Carlos R. CUNHA1, Vítor MENDONÇA2, Elisabete Paulo MORAIS3, Joana FERNANDES4 And Isaías LETRA5
1,3UNIAG; Instituto Politécnico de Bragança, Campus de Santa Apolónia, 5300-253 Bragança, Portugal
2,4,5Instituto Politécnico de Bragança, Campus de Santa Apolónia, 5300-253 Bragança, Portugal
Volume 2020,
Article ID 585068,
IBIMA Business Review,
14 pages,
DOI: 10.5171/2020.585068
Received date: 7 October 2019; Accepted date: 23 October 2020; Published date: 28 December 2020
Academic Editor: Isabel Ferreira
Cite this Article as:
Carlos R. CUNHA, Vítor MENDONÇA, Elisabete Paulo MORAIS, Joana FERNANDES And Isaías LETRA (2020)," Using Mobile Devices and Apps to Assist the Elder Population in Rural Areas and Generate Business Opportunities ", IBIMA Business Review, Vol. 2020 (2020), Article ID 585068, DOI: 10.5171/2020.585068
Providing gerontological cares represents an increased challenge when applied to rural scenarios. This paper discusses the role of technology in gerontology and specifically how technology-based solutions can be developed to assist the elderly population in rural areas. We also characterize the Northeast Portuguese region exposing its rural characteristics and presented some demographic numbers. Finally, a conceptual model and a prototype supported by mobile devices are presented to assist and monitor the elderly and enhance business opportunities. The developed prototype allows not only to assist the elderly in a set of typical elderly population routines – such as those related to health – but also to improve the interaction between the elderly and their relatives and / or caregivers.
This work is part of a more extensive effort that has been made in the search for effective solutions to assist the elderly population in rural areas, typically distant from the main health and / or support services; contributing to relieve these deficits.
Keywords: Mobile Devices, Elders, Rural Regions, Business, Prototype.
Introduction
Factually, rural areas are further apart from services that are of great importance for the elder population, such as services dedicated to health and care. However, it is in these areas that a large part of the elder population resides. Alongside this, usually rural areas tend to be less appealing to the young ones, and, as such, the younger relatives tend to live in more populated and economic developed locations. This is another aspect that adds to the isolation of the elder population in rural regions and makes the family support more difficult, having the elders to relay more in other ways of support. Therefore, it is of great importance to develop some mechanisms that allow a higher connection between all the members of such families.
These mechanisms developed with the aid of information and communication technologies are believed to enhance the assistance to the elders and, with that, improve their life quality. With access to such technologies, one can have a better control of their own health issues, surpass some functional limitations, and it would most likely reduce some safety risks (Siegel & Dorner, 2017).
Also, with this continuous and time accurate regulation of the main health aspects it makes possible for the healthcare providers to act in a more effective and precise way.
However, the existence of a technology directed to the elderly population also enhances some practical aspects that Deist and Latouille (2016) enhanced, namely: even if the technology can be developed, are the elders able to understand and use it? If they are capable of using it, what are the restrictions to an effective use?
It is understandable that the elder population has a divergent approach to internet and health information technologies when compared with younger audiences, nevertheless, over the years there are reported growing rates of usage (Fischer et al., 2014). It is also understandable that older people have more difficulty to understand and follow health information technology, but their acceptance to use the healthcare technology along with the recognition of its benefits, specifically the fact that this technology allows them to remain living in their homes, even if they are alone, “will aid care delivery in an environment of a shortage of carers” (Soar & Seo, 2007, p.155).
It is important to enhance the fact that it is the elders’ acceptance of the healthcare technology that can make the assistance more effective and can help all the stakeholders in this topic, such as public and private entities, public and private healthcare workers, and even the technology developers and supporters (Mostaghel, 2016). And the last ones play an important role in the success of implementing the technology, since one of the main concerns and cause of rejection by the elders is the fact that they feel these technologies are not adjusted to their specific needs and restrictions. The major reported requirement is the possibility to communicate in a daily basis with the health care entities (Ferreira et. al., 2013).
This paper is organized in order to first present a bibliographic context of gerontechnology, then the studied region is presented, specifically the Northeast Portuguese rural area, in terms of demographic characterization. Afterwards, a conceptual model that describes the relevant possibilities of using mobile computing, specifically adapted to elderly populations, is presented. To finish, the software prototype developed for Android smartphones to support the elders in their daily lives, is described. This prototype intends to connect the elders with the selected supporting services, when any health concern appears, since it is intended to monitor the health parameters in a continuous way. It can also enhance the connection with the remaining family members, allowing them to rapidly react if needed, for it is possible to add them as assistants to the monitorization.
Gerontechnology
One of the areas that seeks to find answers to the problem of population aging is gerontechnology – it can be classified as an interdisciplinary area of scientific research that uses technology to respond to the opportunities and expectations of older adults. Gerontechnology is the answer to the needs of the elderly with regard to their self-esteem, personal development, isolation (since it is loneliness that leads to loneliness), changes in life plans, constant adaptation to environmental changes, as well as personal resources (Halicka, 2019).
