Lisa R. Simmons1, Lynday Molyneaux2, Elizabeth L Chua3, Steve Chadban4 and Dennis K. Yue5
1,2,3,5Diabetes Centre, Royal Prince Alfred Hospital, Level 6, West Wing, Missenden Road, Camperdown, NSW, 2050, Australia
4Department of Transplantation Medicine, Royal Prince Alfred Hospital, Missenden Road, Camperdown, NSW, 2050, Australia
4,5Sydney Medical School, The University of Sydney, D06, Sydney, NSW, 2006, Australia
Volume (2014),
Article ID 886759,
Journal of Research in Diabetes,
13 pages,
DOI: 10.5171/2014.886759
Received date: 31 October 2013; Accepted date: 7 January 2014; Published date: 17 December 2014
Academic Editor: Vantyghemmc
Cite this Article as:
Lisa R. Simmons, Lynda Molyneaux, Elizabeth L Chua, Steve Chadban and Dennis K.Yue (2014), " Investigation of the Glycaemic Profile of Corticosteroid-Induced Diabetes following Renal Transplant using Continuous Glucose Monitoring", Journal of Research in Diabetes, Vol. 2014 (2014),Article ID 886759, DOI: 10.5171/2014.886759
The aim of this study was to use continuous glucose monitoring (CGM) to evaluate the timing and magnitude of glucose excursions in renal transplant recipients receiving oral prednisone, which may assist in determining optimal time for detection of hyperglycaemia and treatment strategies for this group of patients Ten patients underwent CGM at 3-10 weeks post-kidney transplantation. CGM was undertaken for 3 consecutive days and area under the curve (GAUC) was calculated for morning, afternoon and evening and compared to night. Multivariate analysis was used to determine factors associated with hyperglycaemia. Hyperglycaemia was most severe in the afternoon period. The presence of established diabetes was a significant determinant of the magnitude of rise in GAUC in the Morning and Afternoon Periods (p<0.002). Night-time hyperglycaemia was predictive of high GAUC at all other time periods. Kidney transplant recipients taking prednisone, a calcineurin inhibitor and mycophenolate exhibited a maximal increase in blood glucose during the afternoon. BGL measurement in the afternoon is likely to be more sensitive than fasting BGL in detecting hyperglycaemia and guiding the need and timing for antihyperglycaemic therapy. By contrast, measurement of fasting BGL alone, an inadequate measure.
Glucocorticoids are commonly used in combination with other immunosuppressive agents, including calcineurin inhibitors and mycophenolate, for the prevention and treatment of transplant rejection. Their use can be accompanied by hyperglycaemia which may worsen pre-existing diabetes or precipitate new onset diabetes after transplantation (NODAT). Mechanisms of glucocorticoid induced hyperglycaemia are multifactorial and the resultant hyperglycaemia is likely to vary depending on the type and frequency of its administration 1-6.
Studies in renal transplant recipients have shown that between 2 and 50% develop NODAT, increasing morbidity and mortality and reducing graft survival 7-13. This variability in incidence is thought to be due to lack of standardised definitions or diagnostic criteria used in early studies, short observation periods, varying therapeutic regimens and differing prevalence of diabetes in different study populations. The risk also appears to increase with higher daily doses of glucocorticoids. Recent data suggest that NODAT incidence increases over time: 10%-20% at 1 year, 20%-25% at 3 years, and 25%-30% at 10 years post-transplant 14-17. A recent study has also shown that hyperglycaemia occurs commonly immediately post-transplant in non-diabetic kidney recipients and that higher blood glucose values in the early post-transplant period may identify patients at risk of developing NODAT 18.
Few studies of optimal strategies to diagnose and manage hyperglycaemia, during the use of glucocorticoids and other diabetogenic immunosuppressive agents, are found in the literature and little evidence exists to quantify the time of day and length of the resultant hyperglycaemic excursions. Continuous glucose monitoring (CGM) provides a new method of obtaining comprehensive glucose profiles and providing information regarding the direction, magnitude, duration and frequency of fluctuations in blood glucose levels 19-21. It allows the identification of trends, often unnoticed with intermittent blood glucose and HbA1c measurements and provides information regarding nocturnal hypoglycaemia and postprandial hyperglycaemia 22-23.
