RISEBA University of Applied Sciences, Riga, Latvia
Volume 2022,
Article ID 799143,
IBIMA Business Review,
15 pages,
DOI: 10.5171/2022.799143
Received date: 18 November 2021; Accepted date: 22 January 2022; Published date: 10 March 2022
Cite this Article as:
Kirathimo Muruga (2022)," Effect of Covid-19 Pandemic on Health Systems ", IBIMA Business Review, Vol. 2022 (2022), Article ID 799143, DOI: 10.5171/2022.799143
Research motivation: The current study sought to investigate the effect of Covid-19 pandemic on Health systems and its management in Kenya. Research methodology: The proposed choice of research design was descriptive design. This study is based in the Kenyan context with evidence being based on the influence of Covid-19 globally. The study is thus qualitative with a focus on key respondents that is the health practitioners in the health facilities handling the COVID-19. The targeted population are both public and private healthcare providers in the health facilities in Kenyan hospitals. The study targeted all health care practitioners from the Kenya Medical Practitioners and Dentists Council (KMPDC) doctors’ retention register. The data were collected by the use of an interview guide which was aided by the help of research assistants. Data were processed using the content analysis and the results were presented in the form of content and/or thematic format. Main findings and implications: From the findings, the study concludes that Covid-19 has significantly affected the health system. In this regard, the healthcare facilities have received the allocated finances to help cub COVID-19 from the ministry of health. For those who did not receive the funds, it was noted that they manage COVID-19 by other means such as Readjustments, operation-wise and financially, Funding from donors and charities. Measures to ensure that the allocation of funds and resources necessary to combat COVID-19 need to be made available and accessible to all the hospitals in the country.
Keywords: Covid-19 pandemic, Health systems, Health management
Introduction
Covid-19 is a family of Coronaviruses (COV) – a large family of viruses that cause illness ranging from the common cold to more severe respiratory diseases. It is referred to as severe acute respiratory syndrome coronavirus 2 – SARS-CoV-2; formerly called 2019-nCoV (WHO, 2020). The 2019 novel outbreak of coronavirus disease (COVID-19), which emerged in 2019 from Wuhan city, China, has now spread exponentially from more than one continent and is now on a global scale. As such, on 30 January 2020, the World Health Organization declared coronavirus disease 2019 (COVID-19) outbreak a public health emergency of international significance (Gilbert et al., 2020).
Worldometer reports, as at 15th April, indicated total global confirmed coronavirus cases of up to 2,000,231, with 126,758 deaths and 484,729 recoveries. Europe topping the list with 1,015,507 and 92,224 total cases and deaths respectively; North America with 724,560 and 36,709 total cases and deaths respectively; Asia with 345,970 and 12,426 total cases and deaths respectively South America with 67,591 and 3,057 total cases and deaths respectively and Africa with 18,993 and 968 total cases and deaths respectively (Worldometer, 2020). Due to its rapid and fatal health effects, WHO estimated the novel coronavirus’ case fatality rate at around 2%. The worst part of the virus is that the symptoms of COVID-19 may appear in as few as 2 days or as long as 14 (estimated ranges vary from 2-10 days, 2-14 days, and 10-14 days), during which the virus is contagious but the patient does not display any symptom.
WHO has scaled up strategic objectives to respond to the spread of COVID-19 by interrupting human-to-human transmission including reducing secondary infections among close contacts and health care workers, preventing transmission amplification events, and preventing further international spread as well as identifying, isolating and caring for patients early, including providing optimized care for infected patients. These measures have forced world populations to quarantine, physical social distancing, and countries that are severely hit with COVID-19 infections have been forced to partial and/or total lockdowns (WHO, 2020).
The social distancing, quarantine (both mandatory and voluntary), as well as lockdowns, proved to be one of the world’s most psychological and economic experiment where the most established as well as the developing economies are put to the ultimate test. Sustaining the citizens (economic wise as well as health-wise) in the lockdowns proves to be even harder. In treating the COVID-19 pandemic, the world was scrambling to build enough tents to treat those infected with a deadly, highly contagious virus. Epidemics, of the size of COVID-19, have huge economic and health impacts – not just from the costs of managing the health of people, but stopping them, and keeping the economy working. The steep fall in global stock markets, since it became clear that COVID-19 would not be limited to China, has boldly highlighted the need for a vaccine (taking into consideration that there is no vaccine yet for the virus) and containment of the disease (WHO, 2020; CDC, 2020).
The first critical task for financial sectors and central banks was to support the best possible financial assessment of strict management measures (trying to isolate each potential case) versus the management of the outbreak (delaying the spread of the virus, protecting the most fragile and curing the sick, while allowing the majority of people to continue their everyday lives). The crumbling of the economy is interlinked and/or a derivative of the health of the workforce in a given economy/country/state. Together with health professionals, financial sectors play a full role in educating political leaders on this crucial decision, considering the economic and health implications. In addition, they must guarantee sufficient support for a response to public health. Measures that can make a significant change to the effectiveness of containment approaches, such as improving tracking and ensuring the availability and accessibility of test kits and protective gear for front-line health staff, must not fail due to a lack of resources (Chatham House 2019).