Gerontechnology is a multidisciplinary science that uses technology to innovate in the geriatric area (Sheets et al., 1997; Graafmans & Taipale, 1998). The report of Smith (2014) demonstrates that in older adults the use of technology is on the rise, however, some remain isolated from digital life altogether. Therefore, while the development of technology is moving forward very quickly, a lot of questions are left without response, particularly regarding today’s oldest populations.
The large majority of older people wish to stay in their homes because this gives them a sense of safety and security, they feel independent, near their family and/or friends, it offers them convenient access to known services and allows them to remain in a familiar and comfortable environment. Nevertheless, this phenomenon called “aging in place” often requires adaptations to maintain comfort and safety adapted to changing circumstances of older people. One of the major causes of disability in this category of subjects is dementia (neurocognitive disorders). Its frequency increases with advancing age reaching almost 50 % in people beyond the age of 90 years in developed countries and 30 % in developing countries (Pinte et al., 2015). One solution, for maintaining older people with neurocognitive impairment in their homes, is by using intelligent environments, spaces embedded with information and communication technologies that create an interactive environment (Lazakidou, 2011).
The development of systems to Gerontechnology is a challenging activity requiring areas as different as artificial intelligence, engineering and human computer interaction, to work together in a way to provide solutions able to satisfy growing needs. The stakeholders need to create systems that are intelligent, in a way to detect emotions or falls; usable, so it can be exploited by people with mobility reduced; and simultaneously autonomous and reliable, to be able to mobility and monitor health.
Gerontechnology is related to (Fernández‐Caballero et al., 2017):
Telemedicine and Telehealth services: in line with the expansion of medical knowledge that has occurred in the past decade; it became impossible to have health professionals with constant availability. In order to overcome this constraint, several researchers have worked to develop and implement systems that exploit probabilistic reasoning and techniques in terms of pattern recognition. In this context, medical decision support systems have been developed and implemented, especially those aimed at the elderly population.
Communication devices for the elderly: there has been work to provide tools and systems capable of enabling the elderly population to increase their level of security and independence. In addition to auxiliary tools that allow the elderly, and the people who are their caregivers, to carry out their daily routines, intelligent communication devices have been created capable of assisting in the care provided to the elderly, in a safer, more effective and comfortable way. The existence of mobile access to the Internet is also something worthwhile.
Social networks for the elderly: the existence of strong social ties and adequate social integration are catalysts for maintaining the mental well-being and health of the elderly population; in this way, the chances of a premature cognitive decline, if not an earlier death, will be reduced. In this domain, it has become very important to design and implement social networks adapted to the elderly population, through the design of friendly interfaces tailored to the capacity of this fringe of society.
Lifelong learning for mental health: the ability to learn throughout life can be substantiated by attending academic courses, educational trips, providing community services or volunteering; these experiences will contribute to brain stimulation and will tend to increase the physical activity of the elderly as well as, they will promote an adequate social integration. In this domain, the computational tools of knowledge representation, semantic analysis and interaction, may allow interesting and viable alternatives to support learning, which would be much more complex to apply if specialized human resources were used, which are scarce.
Rehabilitation and mobility technologies: the independence of the elderly and their social participation depends to a great extent on their mobility capacity. When there are motor disabilities that create mobility barriers, the achievement of several objectives is prevented. In this domain, there are several contributions of science to the level of Biomedical Engineering, Ontological Engineering and systems based on sensors and actuators.
Devices and assistive technologies: Technological solutions for assistance are designed to assist additional accessibility for people with physical difficulties or physical-cognitive disabilities. In this context, the elderly should have access to alternative systems of human-machine interfaces, alternative input and output devices (e.g. voice recognition systems, screen reading tools), among other support systems.
Domestic accidents detection: falls of the elderly are one of the most frequent causes of domestic accidents that end in more or less serious injuries. In these events, a quick call for medical assistance and access to health care is critical (for survival). For this to be possible, it will be essential that the elderly can, independently, request assistance. In this area, personal medical alert systems have been developed. These systems are based on technologies that are able to perceive the occurrence of these events and automatically request assistance from pre-configured entities.
Recognition and regulation of emotions: positive emotions are proven to support a healthy life. In this domain, the so-called Affective Computing, based on AI techniques, has been a fruitful theme in the search for solutions that identify emotions, so that we can develop adequate response mechanisms for the elderly.
Environment adaptation and personalization: the development of intelligent spaces where people are surrounded by technology embedded in the physical space and where it is more or less invisible, is a hot field of investigation. This research area aims to provide personalized and contextualized environmental responses, where users’ needs are perceived and anticipated. AI and Data Engineering, have contributed to this domain.
