, E., Huang, T., Radziejewski, C., Bailey, K., Fandl, J. P., Daly, T., Wiegand, S. J., Yancopoulos, G. D. & Rudge, J. S. (2002). “VEGF-Trap: A VEGF Blocker with Potent Antitumor Effects,” Proc.Natl.Acad.Sci.U.S.A, 99, (17) 11393-11398. Publisher – Google Scholar – British Library Direct
National Institutes of Health (1990a). ‘NIH Consensus Conference. Adjuvant Therapy for Patients with Colon and Rectal Cancer,’ JAMA, 264, (11) 1444-1450. Google Scholar
Stockholm Rectal Cancer Study Group (1990b). ‘Preoperative Short-Term Radiation Therapy in Operable Rectal Carcinoma. A Prospective Randomized Trial,’ Cancer, 66, (1) 49-55. Google Scholar
Wu, Y., Cain-Hom, C., Choy, L., Hagenbeek, T. J., de Leon, G. P., Chen, Y., Finkle, D., Venook, R., Wu, X., Ridgway, J., Schahin-Reed, D., Dow, G. J., Shelton, A., Stawicki, S., Watts, R. J., Zhang, J., Choy, R., Howard, P., Kadyk, L., Yan, M., Zha, J., Callahan, C. A., Hymowitz, S. G. & Siebel, C. W. (2010). “Therapeutic Antibody Targeting of Individual Notch Receptors,” Nature, 464, (7291) 1052-1057. Publisher – Google Scholar