Statement Of the Problem
Almost every country/nation has been caught unaware of the ripples sent across the globe by the virus. The unpreparedness elicited fear in the health sector, where many healthcare facilities were found not to have adequate facilities to manage the virus. Coronavirus Disease 2019 (COVID-19) created an economic crisis alongside a health crisis. During the two weeks that ended on March 28, nearly 10 million people applied for unemployment insurance, dwarfing any previous monthly numbers (Cutler, 2020). There were no commercially available medicinal treatments or vaccines for COVID-19 prevention, treatment and/or control. The Centres for Disease Control and Prevention (CDC) and the World Health Organization (WHO) were hopeful that most infected persons with the COVID-19 virus will experience mild to moderate respiratory disease and bounce back without requiring special treatment. However, elderly people, as well as those with underlying medical issues such as cardiovascular disease, diabetes, chronic respiratory diseases and cancer, are more likely to develop serious illnesses (WHO, 2020; CDC, 2020). COVID-19 is believed to have a higher mortality rate than seasonal influenza, even though large variations are confirmed. This was also predicted by the World Health Organization (WHO) that global mortality would be around 0.6% in countries like South Korea the case at 3.4% (Bai et al., 2020). Vaccine development and medical treatment research for COVID-19 are underway, but there are many unknown months away (WHO, 2020).
The lockdowns also meant a long-term unsustainable economy which result in unsustained health system. As Cutler (2020) points out, businesses can only survive a short time without customers, longer with the relief bills among others. But sustained shutdowns were becoming more and more painful. As time passes, relief checks are going to be exhausted. Without access to credit, some retailers (maybe including medical offices) are set to shut down permanently. For example, travel bans and lockdowns in Africa interrupted distribution networks exposed to inputs from Asia, Europe and the Middle East, as well as crush demand in global markets for a wide range of African exports. Besides, Africa encountered delayed or reduced foreign direct investment (FDI) as partners from other continents redirect capital locally (Sunn, 2020).
Thus, given the uncertainties of the virus and its catastrophic impacts, countries relied on behaviour change and non-pharmaceutical interventions, including, amongst others, self-isolation of symptomatic individuals; increased hand hygiene; physical social distancing; working from home where possible; and school and business closure. It is no longer an issue to be dealt with by the Ministries of health, national public health institutes, universities and other public health agencies, but it has started to consume the economic activities, and without urgent action, the socio-economic effects could have wide implications for trade, travel, provision of aid, economic markets, supply chains and the daily lives of people living around the world. Given that most African Countries are reliant on small enterprises, working from home comes at the expense of them putting a meal on the table. In addition, an ailing country implies an unsustained economy. Therefore, the current study sought to find out the effect of COVID-19 pandemic on Health systems and Economies. However, this paper is just the not the first one and further research and studies will follow.
Literature Review
Effect of COVID-19 pandemic on Health Systems
Meanwhile, strains continue to pile up on the global health care workforce. There are 2 ways to this strain. The first is the increasingly excessive pressure of diseases that burdens the capability of the health system and the second is the negative effects on health care staff, including the risk of infection. An estimated 3,000 health-care workers were contaminated in China and at least 22 died. The World Health Organization advises caution in caring for all patients with respiratory symptoms (such as masks, gloves, gowns, and eyewear). Health care providers who meet any patient with respiratory disease should wear a mask and gloves as prescribed, or goggles. Nevertheless, the supply, availability and accessibility of N95 masks, respiratory isolation rooms and powered air-purifying respirator (PAPR), especially in ambulatory offices, is limited to feasibly evaluate any patient with respiratory disease and such steps are not routinely essential (Adams & Walls, 2020).
Since February 21, 2020, when the first COVID-19 incident was reported in Italy, the National Healthcare Service has faced rising strain/pressure, with 165,155 total COVID-19 cases and 21,645 deaths as of April 16, 2020. The National Healthcare Service was almost crumbling in the regions most affected. In daily news and records, a number of healthcare professionals have noted the need to leave the hospital units distressed, traumatized and overwhelmed because of the patients who die at their watch with little in their power to help (Armocida, Formenti, Ussai, Palestra & Missoni, 2020). This drastic rise in cases poses multiple obstacles even for the most sophisticated and developed health systems, like the United States, Spain, Germany, UK as well as France. As of 16 April 2020, the total number of confirmed new cases and deaths was 180,659, and 18,812. Spain in April was the second leading country after the USA with a troubling 644,348 reported total incidents (Worldometer, 2020). Health-care staff in Spain have worked hard to support patients in difficult conditions. This forced the Government to change its response and implement strict lockdown policies that helped slow the spread of the virus and gain time to restructure its healthcare system (World Health Organization, 2020).
In Ecuador, desperate families and neighbours flooded social media with videos and cries of corpses rotting in their living rooms, on sidewalks and in parks for days due to the overwhelmed hospitals and morgues. Currently, Ecuador has recorded a total of 7,858 cases while 388 total deaths (Lobo, 2020). In the UK, the virus is on the verge of making homeless and orphans out of children most of the years below 5 years. Furthermore, there are a number of major direct and indirect safety, social and educational implications for homeless children and families living in temporary or unhealthy accommodation (such as staying with friends or relatives, surfing couch, tents, bed and breakfast accommodation). Owing to pre-existing conditions (such as diabetes, asthma, autism, anxiety, depression), these children are more vulnerable to viral infection (Rosenthal et al., 2020).