Social / assistance agents and robots: the 21st century is promising in terms of the ability to develop robots capable of helping people in the most diverse activities. In the field of health, there have also been examples of surgical robots capable of assisting in rehabilitation. Knowledge-based systems are major drivers of this development.
There are some projects that address the themes above. For example, the project “Nutrition for Elder Care”, a nutritional semantic recommender system for the elderly “presents” a nutritional recommender system. Nutrition for Elder Care, is intended to help elderly users to design their own healthy diet plans following the guidance of the nutrition specialist. The system was developed with the intensive use of Semantic Web technologies seeking to share and reuse knowledge between different applications and agents and to discover implicit new knowledge. (Espín, Hurtado, & Noguera, 2016).
The project developed by Lago, Jiménez‐Guarín, & Roncancio (2015) introduces a representation for long-term model patterns of behavior that can be customized according to the characteristics of the context and a measure of similarity to compare how daily life with these patterns. This representation formalizes the elements to be monitored by an AAL solution, considers the variability due to the characteristics of the context and is able to detect and explain anomalies in an explained manner. The paper shows how expressive features of the model by mining patterns in three data sets and shows how the anomalies found can be explained in terms of context characteristics that differ from what was expected. In the future, this can be used to send notifications to caregivers, allowing them to make the best care decisions.
Costa, Julián and Novais (2017) presents iGenda and its evolution, the UserAccess, with the main objective of developing an AAL platform. It presents an analysis of the most recent developments and future perspectives for the work. These projects have an importance for the interoperability of the platforms, demonstrating a case study for the development of AAL.
The paper entitled “Ontological Modeling and Rules-Based Reasoning for the Provision of Personalized Patient Education” by Quinn, Bond and Nugent (2017) offers a personalized approach to patient education that is tailored to the patient’s individual characteristics and health goals. Personalized resources will be the comprehensibility and usability of the medical education process. Taking this personalization into account, this paper presents a conceptual architecture for creating a personalized web-based patient.
Concepción et al. (2017), describe an approach to monitoring physical activity carried out by the elderly in order to establish guidelines for their rehabilitation process and guarantee the well-being of older people. The system uses only a smartphone to retrieve all the necessary information, specifically the data from the phone’s accelerometer. The core of the Ameva algorithm is used to develop an innovative selection, classification technique and discretization for recognition of activities.
The region Terras de Trás-os-Montes (TTM) can be presented as the centre of the northeast rural area of Portugal. This region congregates nine municipalities, namely Alfândega da Fé, Bragança, Macedo de Cavaleiros, Miranda do Douro, Mirandela, Mogadouro, Vila Flor, Vimioso and Vinhais, and registered, in 2018, a population of 107,860 individuals (INE). Nationwide, is one of the most economically deprived and depopulated regions, and is facing now a serious situation regarding its own sustainability, since it has presented over the last decades a continuously increasing aging index. Now the elderly population (citizens over 65 years of age) are three times more numerous than the young ones (citizens under 15 years of age). In 2018, a milestone was reached were the elderly represent 30.0% of the population and the young ones only 10.0% (INE). This demographic aging was an expected situation due to the Portuguese continuously improving living conditions as well as medical and labour conditions, alongside with a continuous decrease in the mortality and fertility rate (Freitas, 2011). However, Portugal would only expect to reach a 300-aging index in 2060, presenting now a 159.4 aging index while the TTM region is already there with a 301.6 aging index, with all the contingencies that come along (Diaconu, 2015; INE).
An aspect that arises from this reality is the fact that in rural areas there is an increasing part of the population that is elderly and lives alone or with other elders and has reduced social connections. Moreover, the lack of descendants or the fact that the descendants are geographically distant reduce the possibility to have support. Subsequently, the traditional support made by family, friends and neighbours is very fragile (Neville et al., 2018). Also, these particular townships tend to be distant from the centres were all the main services are provided which increases the difficult for these individuals that already tend to have reduced mobility since, to attend any public service – hospital, pharmacy, tax administration, or others –, they have to take a transportation. However, and as we are focusing in deprived regions with underprivileged citizens, it is known that poverty can restrict the individual’s possibilities to take a transportation in order to attend some social event or just to attend medical appointments and so this will intensify the probability of increased isolation (Kemperman, et. al., 2019). In this context, the increasing isolation of this part of the population emphasises several problems such as loneliness (emotional or social), depression, social exclusion, a general fragile health, all of which can imply more appointments to public medical facilities or even prolonged stays in hospitals (Cunha, Pereira, & Loureiro, 2019).
