Florian Lüders, Alfred Doku, Nasser Malyar and Holger Reinecke
Department of Cardiology and Angiology, University Hospital of Muenster, Muenster, Germany
Volume 2014 (2014),
Article ID 232740,
International Journal of Case Reports in Medicine,
7 pages,
DOI: 10.5171/2014.232740
Received date: 4 April 2014; Accepted date: 12 May 2014; Published date: 31 May 2014
Academic Editor: Kenei Shimada
Cite this Article as:
Florian Lüders, Alfred Doku, Nasser Malyar and Holger Reinecke (2014), "Endovascular Management of a Periinterventional Crural Pseudoaneurysm — A Case Report and Review of Literature," International Journal of Case Reports in Medicine, Vol. 2014 (2014), Article ID 232740, DOI: 10.5171/2014.232740
Iatrogenic pseudoaneurysms of the anterior tibial artery are infrequent; the optimal treatment strategy is still a subject of debate. We report a case of an anterior tibial artery pseudoaneurysm complicating an endovascular intervention which was managed by transluminal platinum coil embolization and review the current literature. Three platinum coils were placed in the anterior tibial artery endovascularly resulting in the successful embolization and occlusion of the pseudoaneurysm. Endovascular therapy offers an effective and a safe strategy in managing infrapopliteal pseudoaneurysms.
Rising awareness and recognition of the burden of obstructive peripheral arterial disease (PAD) in the health care system has also seen a parallel marked increase in utilization of lower extremity endovascular revascularization procedures [1]. Revascularization of infrapopliteal lesions by means of endovascular approach is evolving to be the standard of care, as it provides in general an excellent clinical outcome with low morbidity and at low procedural costs [2]. However, experiences with the management of the complications following PTA, such as iatrogenic infrapopliteal pseudoaneurysm, are sparse and varied.
Infrapopliteal aneurysms, compared to femoral aneurysms, are rare, and consist mainly of pseudoaneurysms. The pathogenesis of a pseudoaneurysm is characterized by a disruption of the arterial wall with extravasation of blood into the surrounding tissue. This leads to the development of a fibrous sac, which gradually increases in size due to the arterial pressure.
Infrapopliteal pseudoaneurysms could develop from penetrating or blunt injury [3,4], bimalleolar fracture or fracture of the ankle [5], infectious processes of the arteries [6] or connective tissue disorders such as Behcet’s disease [7] or as a complication of endovascular procedures, like Fogarty-balloon thromboembolectomy [8], and rarely as a complication of PTA [9,10].
It is expected that with the increase in the number of infrapopliteal endovascular revascularization procedures, the number of procedural related complications will also increase. Such complications frequently necessitate an endovascular therapeutic management [8] since a surgical approach in such patients with comorbidities is associated with an increased morbidity and delayed wound healing.
Here we report a successful endovascular management of an infrapopliteal pseudoaneurysm in a patient with severe claudication (Rutherford category 3) who underwent PTA because of high-degree stenosis of the anterior tibial artery, and review the existing literature.
Case Report
The patient is a 72-year-old woman with a history of dyslipoproteinemia, arterial hypertension and type II diabetes mellitus. She complained of claudication in the right foot and calf after walking a distance of 20 meters. Duplex ultrasonography showed moderate stenosis of the right popliteal artery, total occlusion of the proximal right ATA and right tibiofibular tract.
Because of clinically distinct pulmonary arterial hypertension associated with CREST syndrome, coronary 3-vessel artery disease, impaired right ventricular systolic function with severe tricuspid regurgitation and her refusal of a surgical treatment, an endovascular approach for revascularization was chosen. Because of the planned PTA, 300 mg loading dose of Clopidogrel was given in addition to her regular platelet inhibition with Aspirin (acetylsalicylic acid). The pre-procedural angiographical image confirmed the findings of the previous Duplex ultrasonography of distal popliteal artery and lower leg arteries (Figure 1). After successful PTA and stenting of the distal popliteal artery and the right tibiofibular tract, PTA of ATA was performed with a 2.5 mm diameter Pacific balloon with an inflation pressure of 8 bar (nominal pressure) over 2 minutes. Immediately after the PTA an extravasation of contrast agent into the surrounding tissue of mid ATA was visible (Figure 2). Six prolonged PTAs with a Pacific balloon (average 7.5 minutes each) with adjuvant administration of 1000 IE protamine stopped the extravasation of contrast medium. The next day, an ultrasound examination revealed a 36 x 23.