The consequences of the COVID-19 pandemic have been seen to ravage not only an individual’s physical wellbeing but also the mental health of the infected (and recovered) as well as those affected. However, the severity of the impact cannot be underestimated. Daily reports of growing illnesses and deaths worldwide increase fear among people and plug us into mourning in cases of personal loss. The key reason is that there is no assurance about tomorrow; about our families, friends and loved ones’ health and safety; and about our ability to lead the lives that we enjoy (Pfefferbaum & North, 2020). With overburdened hotlines and healthcare systems, patients seeking medical treatment can fall by the wayside for other critical, non-COVID-19 related problems. In March, a 28-year-old man who returned from Zanzibar to London died of malaria, having failed to reach the NHS hotline due to COVID-19 related calls volume (WHO, 2020).
In the US, the federal government early this April reacted by lowering interest rates and flooding the markets with cash. On the fiscal side, Congress released the largest aid bill in history; that is the $2 trillion relief bill that generates cash to most U.S. households, small business loans, and $100 billion allocated for COVID-19 distressed hospitals (Cutler, 2020). Governments took actions by closing schools (Bayham & Fenichel, 2020). Owing to the inadequate capacity of the official health care units, such services in African countries like Kenya are already set up as health care centres. Public areas such as stadiums and other sporting centres around the world are being turned into alternative temporary hospitals to relieve the pressure that hits the healthcare systems. For instance, Wuhan converted one of its major sports complexes into a hospital when the epidemic escalated. As per the Philippine Sports Board, two National Sports Complexes (one in Manila and one in Pasig City) have been turned to hospitals. The most famous stadium in Brazil, the Maracanã in Rio, is now a field hospital; a temporary facility is also being built in a Stadium in Sao Paulo. Wales’ health minister approved funding for the construction of a 2,000-bed hospital at Principality Stadium, the national stadium, which has a retractable roof. Santiago Bernabéu, Real Madrid stadium, is set to store emergency supplies (Gregory, 2020).
In Africa, it is difficult to gauge the number of unconsciously circulating COVID-19 cases in the population, thus, in the weeks ahead, health systems in Africa will have to brace for a possible surge in serious cases of typical pneumonia and respiratory failure (Harries, Martinez & Chakaya, 2020). A well-functioning health system, however, is dependent on a multitude of factors including skilled and empowered health personnel, excellently-maintained facilities, and a secure supply of medications and personal protective equipment, which must be accompanied by sufficient resources and effective strategic programs. Given most advanced health systems being brought to their knees in Europe as well as the USA, there is more reason for African countries to buckle up their containment and mitigation strategies (Paintsil, 2020).
In preparation for the inevitable importation of SARS-CoV-2 to Africa, on 3 February 2020, the Africa CDC, in cooperation with the WHO and African countries, set up the Novel Coronavirus Task Force. The African Task Force had six approaches: laboratory diagnosis; surveillance, namely screening at entry points and cross-border tasks; control and prevention of infections in medical centres; clinical management of individuals with extreme COVID-19; risk awareness and community involvement; and supply chain management and stockpiles (WHO, 2020; CDC, 2020).
Drawing evidence from the outbreaks of severe acute respiratory syndromes (SARS) in 2003 and Influenza A Virus Subtype H7N9 (H7N9) in 2013, China had been greatly impacted by the negative health, economic, and even national and even international security impacts of the diseases (Qiu, Chu, Mao & Wu, 2018). Although the U.S. general population’s 2009 H1N1 pandemic was mild in terms of overall morbidity and mortality, extreme outcomes from H1N1pdm09 virus infection were more frequent among infants, youth, and particular groups at risk of severe complications (such as pregnant women) than among older adults (Sambala, et al., 2018). However, the case is not with Covid-19, since the risk befalls greatly the elderly compared to the young persons. These pandemics are a reminder to be prepared for the unpredictable nature of pandemics. The increased demand arising from COVID-19 is likely to cripple troubled healthcare systems in less developed countries. For instance, in West Africa, access to health care facilities was cut by 50 per cent during the 2014–15 Ebola epidemic, exacerbating malaria, HIV / AIDS and mortality rates for tuberculosis. The indirect effect of other diseases on mortality significantly surpassed the number of Ebola-caused deaths (Parpia, Ndeffo-Mbah, Wenzel & Galvani, 2016).
The proliferation and crippling effects of coronavirus strike cause politicians and soccer players as well as other high-profile athletes to take pay cuts to help so that the finances can be used to save lives in the health sectors. France, Italy and Spain, which have been the most affected by the virus in Europe so far, are among the countries calling for joint debt sales to pay for recovery efforts, but they are resisting the attempts of northern states, including Germany, to help collective debt issuance (ILO, 2020). The limiting conditions of the Virus in Nigeria were expected to aggravate the country’s debt profile. For instance, due to the introduced lockdowns, the decline in domestic consumption in Nigeria was expected to result in households spending predominantly on basic commodities; the drop in projected incomes, especially for employees employed on a contract basis, as well as the depletion of wealth and expected wealth as a result of the collapse in assets such as stocks Investments are unpredictable given the pandemic-limited awareness of the extent of the epidemic, the efficacy of policy measures and the economic agents’ reaction to those measures (Onyekwena, 2020). Therefore, for the governments that are commodity-dependent, the fall in the global demand for commodities stemming from the pandemic significantly increased their fiscal deficits.
