Sara Moruzzi, Domenico Girelli, Oliviero Olivieri and Simonetta Friso
University of Verona School of Medicine, Department of Medicine, Policlinico “Giambattista Rossi” Piazzale L. A. Scuro, Verona, Italy
Volume 2013 (2013),
Article ID 748811,
International Journal of Case Reports in Medicine,
7 pages,
DOI: 10.5171/2013.748811
Received date: 27 June 2013; Accepted date: 7 August 2013; Published date: 22 October 2013
Academic Editor: Wolfgang Tillinger
Cite this Article as:
Sara Moruzzi, Domenico Girelli, Oliviero Olivieri and Simonetta Friso (2013), "An Unusual Case of Acute Abdominal Pain," International Journal of Case Reports in Medicine, Vol. 2013 (2013), Article ID 748811,
DOI: 10.5171/2013.748811
Differential diagnosis for abdominal pain should enclose the rare occurrence of venous thromboembolism (VTE) which may be the clinical expression of a systemic disease including the complication or the unusual first clinical presentation of an inflammatory bowel disease (IBD) (Danese et al., 2005). Patients with IBD have an elevated risk of VTE compared with the general population (Kappleman et al., 2011, Grainge et al., 2010, and Miehsler et al., 2004). Mortality among patients with portal-mesenteric vein thrombosis is rather high (Quera et al., 2004), while, due to its rare occurrence, studies on splanchnic vein thrombosis are few and there are no univocal data on appropriate duration of oral anticoagulation therapy (Twing et al., 2005), long-term prognosis, morbidity, and mortality of the disease, which remain mostly unknown. The clinical case reported here describes a life-threatening, rare case of splenic-mesenteric-portal vein thrombosis as the acute manifestation of ulcerative colitis. Awareness and early diagnosis of splanchnic thrombosis deserve, therefore, particular attention to ameliorate the final outcome and prognosis of the disease.
Inflammatory bowel diseases (IBDs) are considered as favouring conditions for venous thromboembolism (VTE) (Danese et al., 2005, Kappleman et al., 2011, Grainge et al., 2010, Guglielmi et al., 2005, and Miehsler et al., 2004). This extraintestinal manifestation is an important cause of mortality in patients with IBD (Quera et al., 2004, Twing et al., 2005, and Hatoum et al., 2005). This rare condition, at least in noncirrhotic patients, infrequently involves uncommon sites as the splenic-mesenteric-portal vein system and may be associated with severe morbidity and mortality (Guglielmi et al., 2005). This case report points out the rare occurrence of splenic-mesenteric-portal vein system thrombosis as the first acute manifestation of ulcerative colitis in a young adult patient.
Several points define the peculiarity of the here described case: (i) the first onset sign of an ulcerative colitis by a rare occurrence, life-threatening thrombotic event in a very unusual site such as the portal-mesenteric vascular district indeed represents a challenge; (ii) the importance of an accurate multidisciplinary approach for a prompt, correct diagnosis may greatly influence the positive outcome of the disease; and (iii) the therapeutic choice and the effectiveness of an adequate duration of the anticoagulant therapy may significantly influence the disease prognosis. Given the scarce data available from the medical literature, the description of such an uncommon case with a favourable outcome may be of help in adding some knowledge for the clinical approach.
Case Report
A 32-year-old man was first referred to the emergency department (ED) of a suburban hospital because of severe, acute, and abdominal meso and epigastric pain. No signs of acute abdomen syndrome were reported, and the blood white cell count, serum amylase, and lipase levels as well as kidney and liver function markers were normal. Intravenous ketoprofen was administered with benefit, and the patient was dismissed from the hospital with the recommendation of undergoing an abdomen ultrasonography shortly.
On the subsequent day, still persisting the abdominal pain, the patient turned up to the ED of the University Hospital of Verona, where he promptly underwent an abdomen ultrasonography revealing a thrombotic portal vein obstruction.