Accurate detection of blood glucose patterns could assist in determining the type and timing of treatment required and may also be used to identify the best time for finger-prick blood glucose monitoring. This study aimed to explore the occurrence, timing and distribution of glucose excursions by CGM in kidney transplant recipients receiving glucocorticoids, and confirm whether they exhibit consistent diurnal variation by analysing their 24 hour glucose profiles. Research Design and Methods
Participants receiving oral glucocorticoid therapy post-transplantation were recruited from the Royal Prince Alfred Hospital Renal Transplant Unit. Inclusion criteria for this study included individuals who have undergone recent organ transplantation (new transplant recipients) and were about to commence or already receiving steroid therapy. Exclusion criteria included patients aged less than 18 years, individuals with known diabetes prior to transplant and participants who were expected to be on glucocorticoid treatment for less than 3 months. The study protocol was approved by the Institutional Ethics Review Board at Royal Prince Alfred Hospital (Protocol no.: X09-0011 and HREC/09/RPAH/15). Informed consent was obtained according to our institutional ethics review committee policy. Study Design
All subjects had a fasting venous blood glucose measurement prior to commencing the study. They performed self-monitoring of blood glucose (SMBG) by intermittent capillary blood sampling, using a glucometer and underwent continuous glucose monitoring for 72 hours, using a portable Medtronics Guardian® REAL-Time continuous glucose monitoring system (CGMS) (Minimed, Northbridge, California). Medtronics CGM uses a glucose oxidase-based sensor to measure interstitial glucose in subcutaneous tissue.
A wireless sensor was inserted subcutaneously into the participant’s abdomen, measuring interstitial glucose levels every 5 minutes for 72 hours and sending it to a monitor for storage. Patients were given written instructions and trained in its use. All patients also received home blood glucose meter training to perform capillary blood glucose measurements four times daily to calibrate the sensor. After the removal of the sensor, the stored information was downloaded onto a computer for further analysis.
Compared with intensive conventional blood glucose measurements, continuous blood glucose monitoring provides much greater insight into glucose levels and trends, facilitating detailed research studies of 24-hour glucose profiles.
Diagnosis and classification of diabetes was based on the current WHO diagnostic criteria of fasting plasma glucose ≥7.0mmol/L or random plasma glucose >11.0mmol/L. The post-meal value was defined as the value obtained 2 hours after the pre-meal measurement.
Statistical Methods
Data were analysed using NCSS (Number Cruncher Statistical System, Kaysville, Utah) 2007. CGM recordings were grouped into 4 equal time periods (Morning: 6am-12pm, Afternoon: 12pm-6pm, Evening: 6pm-12am, Night: 12am-6am). BGLs were determined every 5 minutes by CGM and, hourly means were used to determine GlucoseAUC (GAUC) of each period and its % increase above the Night values.
Results were expressed as mean+SD or median[IQR] and compared by Kruskal-Wallis test. Multivariate analysis was used to assess which factors determined the magnitude of rise in each of the three day time quarters.
Independent variables included diabetes status, prednisone dosage, types of immunosuppressive therapy (in addition to prednisone), the different time periods, fasting BGL and Night GAUC. Only significant variables were included in the final model. Area under the curve was calculated using the trapezoidal rule. Statistical significance level was accepted at p<0.05. Results
CGM was used successfully and appropriately by all patients 3-10 weeks post-transplantation and sensor insertion was well tolerated. One patient was excluded as she failed to measure BGLs for calibration.
Ten patients (6 males/4 female), aged 52.4 12.1years and with a body mass index(BMI) of 26.1 4.0kg/m2 were treated with daily morning doses of prednisone ranging from 15mg to 25mg (mean:19.75 4.15mg/day). One had longstanding diabetes and a further three had new onset diabetes treated with a sulphonylurea prior to undergoing CGM. Six participants had a family history of diabetes. All patients were also receiving other forms of immunosuppression, following recent renal transplantation (Table 1).
Table 1: Patient Demographic and Clinical Profile
Average glucose recording time was 65 hours 32 minutes. Blood glucose was measured 280+/-20 times per 24 hour period and on average 784+/-49 total glucose measurements were recorded per patient. Analysis showed hyperglycaemia was most severe in the Afternoon period. Night GAUC was associated with the magnitude of rise in GAUC for the three other time periods (p<0.002) (Table 2). The presence of established diabetes was a significant determinant of the magnitude of rise in GAUC in both the Morning and Afternoon Periods (p<0.02).
Table 2: Magnitude of GAUC and its % increase above Night GAUC
(* vs Night , † vs Morning, p<0.002)
Only one of the ten patients experienced an episode of hypoglycaemia (blood glucose level <3.3mmol/L). In this case, hypoglycaemia was observed overnight on only a single occasion with no symptoms and no causative or precipitating factors noted. Discussion
Although research in kidney recipients is lacking, studies in the general population (including the DCCT and UKPDS) have demonstrated the beneficial effect of early intensive glycaemic control in preventing complications in type 1 and type 2 diabetes 24-28. This is of increasing importance in transplant recipients who are now living longer due to improved therapy. A need therefore exists for early diabetes detection strategies and management protocols for patients who undergo organ transplantation.
