Lara Galbarriatu1, Mónica Rivero-Garvía2, David Miranda3, Magdalena Olivares2, Enrique Jiménez-Mejías4, Edurne Ruiz de Gopegui1, Iñigo Pomposo1 and Javier Márquez2
1Neurosurgery Department, Cruces University Hospital, Bilbao, Spain
2Neurosurgery Department, Virgen del Rocío University Hospital, Seville, Spain
4Infectious Diseases Department, Virgen del Rocío University Hospital, Seville, Spain
Volume 2013 (2013),
Article ID 245718,
International Journal of Case Reports in Medicine,
5 pages,
DOI: 10.5171/2013.245718
Received date: 10 March 2013; Accepted date: 4 April 2013; Published date: 19 June 2013
Academic Editor: Andrei Borin
Cite this Article as:
Lara Galbarriatu, Mónica Rivero-Garvía, David Miranda, Magdalena Olivares, Enrique Jiménez-Mejías, Edurne Ruiz de Gopegui, Iñigo Pomposo and Javier Márquez (2013), "Postcraniotomy Brain Abscess and Empyema by Clostridium Perfringens. An Unusual Neurosurgical Complication," International Journal of Case Reports in Medicine, Vol. 2013 (2013), Article ID 245718, DOI: 10.5171/2013.245718
Background: Clostridium perfringens (C. perfringens) is the most frequently involved pathogen in gas-containing brain abscesses, most of them in the setting of penetrating traumatic brain injury. Postcraniotomy brain abscesses caused byC. perfringens are quite unusual, with very few cases reported previously in the literature. Case Description: A 17-year old male was admitted to the emergency department with signs of infection in surgical wound. He had been operated on for a recurrent craniopharyngioma two months ago. CT scan showed a gas-containing fluid collection under cranioplasty and leptomeningeal and parenchymatous enhancement. He underwent urgent surgical intervention and cultures showed C. perfringens and Proteus mirabilis growth. Broad spectrum antibiotics were administered and after 6 weeks, he was discharged home in his previous functional state. Conclusions: Clostridial brain abscess should be in the differential diagnosis of gas-containing infections after craniotomy. Surgical debridement and antibiotics are the basis of treatment, having a much better prognosis than clostridial infections outside the nervous system.
Gas-containing brain abscesses are very rare (Heineman, 1963). The majority of them are caused by Clostridium perfringens (Colen et al., 2007), (Tekkok et al., 1996) (often called “gas-gangrene of the brain” (Domingo, 1994)), usually in the setting of penetrating traumatic brain injury (60-80%) (Cohen et al., 1999), (Colen et al., 2007). Postcraniotomy brain abscesses caused by Clostridium perfringens (C. perfringens) are quite unusual (Duntze et al., 2009), with very few cases reported in the literature. We present the case of a brain abscess and empyema attributable to C. perfringens after a craniotomy for a brain tumor performed two months before.
Case Description
A 17-year-old male was admitted to the emergency department presenting fever and swelling on the previous craniotomy site. He had a history of several surgical interventions for a recurrent craniopharyngioma, the last one two months ago. The procedure consisted of subtotal tumor excision and cranioplasty; water-tight dural closure was not possible due to tissue damage and duroplasty was also performed. The post-operative period was uneventful. He suffers from panhypopituitarism and takes daily steroids.
On physical examination, he had persistent vomiting and headache, but he was able to speak and obey commands, without motor deficit (GCS 13). The craniotomy site looked reddish, tender, hot and it was painful to touch, with subgaleal gas content and pus on the wound edges. The laboratory test showed increased C-reactive protein and hyponatremia.
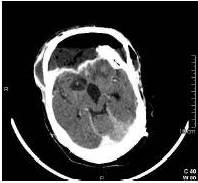
Contrast-enhanced CT scan showed gas-containing fluid collection under the cranioplasty with diffuse leptomeningeal and parenchymatous enhancement, suggesting surgical wound infection, with associated empyema and brain abscess (Fig. 1). Few hours after the diagnosis, the patient worsened, developing hypotension and oliguria, leading to shock due to the infection.
Fig 1: Contrast-Enhanced Axial CT Scan. Gas-Containing Fluid Collection under Cranioplasty with Leptomeningeal Enhancement and Brain Parenchyma Extension.
Emergency surgical intervention was performed and immediately after skin incision purulent exudate was visible. Cranioplasty was removed and a fetid collection was observed underneath, extending through subdural space and brain parenchyma. After meticulous debridement with saline with gentamicin and hydrogen peroxide, duroplasty and cranioplasty were replaced. Cultures from the abscess showed C. perfringens (susceptible to penicillin, amoxicillin, meropenem, clindamycin, metronidazole, ciprofloxacin) and Proteus mirabilis (susceptible to cephalosporins, aminoglucosydes, quinolones and carbapenems) with no fungal growth.
Broad spectrum antibiotics were administered in the post-operative period (meropenem 2gr/8h and clindamycin 600 mg/8h during 4 weeks). The patient recovered slowly and favourably, with normalization of laboratory tests and afebrile after stopping the antibiotics. At discharge, 6 weeks after the intervention, he was able to obey commands and sustain a simple conversation, without motor deficits (GOS 3).
