Ines Velez1, Maritzabel Hogge2, Steven Kaltman3, Eustorgio Lopez4 and Kurt Friedman5
1,5Oral and Maxillofacial Pathology Nova Southeastern University, USA
2Oral and Maxillofacial Radiology Nova Southeastern University, USA
3,4Oral and Maxillofacial Surgery Nova Southeastern University, USA
Volume 2013 (2013),
Article ID 530750,
Journal of Research and Practice in Dentistry,
8 pages,
DOI: 10.5171/2013.530750
Received date: 5 September 2013; Accepted date: 28 October 2013; Published date: 9 December 2013
Academic Editor: Midion Mapfumo Chidzonga
Cite this Article as:
Ines Velez, Maritzabel Hogge, Steven Kaltman, Eustorgio Lopez and Kurt Friedman (2013), "Central Mucoepidermoid Carcinoma: A Rare Entity Analysis of Five Cases," International Journal of Research and Practice in Dentistry, Vol. 2013 (2013), Article ID 530750, DOI: 10.5171/2013.530750
Mucoepidermoid carcinoma (MC) is one of the most common salivary gland neoplasms. When it develops inside the bone, is called Central Mucoepidermoid Carcinoma.(CMC) MC is the most common malignant salivary gland tumor in children, and the most common central salivary gland neoplasm. Misdiagnosis of CMC occurs frequently, due to the rareness of the location for a salivary gland tumor and the clinical and radiographic manifestations, which are suggestive of an odontogenic lesion. It is often treated inappropriately or late, leaving undesired sequelae. We report four cases of CMC and analyze five, with different manifestations and diagnostic problems. The dental profession should be aware of the fact that this malignant tumor may mimic benign processes.
According to Pires et al., (2003), the diagnosis and treatment of salivary gland tumors (SGT) constitute a challenge for the clinician. In the book by Dardick (1996) is mentioned that clinical and radiographic manifestations of these neoplasms are diverse and they are characterized by the most complicated histology of any tissue in the human body.
Ezsias et al., (1994) stated that MC is the most common malignant salivary gland tumor in children and the most common intra-osseous salivary gland carcinoma. Approximately 3% of all mucoepidermoid carcinomas are intra-osseous, and in that case, they are called Central Mucoepidermoid Carcinoma (CMC). Besides the occurrence of mucoepidermoid carcinoma in the oral cavity and bone, it has been reported in other anatomic locations as nasal cavity, (Deepak et al., 1998) thyroid, (Jayaram et al., 1998) and Eustachian tube (Kim et al., 2003).
While the pathogenesis of CMC is not known, some theories of its origin do exist. It has been theorized that embryological pluripotential cells can give rise to dental or salivary gland tissues. The most likely source for an intra-osseous salivary gland neoplasm is odontogenic epithelium. Mucous—producing cells are commonly seen in odontogenic cyst linings. Furthermore, glandular tumors can develop in association with non-erupted teeth. An odontogenic condition called glandular odontogenic cyst, often mimics CMC, clinically, radiographically and histologically. CMC appears most commonly in middle-aged adults but has been reported in all ages. No ethnicity predilection has been identified. The usual location is the posterior area of the mandible, followed by the posterior maxilla. But CMC may appear in any tooth bearing area of the jaws. Frequent symptoms are cortical swelling, pain, often radiating to other body areas, paresthesia, numbness and trismus.
Radiographic imaging is often a multilocular, well circumscribed radiolucency. Displacement of the teeth, cortical perforation and root resorption are not uncommon. A few reported cases of a mixed radiolucent/radiopaque presentation of CMC are in the English literature. The fifth case analyzed in this paper, (Velez et al., 2008) which was characterized by radiolucent/radiopaque manifestation, was previously reported by one of the authors.
Report of Four New Cases:
Case # 1
70 year old male patient, Slight expansion of posterior right mandible is noted upon extra-oral examination. Intra-oral exam exhibits swelling of the mandible and a 2 cm soft mass on the alveolar ridge covered by discolored, smooth mucosa. Patient stated that an extraction was performed “several” years previously due to a “cyst with an unerupted tooth”. The soft tissue nodule had been growing for months. Panoramic radiography exhibits a large radiolucent, well circumscribed, multilocular manifestation with cortical destruction this lesion clearly originated inside bone and the soft tissue lesion is an extension of the intraosseous mass. With a differential diagnosis of ameloblastoma and odontogenic keratocystic tumor, a biopsy was performed. A salivary gland tumor was diagnosed as intermediate grade central mucoepidermoid carcinoma. Hemi-mandibulectomy and reconstruction followed the diagnosis. No recurrence found after four years.
Case # 2
25 year old oriental female consulted for extreme pain on the right maxilla, radiating to teeth, palate, nose and face, present for some months. It was previously diagnosed as a traumatic condition and pain medications were prescribed. Clinical examination disclosed a red/bluish flat area on posterior right maxilla over the palatine foramen (Fig # 1) Imaging shows a well circumscribed lytic lesion with cortical compromise. (Fig # 2-3)The soft tissue discoloration is a manifestation of the intraosseous tumor. Incisional biopsy showed a tumor composed of squamoid cells with mitotic activity and perineural invasion, goblet cells, and micro cysts, it was diagnosed as central mucoepidermoid carcinoma intermediate to high grade.( Fig # Block resection with 2.0 cm margin was performed and an temporary obturator was placed. The patient is free of tumor one year later.