An abdomen CT scan with contrast showed marked portal vein dilatation (3.5 cm) with characteristics of an aneurysmal-like enlargement at the site of the splenic-portal vein confluence, which appeared wholly occupied by thrombotic material (Figure 1). A thrombus of 3 cm diameter extended also to the mesenteric vein. A moderate splenomegaly was documented while pancreas and liver parenchyma appeared normal with no evidence of intra- and/or extrahepatic biliary ducts dilatation.
Figure 1. Intravenous Contrast-Enhanced Abdomen CT Scan with Contrast Showing Portal Thrombosis (Top Arrow) Associated with a Marked Portal Vein Dilatation with the Characteristic of an Aneurismal Dilatation at the Splenic-Portal Confluence that Appeared Wholly Occupied by Thrombotic Material (Left Side Arrow).
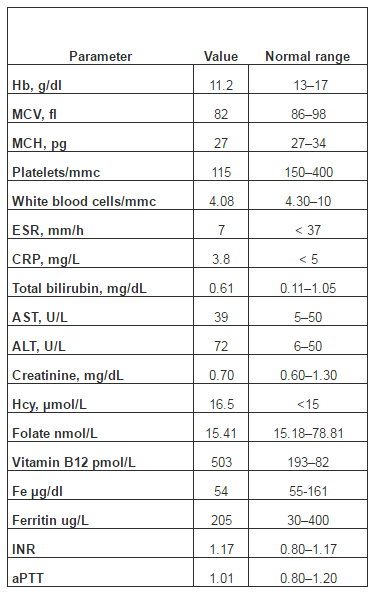
The patient was then admitted to our internal medicine department (IMD).The patient reported no significant family or personal history of venous thromboembolism (VTE). He was a smoker, but there were no other clear risk factors for VTE. Nevertheless, the patient reported that, due to persistent constipation and occasional hematochezia in the two months prior to admission, he had undergone a proctosigmoidoscopy with diagnosis of an “aspecific proctitis.” At physical examination, the epigastric and mesogastric regions were mildly painful. Peristaltic movements were normally at auscultation with negative Blumberg and Murphy signs. Cardiopulmonary examination was unremarkable. The weight was normal and the patient was afebrile. Laboratory tests (Table 1) revealed a mild microcytic hypochromic anemia (Hb 11.2 g/dL, MCV 82 fl, and MCH 27 pg) associated with hyposideremia (54 μg/dl) and normal ferritinemia (205 ng/mL). White blood cells and platelets count, inflammatory markers, electrolytes, creatinine, activated partial thromboplastin time, international normalized ratio, total and direct bilirubin, total proteins concentration, albumin, and alkaline phosphatase were normal. The neoplastic markers were also negative. Homocysteine was slightly increased (16.5 µmol/L) in association with low folatemia (6,8 nmol/L) but normal vitamin B12 plasma concentrations (503 pmol/L). Lupus anticoagulant, antiphospholipid and anticardiolipin antibodies, coagulation protein C and S, antithrombin III, activated protein C resistance, factor V Leiden, and prothrombin 20210G>A mutations were negative; the patient was heterozygous for the MTHFR677C>T polymorphism.
Table 1. Biochemical Data of the Patient at Admission in the Internal Medicine Department
Hb: hemoglobin; MCV: mean corpuscular volume; MCH: mean corpuscular hemoglobin; ESR: erythrocyte sedimentation rate; CRP: C-reactive protein; Hcy: homocysteine; AST: aspartate transaminase; ALT: alanine transaminase; Fe: serum iron concentration; INR: international normalized ratio; aPTT: activated partial thromboplastin time.