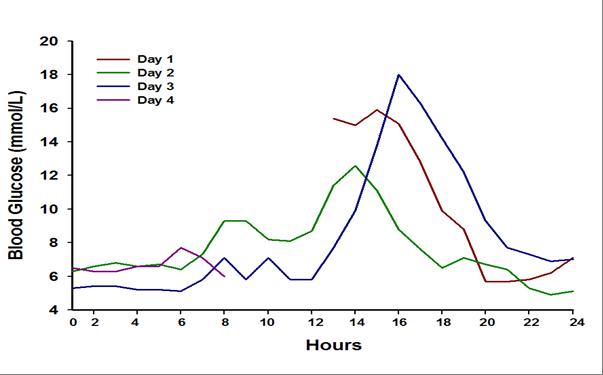
CGM offers the capability of documenting frequency, duration, time and severity of hyperglycaemic episodes more clearly than does intermittent glucose testing. Our study using CGM not only supports the limited data from earlier studies suggesting that patients receiving mane oral prednisone together with other immunosuppressive agents exhibited a maximal increase in blood glucose during the afternoon 29-32 but was also able to quantify glucose excursions more accurately, noting that the afternoon excursion is present for a longer period (Figure 1).
Figure 1: CGM profile of a typical kidney transplant recipient at day 28 post-transplant receiving tacrolimus, mycophenolate and prednisone for immunosuppression
This helps to define the degree of anti-hyperglycaemic therapy that should be directed to this period of time. Despite our modest sample size which is a limitation of this study, and CGM limited to 72 hours, this is the first study of its kind in renal transplant recipients to continuously evaluate the timing and magnitude of glucose excursions during the day and overnight. Future studies incorporating a larger sample size would allow for multivariate analysis to confirm that the negative associations were real. Further studies addressing the impact of various therapies on BGL control and the modulating effects of immunosuppressive agents are warranted.
Although CGM is well tolerated and highly informative, its use to screen for hyperglycaemia for every patient is not practical, as it is expensive and requires additional training. However, a study of this nature helps to provide quantitative data to guide evidence based management.
In conclusion, patients receiving oral prednisone in the morning exhibited a maximal increase in blood glucose during the afternoon. In patients receiving mane prednisone, BGL measurement in the afternoon would be more sensitive in detecting hyperglycaemia and guiding the need for anti-hyperglycaemic therapy, with measurement of fasting BGL alone clearly an inadequate measure.
Treatment should therefore target improving insulin availability, particularly in the afternoon. The persistence of hyperglycaemia throughout the afternoon period suggests that short acting insulin with a 4 to 6 hour action, rather than a rapid acting insulin analogue, may provide better treatment for this type of hyperglycaemia. In subjects with pre-existing diabetes and overnight hyperglycaemia, additional measures to provide more insulin in the morning and evening may also be necessary.
Further studies addressing the impact of various therapies on BGL control and the modulating effects of immunosuppressive agents over a broader range of corticosteroid type and dosage are warranted References
8. Davidson, J, Wilkinson, A, Dantal, J, et al. New-onset diabetes after transplantation: 2003 International consensus guidelines. Proceedings of an international expert panel meeting. Barcelona, Spain, 19 February 2003. Transplantation 2003; 75:SS3-SS24. Google Scholar
9. Caillard S, Eprinchard L, Perrin P, Braun L, Heibel F, Moreau F, Kessler L, Moulin B. Incidence and risk factors of glucose metabolism disorders in kidney transplant recipients: role of systematic screening by oral glucose tolerance test. Transplantation. 2011; 15;91(7):757-64. Google Scholar
11. Cosio, FG, Pesavento, TE, Kim, S, et al. Patient survival after renal transplantation: IV. Impact of post-transplant diabetes. Kidney Int 2002; 62:1440-1446. Google Scholar
23. Boland E, Monsod T, Delucia M, Brandt CA, Fernando S, Tamborlane WV. Limitations of conventional methods of self-monitoring of blood glucose: lessons learned from 3 days of continuous glucose sensing in pediatric patients with type 1 diabetes. Diabetes Care. 2001;24(11):1858-62. Google Scholar
24. The Diabetes Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 329 :977– 986,1993
25. The UK Prospective Diabetes Study (UKPDS) Group: Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 352 :837– 853,1998 Google Scholar
26. The UK Prospective Diabetes Study (UKPDS) Group: Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet352 :854– 865,1998 Google Scholar
28. Nathan DM, Cleary PA, Backlund JY, Genuth SM, Lachin JM, Orchard TJ, Raskin P, Zinman B; Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group: Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med353 :2643– 2653,2005