This can be regarded in two perspectives, one is that these elders could remain an active part of local society and, in this context, that does not happen and they are isolated and diminished, and, on the other hand, the consequences of that isolation can increase the public health expense, and both perspectives could be prevented. Local and central governments are becoming more aware of the critical situation however there is a lack of means to support all the elderly and isolated population. In fact, the dimension of the social problem of the demographic aging is only due to a reduced, insufficient or inexistent response of the official social services. Also, when the response does exist, such as nursing homes, this implies a considerable cost for the state and it can increase the loneliness of the elderly, since they are removed from their homes, daily routines and social interactions (Freitas, 2011; Hartmann & Gomes, 2014). Therefore, it is necessary to develop means to grant or increase social support to these elders, especially granting them the possibility to remain in their homes in their routines in their neighbourhood, a situation that they prefer and that promotes a better life quality (Fonseca, 2016; Neville et al., 2018).
The social support can be achieved through the support network these elder already have, can develop or can establish. Social support can be understood as the availability of people that elders trust or that care and appreciate them. Social support networks can be formal, when regarding formal public or private organizations that provide formal care, such as health care or daily care organizations; or informal (or natural), when regarding significant persons, such as family, friends or neighbours (Cunha, Pereira, & Loureiro, 2019; Freitas, 2011).
The formal and informal support network together represent the social support network an elder has (Freitas, 2011). The informal support network is developed by the individuals throughout their lives, although in older ages tends to be reduced due to natural changes that occur in their life cycle stage, such as retirement or loss of family and friends. When the informal support network is inexistent or has very few connections then the importance and dependency on formal support increases. However, even when the connections exist in a satisfactory dimension, they can be incapable of providing the care these older adults need and formal support is required (Kemperman et al., 2019).
Nevertheless, the majority of the elders, even when they depend greatly on formal support networks, prefer to remain in their own homes, this allows the elder to maintain some control on their lives and respond better to essential protocols (Fonseca, 2016; Kemperman et al., 2019). The maintenance of the elder in their own homes and the preservation of previous informal relationships is extremely relevant for their quality of life, comfort and even safety in rural communities (Cunha, Pereira, & Loureiro, 2019).
In order for this to happen there must be developed a support that can connect the formal and informal support networks and optimize the effectiveness of both.
Business Opportunities in the Elders’ Assisting Ecosystem
The ecosystem in which care for the elderly falls is quite complex. There are countless and diverse support services that an elderly person needs in their daily lives – cleaning, food, health, leisure services, among others. In this context, and especially when the caregivers are family members, the help of external entities is often requested in order to guarantee the provision of care.
This reality makes possible a set of business opportunities. The integration of support frameworks for the elderly with networks of external service providers is a good opportunity to promote business. In a complementary perspective, from the analysis of the needs for the provision of services, opportunities for creating business tailored to the needs of the elderly may arise, which, in countries with more developed economies, and with a high quality of life, will allow the creation of new topologies of business that satisfies the specific needs of a given group of elderly people who demand more than the undifferentiated offer that currently exists.
As the concepts of need and the mechanism for satisfying that need are complex, the individuality of each elderly person may dictate a set of particularities that prove to be demanding in view of the capacities and availability of classic caregivers (e.g. family, and social security institutions). In this context, the emergence of business solutions should be explored. The development of technology-based solutions, based on applications and mobile devices, may allow a new dynamic for the elderly care ecosystem. Classic business concepts, such as time-to-market, personalized marketing, cooperation networks or 24/7 assistance may be a reality in solutions to support the elderly and / or the families who care for them and who often despair for solutions to help the mission to take care of loved ones.
Following is a proposal for a Framework that aims to respond to the stated premises and culminated with the development of a prototype App that aims at experimenting and validating some of the main concepts of the proposed Framework. However, it is a mission in progress and in a process of continuous improvement.
Framework
The recent technology evolution allows nowadays the measurement of various vital health parameters. Also, the recent developments of Apps has brought intuitive and easy interfaces-manipulation that can be widespread used. Next, we will present a proposal for the development of an application that allows caregivers to better monitor the health status of the elderly. Allowing caregivers to monitor medication intake, measurement values of indicators such as blood glucose, blood pressure, and others.
Fig. 1: Conceptual Proposal
The proposed model, presented in Figure 1, is based on the development of two mobile applications, for tablets and smartphones. This will enable older people to record medication, record indicators, make requests, send messages and, if necessary, send an SOS request. On the other hand, caregivers will be able to monitor the elderly by consulting the records made and / or responding to requests. The functionalities of each of the applications are presented in the use case diagrams shown in Figure 2 (Elderly App) and Figure 3 (Caregiver App).
The model allows that several service providers (e.g. pharmacies, physiotherapists, restaurants, grocery stores, cleaning services, among others) can participate, allowing, on the one hand, to add value to the care provided to the elderly, and on the other, to generate business opportunities.