COVID-19 has shown its probable devastating effect, but it is a cause of great concern particularly in African countries such as South Africa and Egypt. The total number of Covid-19 cases in Egypt by April 2020, was at the top of the African chart after Egypt (Worldometer, 2020). With the first case reported on the continent with an infected individual being identified in Algeria, the epidemic started to hit the ground quickly in other nations, especially in Egypt, South Africa, and Morocco. For example, the total number of confirmed cases in Africa as at 15 April 2020 stood at 16,873 with Egypt at 2,673 at the front with 2,415, followed by South Africa at 2,605 and Morocco at 2,283 confirmed Covid-19 cases (Worldometer, 2020).
Almost all African countries are, therefore, disadvantageous in many areas, from basic hygiene requirements to health facilities at a national and local level. Other essential and worrisome factors include the existence of persons living in unfavourable conditions in major cities, as well as communities of displaced people in sub-Saharan African countries, forced to migrate to other countries and forced to live in non-sterile camps. If the virus spreads to these areas where these people in the camps are struggling for life, what both the host countries and the international community can do may require serious restrictions and drastic measures (The World Bank, 2020).
Notwithstanding all these concerns, Africa has some benefits over the outbreak in Asia, Europe and the Americas. The first is the recent experience of the continent with viruses such as Ebola, AIDS, malaria and Lassa fever. Evidence provides the continent with significant infrastructural room for help to deal with outbreaks, but inadequate health equipment and clean drinking water across much of the continent are issues of concern. On the other hand, the fact that COVID-19 spread to African countries later than other regions around the world was also seen as an advantage in the fight against the disease outbreak since the governments stand a better chance of benchmarking the virus spreading (WHO, 2020).
For instance, to help Ethiopia mitigate the effects of the COVID-19 pandemic in the country, the World Bank Group’s Board of Executive Directors on 2nd April 2020 approved $82.6 million ($41.3 million grant and $41.3 million credit) from the International Development Association. The World Bank Group is rolling out a $14 billion fast-track package to strengthen the COVID-19 response in developing countries and shorten the time to recovery. The immediate response includes financing, policy advice and technical assistance to help countries cope with the health and economic impacts of the pandemic. In addition, The International Finance Corporation provided $8 billion in financing to help private companies affected by the pandemic and preserve jobs (The World Bank, 2020).
Likewise, in Kenya, the World Bank Group Board of Directors approved today $50 million in immediate funding to support Kenya’s response to the global COVID-19 (coronavirus) pandemic under a new operation – the Kenya COVID -19 Emergency Response Project. The project was set to provide emergency funding for medical diagnostic services, surveillance and response, capacity building, quarantine, isolation and treatment centres, medical waste disposal, risk communications and community engagement as well as for strengthening the country’s capacity to provide safe blood services (The World Bank, 2020). The ability of countries to mount the required fiscal response was highly contingent on ample external financing and grant on concessional terms being made available by the international financial community. Without adequate financing, temporary liquidity issues could turn into solvency problems, resulting in the COVID-19 crisis having long-term pressure and negative implications on health departments (IMF, 2020).
Consequently, the real cost of COVID-19 would be much larger than the direct health costs associated with handling cases. Indeed, the indirect cost of the illness will greatly outweigh the expense of medical testing, diagnosis, and hospitalization. The scale of these administrative costs, including economic harm, will rely on how prolonged the pandemic is, the effectiveness of the measures taken by governments to contain it, the effect and collective compliance to behavioural measures such as physical distance implemented by officials and how much economic assistance governments and development agencies are prepared to mobilize and allocate during the immediate impact of this pandemic. The availability of effective treatments and vaccines, as well as new diagnostic tests, will also determine the level of non-pharmaceutical interventions (NPIs) that will need to be retained.
Methodology
The proposed choice of research design was descriptive design as it seeks to explain the state of affairs through a process of data collection to describe the situation as it is. This study is based in the Kenyan context with evidence being based on the influence of Covid-19 globally. The study is, thus, qualitative with a focus on key respondents that are the health practitioners in the health facilities handling the CVID-19. The targeted population were both public and private healthcare providers in the health facilities in Kenyan hospitals. The study targeted all health care practitioners from the Kenya Medical Practitioners and Dentists Council (KMPDC) doctors’ retention register. The selection was scientifically guided using Fisher’s formula (Fisher, 1956, Fisher, 1962). The Fisher formula is as follows:
Where;
n= sample size
z= the standard normal deviate value for the level of confidence, for instance 95% level of confidence =1.645.
d= margin of error or level of precision at 0.1 for CI at 95%
p= proportion to be estimated, Israel and Duffy (2009) recommend that if you don’t know the value of p then you should assume p=0.5.