Case # 3
56 year old male with history of long standing pain and numbness in the left mandible and left arm. Clinical examination exhibited expansion of the posterior mandible. Radiography exhibited a large, expansive, well circumscribed radiolucent and radiopaque lesion with cortical compromise and associated with an impacted molar. Biopsy showed central mucoepidermoid carcinoma intermediate grade. Partial hemi-mandibulectomy with 1.5 cm margin, and placement of a reconstructive bone plate was performed. (Fig # 4)No recurrence is found after one year.
Case #4
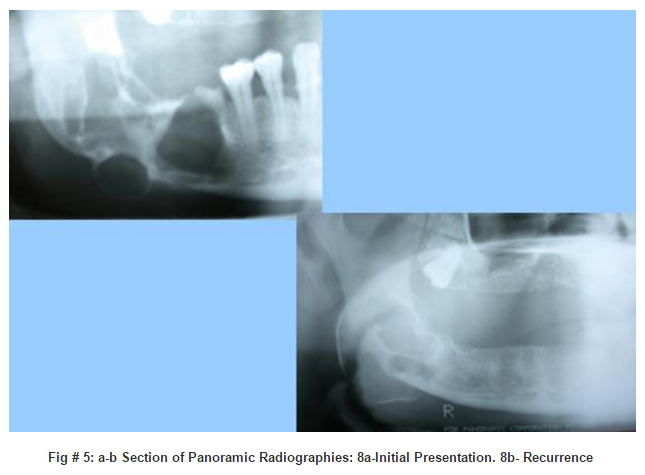
52 year old, white male presented to the clinic complaining about pain of the posterior right mandible. Upon clinical examination, expansion of the inferior border of the mandible was noticed. The patient stated that he had previous surgery of an impacted tooth which was diagnosed as follicular cyst. Panoramic radiography was taken and a radiolucent multilocular, well circumscribed lesion, with cortical compromise and severe expansion, was seen. (Fig #5)New biopsy disclosed low grade CMC. Patient underwent block resection with 1.0cm margins and reconstructive bone plate placement. He is free of recurrence four years later.
Case 5 previously reported by one of the authors:
Case# 5
African American female with the chief complaint of severe pain in the anterior maxilla. A mixed radiolucent/radiopaque lesion, well defined, apical to the vital central incisors, was found. With the differential diagnosis of focal cemento-osseous dysplasia, early central ossifying fibroma, calcifying epithelial odontogenic tumor, and desmoplastic ameloblastoma, an incisional biopsy was performed. The diagnosis of central mucoepidermoid carcinoma, low grade, was rendered. The tumor has not recurred in five years, after block resection with 1.0 cm margin. Discussion
Misdiagnosis of CMC occurs frequently, due to several factors, such as the rareness of the location for a salivary gland tumor, the clinical manifestations and the radiographic appearance, which are suggestive of an odontogenic lesion. Furthermore, the histologic finding of mucous cells in odontogenic cysts and the existence of sialo-odontogenic/glandular odontogenic cyst may misguide the pathologist. It may result in a more invasive treatment and worst sequelae for the patient. (Simon et al., 2003)
According to Zhow et al., (2012) the histologic grading of Mucoepidermoid carcinoma for prognostic purposes is based in the degree of cystic formation, the amount of intermediate and epidermoid cells and the grade of anaplasia. Low grade tumors infrequently develop large numbers of epidermoid cells. Most CMC are low grade tumors. Current surgical treatment of choice is block resection, which means removal of the entire specimen as one piece, including at least 1.0 cm margins. Brookstone et al., (2008) reported 40% recurrences after marginal resection and 4% recurrence after block resection. CMC is not as rare as it was previously thought, and metastases are reported by Lebsack et al., (1990) in about 9 %. The main symptom of CMC found in the cases reported in this paper is pain. All the cases were painful; however, the type of pain was different. In two of the patients, the pain was extreme. Two had radiating symptoms to the face and to the left arm and left mandible. In those cases is easy to misdiagnose the condition. Radiating left arm pain, as well as left mandible, is an important symptom of a heart attack, especially when it is associated, like in case # 3, with numbness or tingling sensations. Radiating pain to teeth, palate, nose and face from the palatine foramen in case # 2 may mislead the clinician to focus on dental, neural or maxillary sinus problems. The case # 5 was characterized by extreme pain, especially upon percussion, suggesting dental origin.
Misdiagnosis is of common occurrence: Three cases were associated to unerupted teeth and one was periapical located. Case # 1 was misdiagnosed clinically and radiographically as dentigerous cyst, and treated as such. Case # 2 was clinically diagnosed for months as “traumatic lesion” therefore the treatment was delayed. The symptoms of case # 3 were suggestive of a heart attack. Case # 4 was misdiagnosed clinically, radiographically and histologically as dentigerous cyst with mucous cells, and therefore a wrong treatment was performed. The pain in case # 5 was suggestive of endodontic problem. Even worst, the radiographic image of this later patient combined with the associated pain was reminiscent of osteoblastoma.
Even further, case # 4 had a negative PET scan. (Table # 1) This is another factor that contributes to the wrong diagnosis and treatment. It is well known that malignant tumors with a large amount of mucin or pus are FDG PET negative because the FDG uptake correlates with the cellularity of the tumor and the amount of mucin. These tumors do not have enough nuclei to uptake the radioactive material.
Central mucoepidermoid carcinoma, due to the extensive variation of the clinical and imagenologic presentation, is often no treated in time or treated inappropriately, leaving undesired sequelae.
Table # 1: Summary of 5 Cases, With Clinical, Imagenologic and Histologic Manifestation
10. Velez I, Johnson B, Central mucoepidermoid carcinoma with an atypical radiographic appearance. Oral Surg, Oral Med, Oral Pathol, Endodontics and Radiol. 2008; Electronic version.doi:10.1016/j.tripleo.