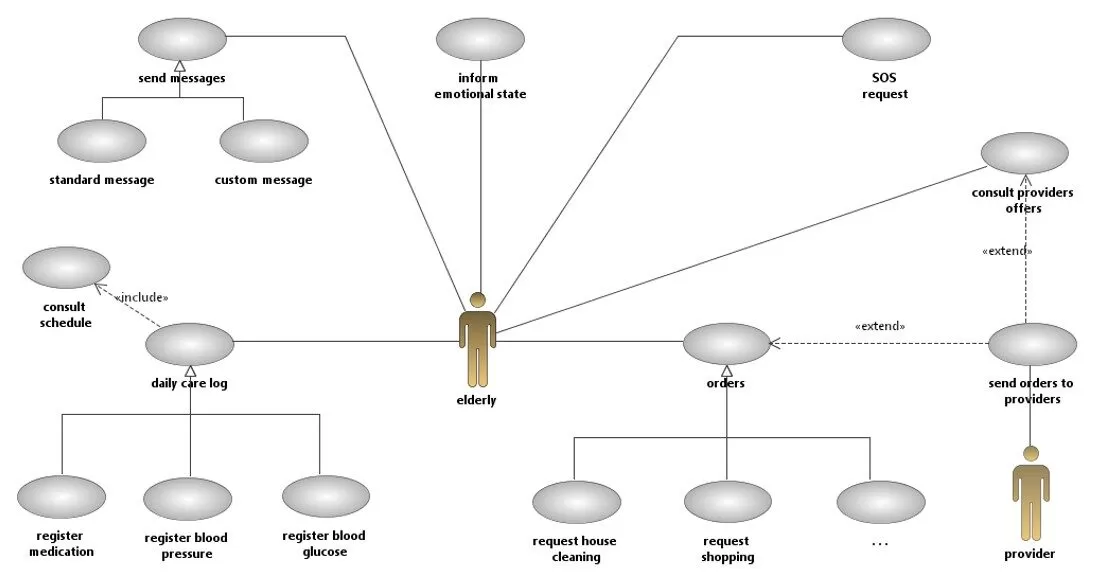
Fig. 2: Elderly Application: Use Cases diagram
Considering Figure 2, it can be seen that the elderly will have at their disposal a set of features that will allow them to communicate with their caregivers, sending messages, indicating their emotional state or even making SOS requests. However, we highlight the daily care record, such as: taking medications, recording blood pressure, recording blood glucose, among others.
Lastly, the elderly people may also make requests to their caregivers, or even send orders to providers, for example requesting the purchase of products or cleaning house services.
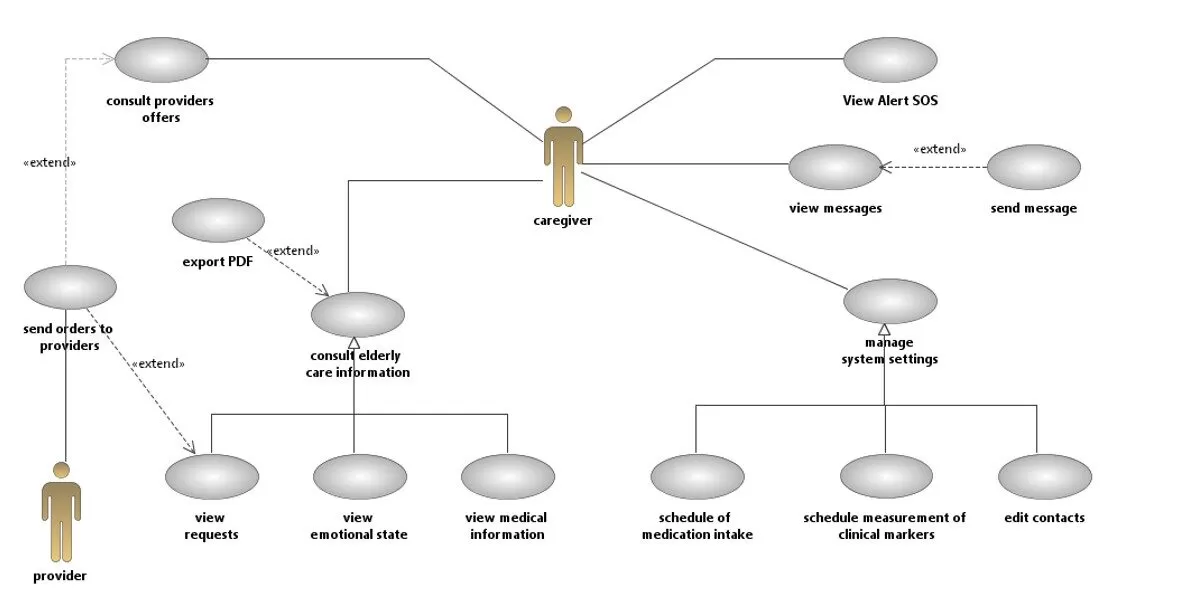
Fig. 3: Caregiver Application: Use Cases diagram
The application that will be used by caregivers of the elderly, includes system configuration features, allowing them to configure the medication’s schedule, customize the indicators to be measured, edit contacts to send messages, among others. In addition to allowing communication with the elderly, the main objective of the application is based on the consultation functionalities of the records made by the elderly, allowing to know if the elderly complied with the medication, track the blood glucose levels and the blood pressure, and consult the elderly requests, and be able to address requests to service providers.