Figure 1:Pre-procedural Angiographical Image of Distal Popliteal Artery and Lower Leg Arteries
Figure 2: Postinterventional Extravasation of Contrast Agent into the Surrounding Tissue of Mid ATA, as an Expression of a Pseudoaneurysm
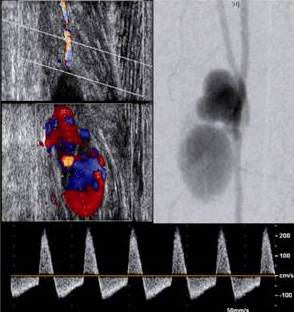
x 21 mm pulsatile pseudoaneurysm with oscillating flow in the ATA (Figure 3). Because of the high operative risk, an endovascular approach using coil embolization was preferred.
Figure 3: Ultrasound Examination Revealed a 36 X 23 X 21 Mm Pulsatile Pseudoaneurysm with Oscillating Flow in the ATA
Using the right common femoral artery access in antegrade puncture technique, a 110 mm-long, 4-Fr sheath was percutaneously advanced into the vessel. Angiography showed a good short-term result of the interventions at the popliteal artery and of tibiofibular tract. Digital subtraction angiography confirmed a 5.1 × 2.4 cm three-chambered, pulsatile pseudoaneurysm at the middle third of the right ATA. There was no flow in the ATA distal to thepseudoaneurysm. Branches of the fibular artery showed a good blood supply of the foot.
Three microcoils (Boston interlocking coils) were inserted into the ATA just proximal to the PSA via a micro-catheter (Figure 4). The immediate angiographic control (Figure 4) and duplexsonographic control the next day confirmed a complete occlusion of the pseudoaneurysm with occlusive signal in the ATA. In view of the successful PTA and stenting of the distal popliteal artery and the right tibiofibular tract, the postcoiling ABI value measured in the right ATP (0.75) was slightly improved compared to the pre-interventional value (0.57); the postcoiling ABI value in the right dorsalis pedis artery (0.43) was similar to the pre-interventional value (0.44).
Figure 4: Three Microcoils were Inserted in the ATA Just Proximal to the PSA via a Micro-Catheter. The Immediate Angiographic Control Confirmed a Complete Occlusion of the Pseudoaneurysm
The patient improved clinically, and was discharged from hospital 2 days after the coil embolization. Discussion
Increasing prevalence of atherosclerotic risk factors, particularly diabetes, with an ageing population has resulted in a dramatic increase prevalence of PAD involving more distal, small-sized arteries. These patients frequently have severe comorbidities with a high perioperative risk precluding them from a surgical approach. On the basis of this, the number of endovascular revascularization of the distal parts of lower limb vasculature is increasing worldwide [2]. Despite accumulating experiences with endovascular interventions in the distal arterial bed, increasing the number of such interventions is expected to result also in increasing the number of periprocedural complications such as formation of an intervention-related PSA [10].
The clinical feature of such PSAs is variable. The spectrum ranges from clinically inapparent pseudoaneurysms to the complete scenario of a compartment syndrome necessitating immediate surgical intervention.
There are no evidence-based recommendations or guidelines as to how such complications should be treated. The management of such PSAs depends also on the clinical scenario. In cases of a small (<2 cm) asymptomatic PSA without a tendency to enlargement, a conservative approach is justified, as such PSA can occlude spontaneously by thrombosis within the lumen of PSA [11]. While PSA of the common femoral or popliteal arteries can often be treated successfully with ultrasound-guided compression, PSA of the infrapopliteal arteries, particularly arising from the ATA is difficult or almost impossible to compress. The surgical management involves the cut off of blood flow to the PSA, either by proximal and distal ligation, or by primary closure of the inflow or by rerouting the blood flow around this damaged segment of the artery. The bypass could be achieved either by using an autologous vein of the patient or by using a synthetic graft [12]. It must be emphasized that surgical approach in small-sized infrapopliteal arteries are associated with a high rate of re-occlusion and abnormal wound healing.
Ultrasound-guided thrombin injection [13] has also been described as an alternative therapeutic option for PSA.Endovascular options include the insertion of a plain or covered stent [14], and the occlusion of the PSA by means of repeated balloon inflation proximal to the PSA neck [15]. Endovascular coil embolization as described in this case might be another option, when the aforementioned are either not possible or not successful. In our patient, repeated inflation of the Pacific balloon did not lead to an occlusion of the PSA.
Looking in the current literature, we found only few cases of endovascular interventions of infrapopliteal PSA [16, 17, 18]. In our case endovascular coil embolization was appropriate because the peroneal artery was the dominant arterial supply to the foot, and therefore the right ATA could be occluded proximal to the PSA neck. The postprocedural obtained peripheral pressures and the ameliorated clinical status of the patient confirmed that the occlusion of the ATA did not result in an aggravation of the right foot ischemia.
Abbreviation
ATA – anterior tibial artery
PAD – peripheral artery disease
PSA – pseudoaneurysm
PTA – percutaneous transluminal angioplasty
Competing Interests
The author(s) declare that they have no competing interests.