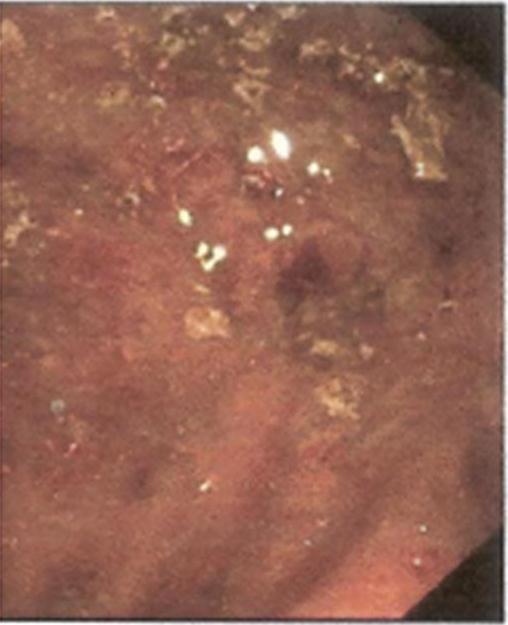
Upon arrival at IMD, intravenous sodium heparin infusion was promptly initiated (18 UI/kg/h after a bolus of 80 UI/kg). For the persistence of mild abdominal pain, a thrombolytic therapy approach was initially hypothesized. However, since the strict followup by radiologic imaging during the succeeding hours showed a progressive reduction of the mesenteric-portal thrombus extension with complete regression of the abdominal pain, this option was discarded and the patient continued intravenous heparin while oral anticoagulation was simultaneously initiated. The recent history of hematochezia associated with changes in bowel function needed further investigation, especially since a major hereditary thrombophilic state and a manifest malignant disease appeared unlikely. A colonoscopy revealed an inflamed mucosa affecting the tract from proximal transverse colon to rectum (Figure 2), suggestive for ulcerative colitis in active phase which was confirmed by histological examination of colon biopsies that showed an increase in chronic inflammatory cells in the lamina propria with basal plasmacytosis associated with marginal granulocytes deposition and scattered crypt abscesses.
Figure 2. Colonoscopy: This Picture Shows an Inflamed Mucosa, Suggestive for Ulcerative Colitis in Active Phase, Confirmed by Histological Examination.
Thus, the portomesenteric thrombosis could be attributed to a complication of inflammatory bowel disease (IBD). Therefore, oral mesalazine (1600 mg three times a day) associated with rectal-administered mesalazine (2000 mg twice daily) and folic acid was commenced.
At discharge, the patient was asymptomatic and clinically stable while continuing the IBD therapy associated with warfarin. The patient was subsequently followed up in the outpatient clinic.
Forty-five days after discharge, the patient underwent contrast-enhanced magnetic resonance that showed resolution of the portomesenteric thrombosis, while the aneurysmal dilatation at the splenic-portal confluence was still detectable. About a year after the diagnosis, an abdominal ultrasonography confirmed a splenic-portal vein axis free from thrombotic material and the colonoscopy documented a quiescent state of IBD so that oral anticoagulant therapy could be discontinued.
Discussion
VTE infrequently involves uncommon sites as the splenic-mesenteric-portal vein system. Early diagnosis is often difficult because VTE can develop in asymptomatic patients (Maconi et al., 2012), and the most recurrent symptom, that is, moderate-to-severe abdominal pain in the upper quadrants, is largely aspecific, as it occurred to our patient.
In the present case, the abdominal pain was likely due to VTE and not to IBD considering that the white blood cell count and the inflammatory markers were within the normal values and that other signs or symptoms as rectal bleeding or diarrhea were absent. This infrequent condition of a VTE in such site may be associated with severe morbidity and mortality (Hatoum et al., 2005, Martinelli et al., 2008), but the recent literature shows conflicting data (Maconi et al., 2012).
The peculiarity of the present case refers to the onset of an ulcerative colitis at inactive stage by a rare occurrence, life-threatening thrombotic event in a very unusual site such as the portal-mesenteric vascular district that indeed represents a clinical challenge. Furthermore, the appropriate treatment and the duration of anticoagulant therapy are not consistently reported in the literature, so far, and the description of the effectiveness of the therapeutic approach in specific cases, considering the rare occurrence of the disease, may be greatly helpful for the clinician.
At the first access to the ED, the patient was probably not adequately treated considering that the abdominal pain was acute and severe, and in such event, instrumental investigations (e.g., plain abdominal X-ray or ultrasonography) should have been performed as soon as possible. Moreover, in the differential diagnostic approach of epi-mesogastric pain in which the suspicion of peptic disease had to be considered, the administration of ketoprofen was to be avoided.