Developed Prototype
The developed prototype is designed to be supported by mobile devices with Android operating system. In this way, technologies were used to create mobile applications in Android environment from a distributed system perspective. Following, is presented the supporting technology architecture as well as some screenshots of some features of the developed Android applications.
Technological Approach and Main Technologies Used
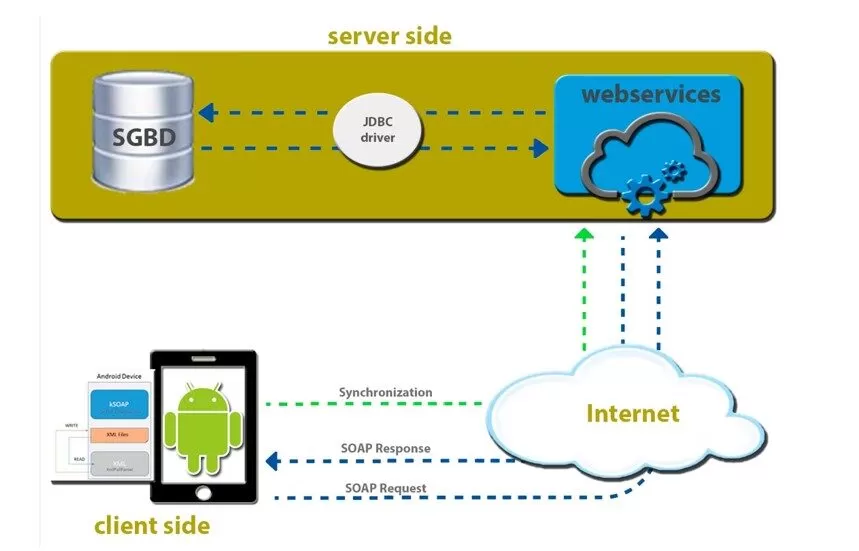
To accomplish the desired interoperability among the different developed components, we have used Web Services (SOAP approach) for a distributed system support, and XML files to store data locally. In the case of the developed App, the data inserted by the user are in first place recorded in a XML file; also, if the web service and Internet connection are, the data will be read and manipulated by the web service. Using the mechanisms provided by the server will be possible to manipulate the database. If the data has been recorded only in the offline mode, we start the synchronization with the database as soon the device has Internet Connection; this will keep all the information homogeneous. Figure 4 present the technological framework used to develop the prototype. The framework presents the client and server components as well as highlighting the main technologies and protocols used in the design of the solution that was implemented.
Fig. 4: Proposed Technological Framework
Mobile Applications Developed
This prototype provides seniors with a way to record medication intake, record daily monitors that are requested by their physician, and make pre-defined service requests by their supervisor. The daily monitoring log generates a report to inform the family doctor or hospital emergency. This data will allow the implementation of treatments with greater precision. It also allows users to record their daily status so that their supervisor regularly checks and understands their progress.
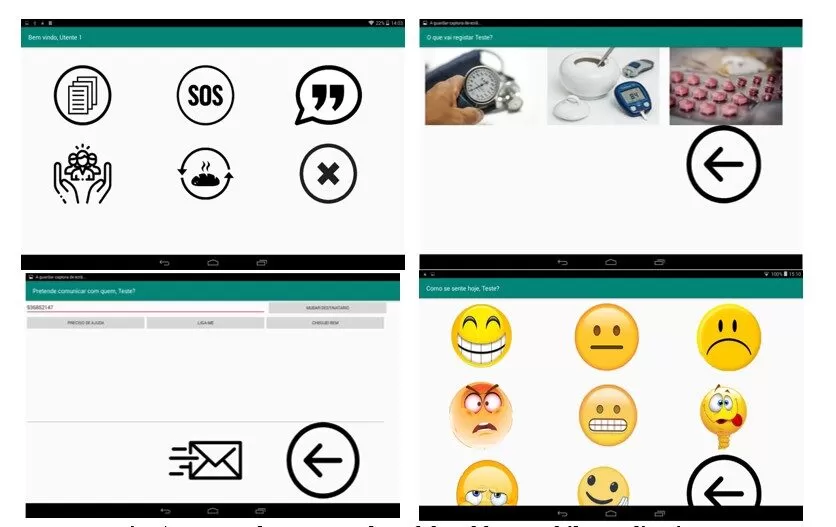
In the main menu we have access to all project group functions letting the user to access a screen and manage the various services that will simplify their daily activities (e.g. Meds Checking, SOS Requests, Messages, Daily Feeling Status or Various Requests). In figure 5 are presented some screenshots that exemplify the Mobile device application developed for the elders. This was planned to be installed in a tablet device, because these devices have bigger screens, compare to smartphones and so it would be easier to use by the elderly.
