Victor Nwagbara1, Maurice Asuquo1, Samuel Akpan1, Dianabasi Eduwem2, Ayodele Omotoso3 and Theophilus Ugbem3
1Department of Surgery, University of Calabar, Calabar, Nigeria
2Department of Radiology, University of Calabar, Calabar, Nigeria
3Department of Pathology, University of Calabar, Calabar, Nigeria
Volume 2013 (2013),
Article ID 436550,
International Journal of Case Reports in Medicine,
6 pages,
DOI: 10.5171/2013.436550
Received date: 4 June 2013; Accepted date: 22 June 2013; Published date: 18 August 2013
Academic Editor: Rubens Chojniak
Cite this Article as:
Victor Nwagbara, Maurice Asuquo, Samuel Akpan, Dianabasi Eduwem, Ayodele Omotoso and Theophilus Ugbem (2013), " Giant Solitary Intramuscular Cystic Plexiform Neurofibroma of the Thigh: A Case Report and Literature Review," International Journal of Case Reports in Medicine, Vol. 2013 (2013), Article ID 436550, DOI: 10.5171/2013.436550
Objective: To report a rare occurrence of giant, solitary, cystic, intramuscular plexiform neurofibroma in the thigh. Case Report: A 45-year-old architect presented with a 5-year history of painless, progressively enlarging soft tissue mass in the right thigh, which was diagnosed on histology as cystic plexiform neurofibroma after excision biopsy. Conclusion: A plexiform neurofibroma should be considered in the differentials of a solitary cystic mass in the thigh even in the absence of usual manifestations of Neurofibromatosis.
According to Stedman’s Medical Dictionary, a plexiform neurofibroma (PN) is a type of neurofibroma representing an anomaly rather than a true neoplasm in which the proliferation of all elements of the nerve occur from the nerve sheath thereby resulting in an irregularly thickened, distorted tortuous structure (Stedman 2006). It is usually associated with other features of neurofibromatosis and very rarely noted as a solitary sporadic finding in those without neurofibromatosis (Cebesoy et al 2007), (Weiss and Goldburn 2002). Management of patient with PN aims at controlling symptoms and surgery is probably the only therapy in the absence medication for PN (Rallis and Ragiadacon 2009) . We present this patient with PN because of its giant size, cystic nature, in a rare intramuscular location and not associated with Neurofibromatosis-1. Case Report
A 45-year-old man presented at surgical outpatient complaining of right thigh mass of 5 years duration, which he claims, started when he fell down after a hard tackle during football practice. The mass was painless initially but increased progressively in size to involve the lower half of the back of his right thigh. There was no associated limitation of movement though he felt some discomfort and heaviness while walking. He had been in satisfactory health and reported no weight loss. There was no similar mass in any other part of his body and he had no significant past medical history nor family history. There was also no history of neurofibromatosis in any sibling.
Examination showed a healthy looking man with no visual or auditory impairment, no subcutaneous nodule, café-au-lait spots or axillary/groin freckling. He had a huge mass at the posterior aspect of lower two thirds of his right thigh (Figure 1). The mass measured about 25cm x 14cm, with poorly defined margins. It was firm (tense), non-tender and within the intramuscular compartment with normal overlying skin. The mass was non-pulsatile, with negative emptying sign. It was also warm with a small fluctuant area at the inferior limit, which yielded serous fluid on fine needle aspiration. There was no associated peripheral lymphadenopathy and no neuro-vascular deficit. His mid -thigh circumference at 18cm above knee joint line measured 65cm while the normal left thigh measured 55cm at same level. A clinical diagnosis of soft tissue tumour was made.
Investigations done showed: a normal full blood count and urinalysis. Plain radiograph of his femur showed normal bones and a huge soft tissue mass in the posterior intramuscular compartment. Chest radiograph was normal. Ultrasound scan of right thigh showed a huge soft tissue mass with a large cystic component centrally, seen in the posterior aspect of right thigh with lots of internal debris. Cyst volume was estimated at 1.6 litres. Computed tomography scan showed well-circumscribed oval shaped hypodense soft tissue mass in posterolateral compartment, (Figure 2). Aspirate cytology was negative for malignancy. Attempted incision biopsy yielded 1.8 litres of stale sero-sanguineous fluid and bled profusely afterwards prompting admission for observation with pressure bandaging. The fluid was found to have re-accumulated weeks after initial drainage but to a lesser degree.
Figure 2. CT — Circumscribed Oval Hypodense Mass
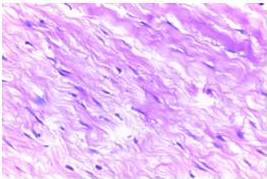
Excision was under sub-arachnoid block and specimen sent for histology. Findings include a well-circumscribed soft tissue mass with thick fibrous capsule (0.5cm thick), within the intramuscular compartment, about 10cm in diameter, containing about 500mls of serous fluid with necrotic debris, (Figure 3). Following satisfactory haemostasis, a drain was inserted and pressure dressing applied. He was discharged to surgical outpatients on second postoperative day after removing the drain. Physiotherapy and crepe bandaging was continued for one month. Histology reported as: macroscopy — cystic mass measuring 13.5 x 7.5 x 2cm with debris, cut surface was grayish, Figure 4a. Microscopy —section showed a tumour characterized by fascicles and whorls of elongated cells with wavy, serpentine nuclei and eosinophilc cytoplasm interspersed by wisps of collagen. The intervening stroma is loose, hypo cellular, and myxoid, no evidence of malignancy — plexiform neurofibroma, Figure 4b. Immunohistochemical studies were not available in our facility.