Imaging techniques (Doppler ultrasonography, CT-scan, and MRI) greatly contribute to early diagnosis (Hatoum et al., 2005, Martinelli et al., 2008). Reports on possible association with thrombophilic abnormalities are scarce (Martinelli et al., 2008). In addition to classical primary or acquired thrombophilic conditions including the JAK-2 V617F mutation, liver cirrhosis, surgical injury to the portal venous system, gastrointestinal cancer, and IBD are listed among favouring conditions for the occurrence of splanchnic vein thrombosis (Martinelli et al., 2008). IBD is a condition associated with a potential hypercoagulability state and with an incidence of thromboembolic events higher than in the general population (Kappleman et al., 2011, Grainge et al., 2010, and Miehsler et al., 2004). The relationship between inflammatory bowel disease and platelet functions is well known, and the platelet aggregation response could be increased even in inactive phase patients (Andoh et al., 2006).
Regarding IBD, Talbot et al. (1986) observed that VTE occurred in 1.3% of the patients during an 11-year follow-up study (Talbot et al., 1986). Mesenteric and portal vein thromboses were mainly postsurgery complications, while 77% of peripheral venous thrombosis occurred spontaneously (Talbot et al., 1986). In most cases (73%), the disease was in active phase as demonstrated by the finding of increased inflammatory markers (Talbot et al., 1986). On the other hand, it has been observed that mesenteric thrombosis may develop even during clinical remission with a mean time of 24.6±13.5 years since IBD diagnosis (Quera et al., 2004, Jackson et al., 2011). A laboratory marker with sufficient predictability to identify patients at particular risk of VTE has not been identified, thus far (Quera et al., 2004). Mortality among patients with portal-mesenteric vein thrombosis is rather high, ranging from 25% to 50% (Guglielmi et al., 2005, Talbot et al., 1986) according to different clinical settings.
Because of its rare occurrence, studies on splanchnic vein thrombosis are few and there are no randomized trials of adequate size to provide convincing data on appropriate duration of oral anticoagulation therapy, long-term prognosis, morbidity, and mortality, which remain mostly unknown. Treatments with catheter-directed or systemic thrombolysis have been proposed in severe cases, but results are contradictory in terms of efficacy and safety. Anticoagulation with vitamin K antagonists is associated with recanalization in 45% of the cases and protects from recurrence. Lifelong anticoagulation is therefore recommended for splanchnic vein thrombosis where the vein is not recanalized and for those patients with inherited thrombophilia such as prothrombin or factor V Leiden mutation carriership (Amitrano et al., 2007).
The issue of an appropriate anticoagulant therapy use in splanchnic vein thrombosis is even more complex than for other rare venous thrombosis for several reasons. Portal vein thrombosis often leads to severe sequelae such as portal hypertension, which in turn increases the risk of bleeding because of both esophageal varices and hypersplenism-related thrombocytopenia (Martinelli et al., 2008). Indeed, the decision on the duration of oral anticoagulation should be individually tailored (Kappleman et al., 2011, Twing et al., 2005) according to the risk/benefit ratio due to presence or absence of major risk factors for bleeding or recurrent thrombosis (De Stefano et al., 2010). If the bleeding risk is low or absent, anticoagulant therapy should be continued until vessel recanalization is documented. In the presence of esophageal varices, an endoscopic bending and medical therapy with beta-blockers is suggested, while in the presence of thrombocytopenia, oral anticoagulation is to be avoided if platelet count is below 50,000/mmc (Martinelli et al., 2008). Considering the prolonged remission of IBD, as it refers to the here described case, oral anticoagulation was discontinued when portal-mesenteric vein axis was completely recanalized. At five-year followup, the patient is asymptomatic, with a regular bowel function, in remission phase of ulcerative colitis disease. Abdominal ultrasonography shows no evidence of thrombi in the portal and mesenteric venous axis.
De Stefano, V. & Martinelli, I. (2010). ‘Safety of Anticoagulant Treatment in Patients with Non-Malignant Non-Cirrhotic Extrahepatic Portal Vein Obstruction,’ Internal and Emergency Medicine, 5:487-94