Substituted as in:
Therefore:
n = 68 respondents
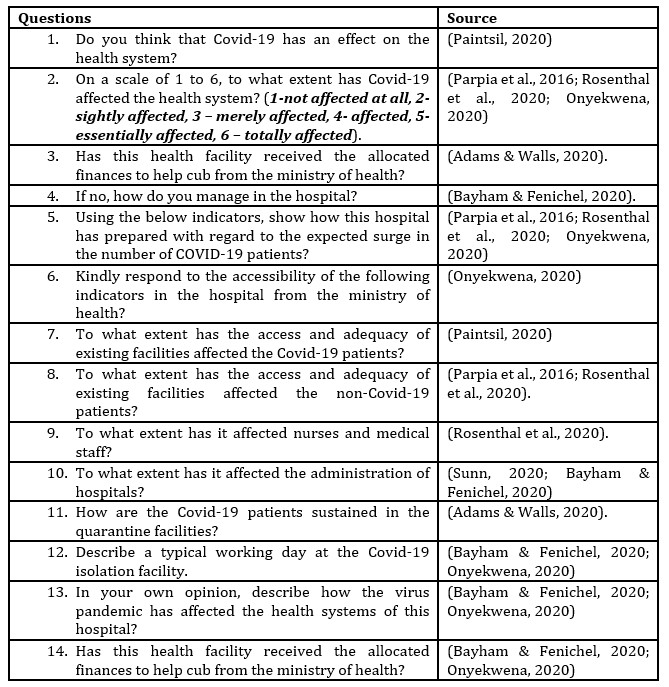
The respondents were then randomly and conveniently selected to respond to the questions. Random sampling ensured the element of bias is eliminated and thus equal chances of participation were provided. The data were collected by the use of an interview guide which was aided by the help of research assistants. Data collection was done by use of google surveys where emails were sent to the selected respondents. Prior to sending the questionnaires in Goole survey format, the researcher sought ethical approval from the Riseba University, ethical review committee, the National Commission for Science and Technology (NACOSTI) and from individual respondents set out to conduct the actual data. The researcher trained and acquainted 2 research assistants on how to collect the data and this ensured professionalism. Data were processed using the content analysis and the results were presented in the form of content and/or thematic format. Below is a table showing how the questions were sourced and modified:
Table 1: Source of Questions
Source, Research Data (2020)
Results
Response Rate
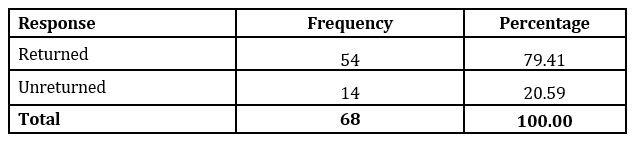
Table 2: Response Rate
Source, Research Data (2020)
The results in Table 2 show that 68 questionnaires were given out and 54 were properly filled and returned. This return saw 79.41% response rate which is adequate. This is so because according to Allen (2016) and also Rindfuss (2015), a response rate of above 50% is adequate for a descriptive study.
Effect of Covid-19 on the health system
The health care practitioners were asked to indicate whether Covid-19 has an effect on the health system. From the study, the findings indicated that all of them were in agreement that Covid-19 has an effect on the Kenyan health system.
Extent to which Covid-19 has affected the health system
On a scale of 1 to 6, the healthcare professionals were asked to indicate the extent to which has Covid-19 affected the health system. Their responses are as shown below:
Table 3: Extent to which Covid-19 has affected the health system
Note: 1= not affected at all, 2= sightly affected, 3 = merely affected, 4= affected, 5= essentially affected, 6 = totally affected, F=Frequencies, P= Percentage, M= Mean, SD= Standard Deviation
Source, Research Data (2020)
The findings indicate that the majority of the respondents 47 (87%) agreed that Covid-19 affected the health system to a great extent. This was supported by a mean of 4.93 indicating that the majority of the responses were in agreement.
Receipt of the allocated finances to curb COVID-19
The health care practitioners were requested to indicate whether their facilities have received the allocated finances to help cub COVID-19 from the ministry of health. Their responses are as shown in Table 4 below:
Table 4: Receipt of the allocated finances to curb COVID-19
Source, Research Data (2020)
The results in the table above reveal that 88.89% of the respondents agreed that their facilities have received the allocated finances to help cub COVID-19 from the ministry of health. For those who did not receive the funds, it was noted that they manage COVID-19 by other means such as Readjustments, operation-wise and financially, Funding from donors and charities
Preparedness of the Hospital to Curb COVID-19
Using the indicators in the table below, the respondents were likewise asked to show how their hospitals have prepared with regard to the expected surge in the number of COVID-19 patients.
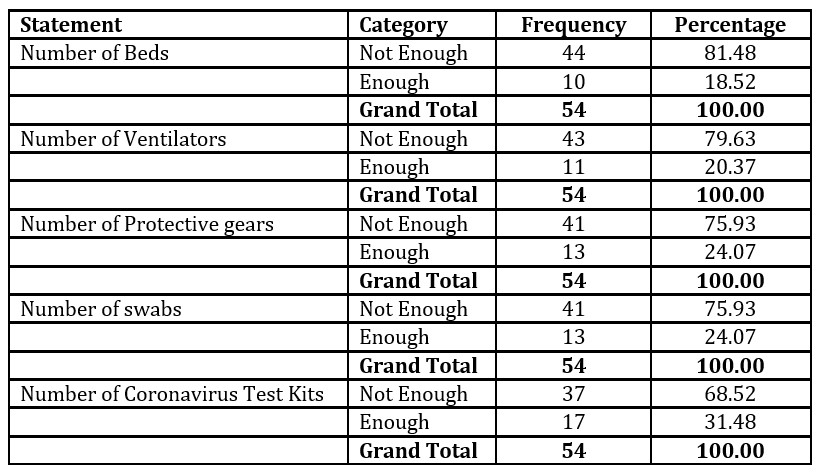
Table 5: Preparedness of the Hospital to Curb COVID-19
Source, Research Data (2020)
The findings revealed that 81.48%, 79.63%, 75.93%, 75.93% and 68.52% indicated that the hospitals had insufficient number of beds, number of ventilators, number of protective gears, number of swabs and number of coronavirus test kits respectively.
