Kango Gopal, Gopinath1, Paul Wilson, Benny2, Sathyendra, Sowmya3, Viggeswarpu, Surekha2, Iyyadurai, Ramya3, Ramachandran, Krishnappriya4 and Prasad Mathews Kuruvilla2
1Aged and extended care services The Queen Elizabeth Hospital Woodville West South Australia
2Geriatrics, Christian Medical College, Vellore, India
3Internal Medicine unit 3, Christian Medical College, Vellore, India
4Respiratory Medicine, Christian Medical College, Vellore, India
Volume 2013 (2013),
Article ID 915700,
International Journal of Case Reports in Medicine,
3 pages,
DOI: 10.5171/2013.915700
Received date: 21 March 2013; Accepted date: 29 April 2013; Published date: 28 May 2013
Academic Editor: Khurshid Iqbal Andrabi
Cite this Article as:
Kango Gopal, Gopinath, Paul Wilson, Benny, Sathyendra, Sowmya, Viggeswarpu, Surekha, Iyyadurai, Ramya, Ramachandran, Krishnappriya and Prasad Mathews Kuruvilla (2013), "Carcinoma of Theesophagus Presenting Asstridor to a Tertiary Care Hospital in South India," International Journal of Case Reports in Medicine,
Vol. 2013 (2013), Article ID 915700, DOI: 10.5171/2013.915700
Esophageal carcinomais an aggressive malignancy and usually manifests with dysphagia and weight loss. We are presenting case details of a patient with esophageal carcinoma who presented to the emergency services with acute onset stridor and breathing difficulty. Computerised Tomography of the chest showed a large esophageal lesion invading the trachea. Stridor as a primary presentation of this tumor has not been frequently reported. This case demonstrates the need to consider esophageal carcinoma in any patient presenting with stridor.
Esophageal carcinomais a relatively common malignancy and is considered to be the third most common tumor in certain districts of rural south India (Swaminathan et al. 2009). Esophageal carcinomais more common in males as compared to females (Sharma et al. 2009). Esophageal cancer is one of the most aggressive malignancies of the digestive tract, with high morbidity and mortality (Pereyra & Velarde 2009).Hence early diagnosis is of paramount importance in these patients. The most common symptom of esophageal carcinomais dysphagia. Stridor as a manifestation of esophageal carcinoma is extremely rare and has been reported by strauss et al in 1996 (Strauss et al. 1996). We are presenting a case of esophageal carcinoma of the middle third who presented to our hospital with stridor without preceding history of dysphagia.
Case Details
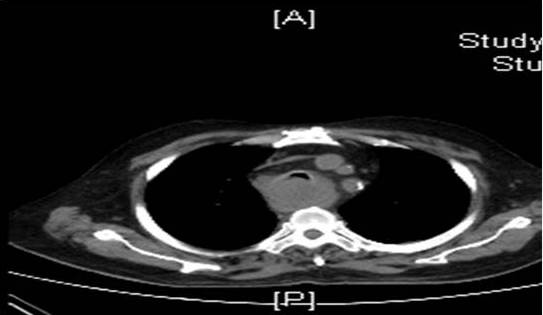
A 76 year old farmer was brought to Accident and Emergency department wing (A&E) of our hospital with history of sudden onset of cough, breathing difficulty associated with a high pitched noise arising from the upper chest. There was no history of fever, loss of consciousness, seizures, trauma or dysphagia prior to presentation. He was a known case of Chronic Obstructive Pulmonary Disease (COPD) and was on regular inhalers and bronchodilators. He had a significant history of smoking with 30 pack years. He gave a history of 15 kg weight loss in the past 4 months. On examination, he was cyanosed, pulse was 100/ min, blood pressure was 100/70 mm Hg and respiratory rate was 38/ min. Examination of the respiratory system revealed a stridor, bilateral wheeze and crepitations along with other features of COPD including barrel shaped chest and wide sub costal angle. A provisional diagnosis of acute exacerbation of COPD and stridor was made and was commenced on usual treatments for an acute exacerbation without considerable symptom resolution. Chest X ray revealed mild widening of the superior mediastinum with hyperinflated lung fields. An urgent Computerised Tomography imaging of the chest was done that showed a large tumor arising from the esophagus obliterating its lumen infiltrating and encasing the trachea, with significant luminal narrowing associated with extension into both the right and left main bronchi with significant carinal narrowing (Figure 1). Biopsy of the lesion showed moderately differentiated squamous cell carcinoma of the esophagus. The patient was treated with bronchodilators and dexamethasone to reduce tracheal edema. Tracheostomy was not feasible considering the level of the lesion. The patient was offered emergent tracheobronchial stenting in consultation with the radiologists. He was also offered percutaneous endoscopic gastostomy (PEG) as a palliative procedure for feeding. However, the patient discharged himself against medical advice from our hospital.
Figure1. Showing the Esophageal Lesion Invading the Trachea
Discussion
We have presented this patient to highlight the importance of considering carcinoma esophagus in patients presenting with stridor. To the best of our knowledge, there are no reported cases of carcinoma esophagus without preceding dysphagia presenting as acute stridor and clinicians need to be aware of this possibility. Mechanisms of stridor in esophageal carcinoma include direct invasion of the trachea and involvement of the vocal cords by the tumor. Stridor has been reported secondary to esophageal stent placement in patients with esophageal carcinoma due to expansion of the stent after placement compromising the tracheal lumen. Infact, in these situations, double stent placement in both the trachea and esophagus is recommended (Nicholson 1998).
Our patient had direct tracheal invasion by the esophageal tumor that was suspected on a computerized tomography imaging of the chest and confirmed on bronchoscopy. Moreover, it is interesting to note that the patient did not complain of dysphagia though the esophageal lumen was almost fully obliterated. Prognosis is considered to be dismal in patients with respiratory tract invasion.
Conclusion
Stridor is a medical emergency that warrants prompt action to establish the etiology and initiate treatment. Esophageal carcinoma should be considered in these patients particularly when common airway causes have been excluded.