Figure 4a —Gross Photograph of Plexiform Neurofibroma after Fixation.
Figure 4b — Plexiform Neurofibroma H&E X 100
He recovered uneventfully with satisfactory wound healing with no neurovascular deficit 4 months post excision. Discussion
Plexiform neurofibroma (PN) is a benign tumour of peripheral nerves arising from a proliferation of all neural elements. It may arise from a single or multiple nerve fascicles in a major nerve trunk and usually associated with neurofibromatosis 1 (NF-1) an autosomal dominant disorder with an incidence of about 1 in 2500-3500 (Khachemoune et al 2003). The diagnosis of neurofibromatosis 1 (NF-1) is clinical and follows the criteria set out in 1987 by the National Institute of Health Consensus development conference on Neurofibromatosis (NHIS, CDC 1988), (Asuquo 2005). This includes two or more of the following:
a. 6 or more café-au-lait spots of >15mm diameter in post pubertal persons (or <5mm in prepuberty)
b. At least 2 neurofibromas of any type or 1 plexiform Neurofibroma
c. Freckling in the axilla or groin (Crowe’s sign)
d. Optic glioma
e. At least 2 lisch nodules (benign iris harmatoma)
f. A distinct bony lesion including sphenoid wing dysplasia or thinning of long bone cortex.
g. A first degree relative with NF-1
Neurofibroma is seen in about 90% of cases of Neurofibromatosis (NF-1) and is pathognomonic but these are mostly subcutaneous in location (Khachemoune et al 2003) Plexiform neurofibroma on the other hand is reported in 26.7% of NF-1 with 5-10 % risk of malignant transformation. Plexiform neurofibroma may be solitary or diffuse. It is mostly cutaneous or subcutaneous in location but can occur anywhere in the body. When massive, PN is described as an uncommon manifestation of NF-1 (Power et al 2007). It may also be asymptomatic throughout life or progress to large invasive lesion with functional disability from ‘mass effect’ and disfigurement.(Power et al 2007).The invasive type may infiltrate multiple tissue planes to affect muscle and bone making it difficult to resect.
Our index patient present with a solitary cystic intramuscular plexiform neurofibroma probably arising from a branch of the sciatic nerve without criteria for the diagnosis of neurofibromatosis and thus threw up a diagnostic challenge. Isolated giant non-cystic PN that involved the common peroneal nerve branches had been reported (Cesboy et al 2007). Cystic PN is an unusual presentation; this may be due to degeneration from the aetiological point of view.
A plain x-ray of the femur ruled out any bony involvement while a computed tomography scan clearly showed a well-circumscribed mass within the muscle compartment. This was confirmed at surgery as the mass had well defined boundaries that facilitated excision in keeping with a benign lesion. Complications include bleeding from trauma, neurological deficit, and limitation of limb function or psychological poor body image. Cystic degeneration as in our patient may occur, as may malignant change (Asuquo 2005). The presence of mitotic activity is indicative of malignancy (Roy 2000).
Surgical resection offers optimal treatment and recurrence is rare after resection except with malignant transformation (Cesboy et al 2007), (Roy 2000) but caution is important as dangerous bleeding may complicate the procedure (Happle 2001). Subtotal and total resection without functional destruction is often possible as was our experience [Onesti et al 2009), however, some may require complex intraoperative management strategies (Ross et al 2011).
It remains to be made clear whether genetic explanation exists for solitary plexiform neurofibroma (Cebesoy et al 2007), (Harper 2001) and whether it has any predilection for particular nerve like the common peroneal nerve (Koof 1999) or sciatic nerve or indeed any other.
A solitary cystic mass in the thigh evokes multiple differential diagnosis, schwanoma, haematoma, hydatid cyst, benign myxoid soft tissue tumours, and malignant soft tissue tumours with myxoid degeneration. These need to be excluded by carefully selected clinical and other investigational modality. Plain radiograph will exclude bony lesions while ultrasound scan can differentiate cystic lesions from solid tumours. The computed tomography scan assists in defining the limits and location but only appropriate tissue histopathology can made a definitive diagnosis and the best sample is an excised tissue where feasible. Though we did not have any facility, immunohistochemical approach is usually undertaken in current assessment of soft tissue tumour especially with unusual clinicopathological features as ours. Schwannomas are often associated with cystic changes compared to PN, however, on histology, the absence of a mixture of two growth patterns Antoni A, and Antoni B (Asuquo et al 2013), in Figure 4b and the characteristic features of PN confirmed the diagnosis.
Solitary plexiform neurofibroma is rare. Plexiform neurofibroma should be considered in the differentials of a solitary cystic mass in the thigh even in the absence of usual manifestations of Neurofibromatosis.
National Institute of Health Consensus Development Conference on Neurofibromatosis Statement in Diagnostic Criteria for Neurofibromatosis — 1 1987. (1988) Neurofibromatosis. (3) 172-178.
Roy, S. Neurofibroma. (2000). Arch Dermatol 36 (10) 1207-1209.
Stedman’s Medical Dictionary (2006). Plexiform Neurofibroma, 28th Edition. Lippincott, Williams and Wilkins, Baltimore, Maryland.
Weiss, S. W., Goldburn. J. R., Enzinger & Weiss. (2002). ‘Soft Tissue Tumours, Mosby-Harcourt Health Sciences Company,’ St Louis. Mo, USA, 4th Edition.