Accessibility of Hospital Equipment to Curb COVID-19
The healthcare practitioners were likewise asked to respond to the accessibility of the following indicators in the hospital from the ministry of health.
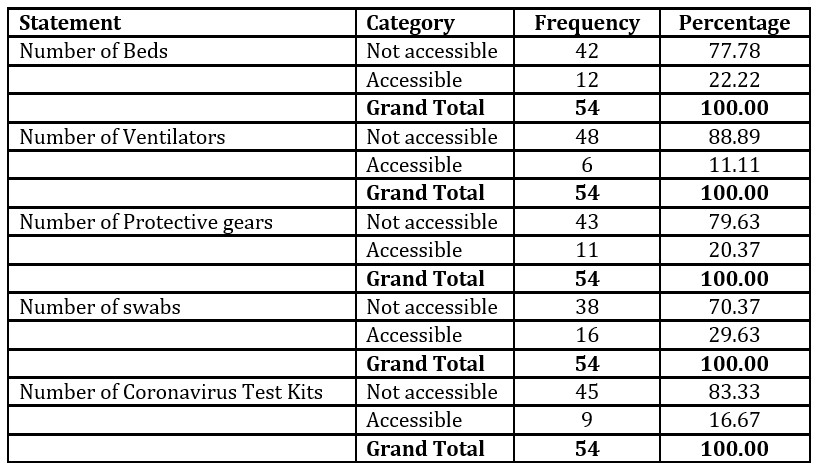
Table 6: Accessibility of Hospital Equipment to Curb COVID-19
Source, Research Data (2020)
The findings revealed that 77.78%, 88.89%, 79.63%, 70.37% and 83.33% indicated that the number of beds, number of ventilators, number of protective gears, number of swabs and number of coronavirus test kits respectively were not accessible.
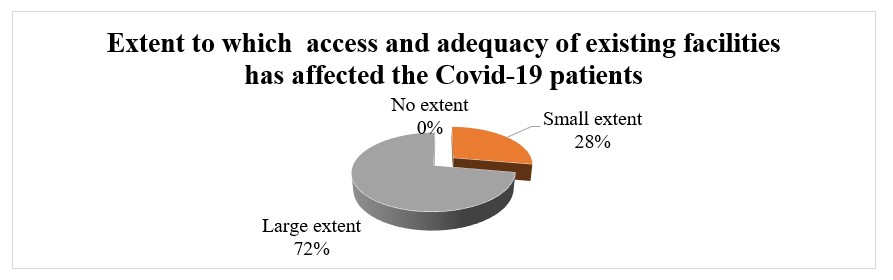
Extent to which access and adequacy of existing facilities has affected the Covid-19 patients
The healthcare practitioners were also asked to indicate to what extent the access and adequacy of existing facilities has affected the Covid-19 patients.
Figure 1: Extent to which access and adequacy of existing facilities has affected the Covid-19 patients
Source, Research Data (2020)
The findings revealed that 72% of the healthcare practitioners indicated that the access and adequacy of existing facilities has affected Covid-19 Patients to a greater extent while 28% indicated that it has affected Covid-19 Patients to a small extent.
Access and Adequacy of Existing Facilities to Non Covid-19 Patients
The healthcare practitioners were asked to indicate the extent to which the access and adequacy of existing facilities has affected the non Covid-19 patients
Table 7: Access and Adequacy of Existing Facilities to Non Covid-19 Patients
Source, Research Data (2020)
The findings revealed that 83.33% of the healthcare practitioners indicated that the access and adequacy of existing facilities has affected non Covid-19 Patients to a greater extent while 16.67% indicated that it has affected non Covid-19 Patients to a small extent.
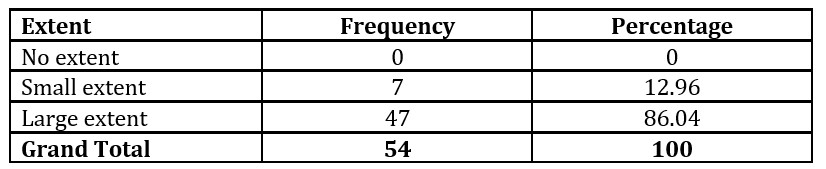
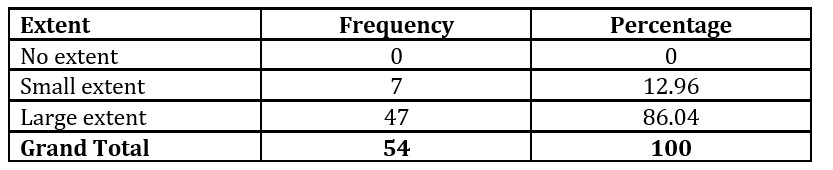
Access and Adequacy of Existing Facilities to Nurses and Medical Staff
The healthcare practitioners were asked to indicate the extent to which the access and adequacy of existing facilities has affected nurses and medical staff.