Discussion
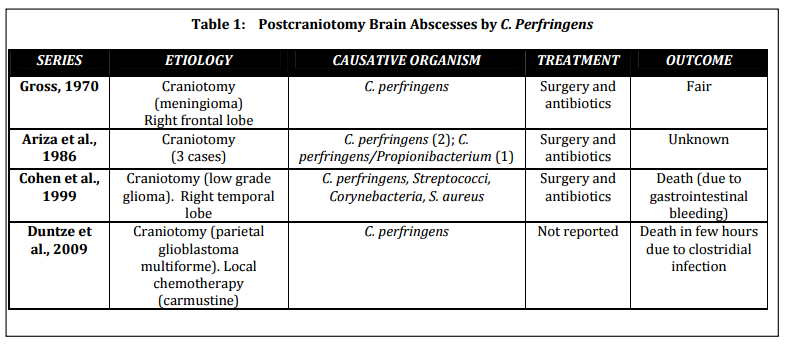
C. perfringens is a large, nonmotile, Gram-positive and spore-forming bacillus that is ubiquitous in the environment (Tekkok et al., 1996) and it is also part of the normal flora of the human bowel and genital tract (Colen et al., 2007). It is the most common cause of the gas gangrene, one of the most fulminant infections in humans, and it is detected in 60 to 90% of cases of Clostridial myonecrosis (Colen et al., 2007). It is not very common in neurosurgery (Duntze et al., 2009); nonetheless, more than 50% of the gas-containing brain abscesses are attributable to C. perfringens, with approximately 40 cases reported in the literature (Colen et al., 2007). In their review, Colen et al. found that the vast majority of them (80%) are consequence of penetrating traumatic brain injury (Cohen et al., 1999), (Colen et al., 2007), (Tekkok et al., 1996), followed by middle ear infection and cancer. Surgery is a far less common risk factor and to authors’ knowledge, there are only 6 cases of postcraniotomy brain abscesses due to C. perfringens previously reported in the literature (Table 1) (Ariza et al., 1986), (Cohen et al., 1999), (Duntze et al., 2009), (Gross, 1970).
Ariza et al. reviewed the intracranial focal infections treated in the intensive care unit and reported 5 patients with abscesses after craniotomy. Three of them were caused by C. perfringens, with the association of Propionibacterium in one case. All of them were successfully treated with surgical excision and antibiotics (Ariza et al., 1986). Gross presents the case of a brain abscess due to C. perfringens after a right frontal craniotomy for a meningioma, with good results after surgery and antibiotics (Gross, 1970). Cohen et al. report a patient who underwent a temporal lobectomy for low grade glioma excision and worsened in the immediate post-operative period. The CT scan showed a gas-containing collection in the surgical field with significant surrounding edema and cultures were positive for C. perfringens, Corynebacterium, Staphylococcus and Streptococcus. After surgical debridement and broad spectrum antibiotics the patient recovered, but he developed severe gastrointestinal bleeding and died unexpectedly (Cohen et al., 1999). Duntze et al. present a patient operated on for a glioblastoma with local carmustine chemotherapy and who developed a brain abscess due to C. perfringens three weeks later. Progression was especially fulminant, leading to patient’s death in a few hours (Duntze et al., 2009). In the present case, the patient was admitted with evidence of wound infection, two months after the last surgery. His neurological condition worsened in few hours and urgent debridement had to be performed. Multiple surgeries, impossibility of dural closure or direct contamination should be considered as predisposing factors for infection.
The optimal treatment for brain abscesses caused by C. perfringens requires a high index of clinical suspicion and early diagnosis. After a craniotomy, the radiological finding of intracranial air requires differentiating between a gas-containing abscess cavity and a postoperative pneumocephalus (Cohen et al., 1999) or other gas-like images, such as craneoplasties. Urgent surgical intervention with radical debridement and drainage is the main component of the management of clostridial cerebral abscesses (Cohen et al., 1999), (Tekkok et al., 1996), followed by intensive antibiotic therapy. Hyperbaric oxygen therapy has been reported by several authors, without clear results (Cianci, 1994), (Keogh, 1973), (Stephens, 1996).
Antibiotics without surgical intervention were used in very few cases; one of the patient reported experienced complete recovery, but had hyperbaric oxygen therapy, and the other patient died (Colen et al, 2007).
Almost half of the cases (30-50%) of clostridial brain abscesses are polimycrobial, as it is in our case. Gram-negative bacilli, including Klebsiella, E. coli and Proteus, and less often, Gram positive, such as Staphylococcus andStreptococcus, are involved in the suppurative process (Cohen et al., 1999). Fungal association should be suspected when failure of antibiotic treatment and cultures should be retained for long periods (6 weeks) to confirm the diagnosis (Tekkok et al, 1996). Despite the seriousness of clostridial wound infections outside the central nervous system, it is surprising that brain abscesses caused by these organisms are not uniformly fatal, with a global death rate attributable toC. perfringens of 10 to 11% (Cohen et al., 1999), (Colen et al., 2007).
Conclusion
C. perfringens is the most frequently involved pathogen in gas-containing brain abscesses, and it should be included in the differential diagnosis of postcraniotomy infections with such features. Urgent surgical intervention and broad spectrum antibiotics are the most efficient treatment to achieve a good functional outcome.