Fig. 5: Screenshots Examples of the Elders Mobile Application
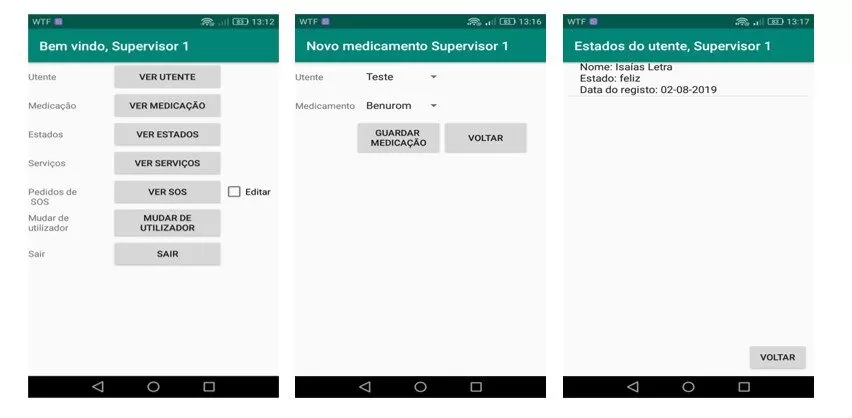
In Figure 6 are presented some screenshots examples of the mobile application developed for caregivers and family supporters that will be able to follow the elder’s daily routines and retrieve useful information (e.g. health parameters measured, important requests).
Fig. 6: Screenshots Examples of the Caregivers/Family Mobile Application
This prototype is meant to be a valuable one for those who cannot keep up with their relatives with multi-level or accompanying needs. This enables them to analyse how their relatives are feeling, attend to their needs and requests, or even generate pdf lists with measured parameters that will be very useful for caregivers to act promptly and properly.
This prototype also increases the need to perform the necessary checks, registering them in a database motivating a better elders’ supervision.
Conclusion and Final Remarks
By promoting a more active, and also decentralized, aging we will contribute to increase the satisfaction of the elderly population and help to optimize health resources, that are scarce. Also, it will promote a more active and committed role for citizens that will become more aware and more collaborative, given the increase of their empowering in the self-monitoring and self-reporting of their own health and needs (Cunha et. al., 2018). The role of applications supported by mobile devices has shown an important potential not only because of the easier interaction they bring, but also, because mobile devices are embedded in people’s daily routines. Building software and hardware solutions that can assist elders in their health-related responsibilities and bridging the gap between elders, caregivers and elders’ families seem today an enormous opportunity to solve the majority of rural elder’s isolation problems.
This paper has reviewed the gerontechnology concept and briefly characterized some most important demographic characterization of the Portuguese Northeast region – a deeply rural region – and presented a prototype based in mobile devices applications capable of managing elders’ health daily routine tasks and also increasing the proximity level among elders, caregivers and families or elders’ tutors. This work represents a major and wider effort to promote, in rural areas, the use of suitable and effective technology approaches to increase equality among citizens in the access to quality of life, care and health. Also, this work untapped the business opportunities that can be enhanced through the integration of services providers on caregivers’ IT platforms.
Acknowledgments
UNIAG, R&D unit funded by the FCT – Portuguese Foundation for the Development of Science and Technology, Ministry of Science, Technology and Higher Education. UID/GES/4752/2019.
Foot Notes
INE (2019). Estimativas anuais da população residente (updated, 2019). Retrieved from http://www.ine.pt
INE (2019). Estimativas anuais da população residente (updated, 2019). Retrieved from http://www.ine.pt
INE (2019). Índice de envelhecimento (N.º) por Local de residência (NUTS – 2013) (updated, 2019). Retrieved from http://www.ine.pt
References
Concepción, M., Morillo, L., Garcia, J. and González-Abril, L. (2017). Mobile activity recognition and fall detection system for elderly people using Ameva algorithm, Pervasive and Mobile Computing, Volume 34, Pages 3-13, ISSN 1574-1192
Costa, A., Julián, V., and Novais, P. (2017). Advances and trends for the development of ambient‐assisted living platforms. Expert Systems. doi: 1111/exsy.12163.
Cunha, L., Pereira, F., & Loureiro, A. (2019). Educação para o suporte social e satisfação com a vida em idosos. In Barroso, A., Hoyos, A., Salmazo-Silva, H., & Fortunato, I. (org.). Diálogos Interdisciplinares do Envelhecimento. São Paulo: Edições Hipótese.
Cunha, C. R.; Mendonça, V.; Morais, E. P.; Fernandes, J. (2018). Using pervasive and mobile computation in the provision of gerontological care in rural áreas. In International Conference on ENTERprise Information Systems, International Conference on Project Management, International Conference on Health and Social Care Information Systems and Technologies, CENTERIS/ProjMAN/HCist 2018. Lisbon. Procedia Computer Science. ISSN 1877-0509. 138, p. 72-79
Deist, F.; Latouille, M. (2016). Acceptability Conditions for Telemonitoring Gerontechnology in the Elderly, IRBM, vol. 37, Issue 5, 2016, pp. 284-288, ISSN 1959-0318.