Table 8: Access and Adequacy of Existing Facilities to Nurses and Medical Staff
Source, Research Data (2020)
The findings revealed that 86.04% of the healthcare practitioners indicated that the access and adequacy of existing facilities has affected nurses and medical staff to a greater extent while 12.96% indicated that they have been affected to a small extent.
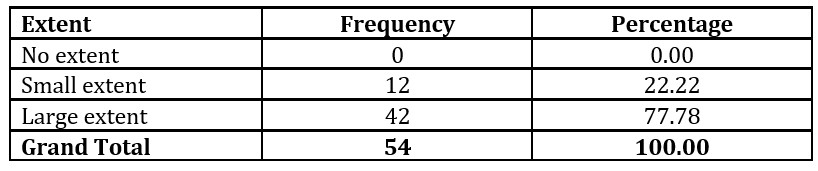
Access and Adequacy of Existing Facilities to Administration of Hospitals
The healthcare practitioners were also asked to indicate the extent to which the access and adequacy of existing facilities has affected the administration of hospitals.
Table 9: Access and Adequacy of Existing Facilities to the Administration of Hospitals
Source, Research Data (2020)
The findings revealed that 77.78% of the healthcare practitioners indicated that the access and adequacy of existing facilities has affected the administration of hospitals to a greater extent while 22.22% indicated that the administration of hospitals has been affected to a small extent.
Covid-19 patients’ sustenance in the quarantine facilities
The healthcare practitioners were also asked to indicate how the Covid-19 patients are sustained in the quarantine facilities.
Table 10: Covid-19 patients’ sustenance in the quarantine facilities
Source, Research Data (2020)
The findings revealed that 57.41% of the healthcare practitioners indicated that the Government has taken care of the costs while 42.59% indicated the patients pay from their personal expenditure.
The healthcare providers were asked to describe a typical working day at the Covid-19 isolation facility. The majority of them indicated and stressed on the adherence to social practices and hygiene practices as directed by the ministry of Health, such as social distancing, washing and keeping hands clean, putting on a mask, among others. These are some of their responses: One respondent indicated, “everything about hospital workday is about being alert. However, given COVID-19 pandemic the healthcare operations are not normal. Our medical facilities are stretching to the limits and to sustain the rising number of new infections or re-infections proves even harder. For me the healthcare is put to ultimate test of a lifetime.” Another one added: “Our hospital operations have really been put on alert and now precautions and accuracies are very strict. However, everything about medication is from the primary healthcare to avoid our bed capacity to be exceeded. We encourage everyone including the nurses and personnel to adhere to the basic standards of COVID-19 prevention.” The same resonated with a doctor who stated that “I think we are in a temporary era where the medical department has seen a shift in operations. A deadly disease is with us and one thing we as the soldiers of the healthcare department, work tirelessly to provide best medical care to our patients. It is clear that no one is 100% secure but we are encouraged to maintain precautions.”
The HCPs were likewise asked to describe how the virus pandemic has affected the health systems of the hospitals these; were some of their responses: One of the respondents indicated, “The virus at first was manageable but upon the second wave of the virus, the health care has been significantly affected. For example, we are forced to scale up the bed capacity but we have insufficient funding. As such we are forced to charge extra on the patients who come in.” Another one added that “Our doctors and nurses really work long hours to save lives and save themselves as well. They are the ones at the front line and for them to be motivated, they need extra monetary compensations.” Another one stated that “on the positive side, the virus has enlightened us towards primary health care practices of prevention rather than treatment. However, the virus is robbing the health care system of its usual capacity to take care of patients. It means continuous preparation and provision of healthcare facilities to manage the disease which at the end lead to constant money required.”
Conclusions
From the findings, the study concludes that Covid-19 has significantly affected the health system. In this regard, the healthcare facilities have received the allocated finances to help cub COVID-19 from the ministry of health. For those who did not receive the funds, it was noted that they manage COVID-19 by other means such as readjustments, operation-wise and financially, Funding from donors and charities. The study however concludes that the hospitals have insufficient number of beds, number of ventilators, number of protective gears, number of swabs and number of coronavirus test kits to help manage the COVID-19. Likewise, the study indicates that the number of beds, number of ventilators, number of protective gears, number of swabs and number of coronavirus test kits, respectively, are not accessible.
The study, therefore, concludes that the access and adequacy of existing facilities has affected Covid-19 Patients, non Covid-19 Patients, nurses and medical staff as well as the administration of hospitals to a greater extent. This concludes that the financing is still an issue to many COVID-19 patients especially those who visit private hospitals/clinics. In conclusion, the study finds that COVID-19 is one amongst the external factors that have negatively influenced the performance of healthcare systems. Amongst the external factors that affect performance, the Pestel model concludes that political, economic, social, technological, environmental and legal factors are the ones beyond the firms’ control yet very instrumental in their output (Apel, 1976). Thus, the effects of COVID-19 can be understood from the same approach of the Pestel model given its ravaging effects and the inability of individual health care systems to manage it (Schmieder-Ramirez & Mallette, 2015).