Diaconu, L. (2015). Ageing Population: Comparative analysis among European Union States. Centre for European Studies, Iasi, 7(1), pp. 50-59.
Espín, V., Hurtado, M., and Noguera, M. (2016). Nutrition for Elder Care: a nutritional semantic recommender system for the elderly. Expert Sys: J. Knowl. Eng. 33, 2 (April 2016), 201-210. DOI: https://doi.org/10.1111/exsy.12143
Fernández‐Caballero A, González P, Navarro E. (2017). Gerontechnologies – Current achievements and future trends. Expert Systems. 34: e12203. https://doi.org/10.1111/exsy.12203
Ferreira, F.; Dias, F.; Braz, J.; Santos, R.; Nascimento, R; Ferreira, R.; Martinho, R. (2013): A Mobile Health Application for the Elder-caregiver Monitoring Paradigm, Procedia Technology, vol. 9, pp. 1361-1371, ISSN 2212-0173.
Fischer, S. H.; David, Crotty, D.; B. H.; Dierks, M.; Safran, C. (2014). Acceptance and use of health information technology by community-dwelling elders, International Journal of Medical Informatics, vol. 83, Issue 9, pp. 624-635, ISSN 1386-5056.
Fonseca, M. (2016). Envelhecimento em meio rural: estudo das redes sociais de suporte dos idosos a usufruir de serviço de apoio domiciliário, no centro social e polivalente de EGA (Dissertação de mestrado). Retrieved from http://hdl.handle.net/11067/4305
Graafmans J, Taipale V. Gerontechnology (1998). A sustainable investment in the future. Stud Health Technol Inform; 48: 3–6.
Halicka, K. (2019). Gerontechnology — the assessment of one selected technology improving the quality of life of older adults, Engineering Management in Production and Services, 11(2), 43-51. doi: https://doi.org/10.2478/emj-2019-0010
Hartmann J, J. & Gomes, G. (2014). Depression in institutionalized elderly: the singularities of grief seen in its diversity. Sociedade Brasileira de Psicologia Hospitalar, 17(2).
Kemperman, A., van den Berg, P., Weijs-Perrée, M., & Uijtdewillegen, K. (2019). Loneliness of Older Adults: Social Network and the Living Environment. International journal of environmental research and public health, 16(3), 406. doi:10.3390/ijerph16030406
Lago, P., Jiménez-Guarín, C. and Roncancio, C. (2015). Contextualized Behavior Patterns for Ambient Assisted Living. In Proceedings of the 6th International Workshop on Human Behavior Understanding – Volume 9277, Albert Ali Salah, Ben J.A. Kröse, and Diane J. Cook (Eds.), Vol. 9277. Springer-Verlag New
York, Inc., New York, NY, USA, 132-145. DOI=http://dx.doi.org/10.1007/978-3-319-24195-1_10
Lazakidou A, Siassiakos K, Ioannou K. (2011). Wireless Technologies for Assisted Living and healthcare: Systems and Applications. Medical Information Science Reference.
Mostaghel, R. (2016). Innovation and technology for the elderly: Systematic literature review, Journal of Business Research, vol. 69, Issue 11, November 2016, Pages 4896-4900, ISSN 0148-2963.
Neville, S., Adams, J., Napier, S., Shannon, K., & Jackson, D. (2018). “Engaging in my rural community”: perceptions of people aged 85 years and over. International Journal of Qualitative Studies on Health and Well-being, 13(1). DOI: 1080/17482631.2018.1503908
Pince M, Wimo A, Guerchet M, Ali Gemma-Claire, Wu YT, Prina M. (2015). World Alzheimer Report 2015. Chapter 2. pages 10-27.
Quinn, S., Bond, R., and Nugent, C. (2017). Ontological modelling and rule‐based reasoning for the provision of personalized patient education. Expert Systems, 34: e12134. doi: 1111/exsy.12134.
Sheets DJ, La Buda D, Liebig PS. (1997) Gerontechnology. The aging of rehabilitation. Rehab Manag; 10: 100–2.
Siegel, C.; Dorner, T. E. (2017). Information technologies for active and assisted living—Influences to the quality of life of an ageing society, International Journal of Medical Informatics, vol. 100, pp. 32-45, ISSN 1386-5056.
Soar, J.; Seo, Y. (2007). Health and aged care enabled by information technology, Annals of the New York Academy of Sciences, 1114 (2007), pp. 154–161.
Smith A. (2014). Pew Research Center. Older adults and technology use. [Available at: http://www.pewinternet.org/2014/04/03/older-adults-and-technology-use/ (Access date: 9 April 2019)