Recommendations
The study recommends the County in conjunction with the National government to scale up measures to ensure that the allocation of funds and resources necessary to combat COVID-19 are made available and accessible to all the hospitals in the country. The study recommends transparency and accountability measure by the ministry of health as well as related healthcare stakeholders on the funds allocated for the purpose of fighting COVID-19 pandemic. Likewise, the study recommends the ministry of health, the management of the hospitals and related healthcare stakeholders, to maintain the sensitization of the public on the need to ensure primary healthcare practices are adhered to. The study also recommends the development of long-term disaster plans that give clear guidelines that keep the nation healthy especially in low-income communities and on vulnerable groups. Given that the Pestel model only includes political, economic, social, technological, environmental and legal factors, the study recommends the extrapolation of the model by including such factors as pandemics like COVID-19 in order to form the basis of policy contributions and practical applications.
References
Adams, J. G., & Walls, R. M. (2020). Supporting the health care workforce during the COVID-19 global epidemic. JAMA.
Apel, H. (1976). Criticism of the Mesarovic-Pestel model and a possible alternative. In Systems Theory in the Social Sciences(pp. 374-385). Birkhäuser, Basel.
Armocida, B., Formenti, B., Ussai, S., Palestra, F., & Missoni, E. (2020). The Italian health system and the COVID-19 challenge. The Lancet Public Health.
Bai, Y., Yao, L., Wei, T., Tian, F., Jin, D. Y., Chen, L., & Wang, M. (2020). Presumed asymptomatic carrier transmission of COVID-19. Jama.
Bayham, J., & Fenichel, E. P. (2020). Impact of school closures for COVID-19 on the US health-care workforce and net mortality: a modelling study. The Lancet Public Health.
Cutler, D. (2020, April). How Will COVID-19 Affect the Health Care Economy? In JAMA Health Forum(Vol. 1, No. 4, pp. e200419-e200419). American Medical Association.
Gilbert, M., Pullano, G., Pinotti, F., Valdano, E., Poletto, C., Boëlle, P. Y., … & Gutierrez, B. (2020). Preparedness and vulnerability of African countries against importations of COVID-19: a modelling study. The Lancet, 395(10227), 871-877.
Gregory, S. (2020, April 2). The World’s Sports Stadiums Are Being Converted into Hospitals to Fight the Coronavirus Outbreak. Retrieved April 16, 2020, from https://time.com/5813442/coronavirus-stadiums-hospitals/
(2020, April 8). COVID-19: impact could cause equivalent of 195 million job losses. Retrieved April 15, 2020, from https://news.un.org/en/story/2020/04/1061322
(2020, April 13). Six Charts Show How COVID-19 Is an Unprecedented Threat to Development in Sub-Saharan Africa. Retrieved April 17, 2020, from https://www.imf.org/en/News/Articles/2020/04/13/na0413202-six-charts-show-how-covid-19-is-an-unprecedented-threat-to
Lobo, A. (2020, April 4). Ecuadorians protest bodies of COVID-19 victims being left in the streets. Retrieved April 16, 2020, from https://www.wsws.org/en/articles/2020/04/04/ecua-a04.html
Onyekwena, C. (2020, April 10). Understanding the impact of the COVID-19 outbreak on the Nigerian economy. Retrieved April 15, 2020, from https://www.brookings.edu/blog/africa-in-focus/2020/04/08/understanding-the-impact-of-the-covid-19-outbreak-on-the-nigerian-economy/
Paintsil, E. (2020). COVID-19 threatens health systems in sub-Saharan Africa: the eye of the crocodile. The Journal of Clinical Investigation.
Parpia, A. S., Ndeffo-Mbah, M. L., Wenzel, N. S., & Galvani, A. P. (2016). Effects of response to 2014–2015 Ebola outbreak on deaths from malaria, HIV/AIDS, and tuberculosis, West Africa. Emerging infectious diseases, 22(3), 433.
Qiu, W., Chu, C., Mao, A., & Wu, J. (2018). The Impacts on Health, Society, and Economy of SARS and H7N9 Outbreaks in China: A Case Comparison Study. Journal of environmental and public health, 2018.
Rosenthal, D. M., Ucci, M., Heys, M., Hayward, A., & Lakhanpaul, M. (2020). Impacts of COVID-19 on vulnerable children in temporary accommodation in the UK. The Lancet Public Health.
Sambala, E. Z., Kanyenda, T., Iwu, C. J., Iwu, C. D., Jaca, A., & Wiysonge, C. S. (2018). Pandemic influenza preparedness in the WHO African region: are we ready yet?. BMC infectious diseases, 18(1), 567.
Schmieder-Ramirez, J., & Mallette, L. (2015). Using the SPELIT analysis technique for organizational transitions. Education Applications & Developments Advances in Education and Educational Trends Series Edited by: Mafalda Carmo, 290.
Sunn, K. (2020, April 2). McKinsey offers four scenarios of Covid-19’s economic impact on Africa. Retrieved June 16, 2020, from https://www.howwemadeitinafrica.com/mckinsey-offers-four-scenarios-of-covid-19s-economic-impact-on-africa/64426/
(2020, April 15). Coronavirus Update (Live): 2,000,765 Cases and 126,776 Deaths from COVID-19 Virus Pandemic. Retrieved April 15, 2020, from https://www.worldometers.info/coronavirus.