RISEBA University of Applied Sciences, Riga, Latvia
Volume 2022,
Article ID 242208,
Journal of e-health Management,
14 pages,
DOI: 10.5171/2022.242208
Received date: 24 March 2022; Accepted date: 11 November 2022; Published date: 21 December 2022
Academic Editor: Carmen-Eugenia Costea
Cite this Article as:
Kirathimo Muruga (2022)," Perception of Health Care Practitioners on Dual Practice in Kenya", Journal of e-health Management, Vol. 2022 (2022), Article ID 242208, DOI:10.5171/2022.242208
Purpose: The purpose of this study was to establish the perception of health care practitioners on dual practice in Kenya. Methodology: The current study adopted the descriptive method of study. The study targeted all health care practitioners from the Kenya Medical Practitioners and Dentists Council (KMPDC) doctors’ retention register. The selection was scientifically guided using Fishers’ formula (Fisher, 1956; Fisher, 1962). Data collected were primary and qualitative in nature. The data were collected using semi-structured interview guide. The collection involved issuing out the interviews via e-mails to the respondents and consistent follow-ups made. Qualitative data collected from the field were analyzed using content analysis which involved identification of recurring themes, patterns, or concepts and then describing and interpreting those categories. The analysis was aided by the use of Excel 2016. Furthermore, the coded data were presented by use of themes, frequencies, percentages, averages, or standard deviations, among others. Results: The findings revealed that dual practice among Kenyan health care providers is prevalent. Many of the healthcare providers fear losing their public health jobs. As such they carry out dual practice secretly without their public health employers’ knowledge. It has likewise been concluded that holding private jobs alongside public jobs in the health sector is influenced by various internal factors such as organizational resources, Income Public healthcare effectiveness and working environment. However, the extent of the influence is strong with respect to organizational resources’ effectiveness of public healthcare and working environment. Income being among the factors has been regarded as a weak influencer compared to the organizational factors. The study therefore concludes that most of Kenyan health care providers engage in dual practice due to the unwelcoming working environment and ineffective public health care facilities. It has also been noted that there is no legally binding contractual framework that optimizes the physician’s dual practice. The study thus concludes that the Kenyan legal framework is weak and thus the physicians have little faith in the existing framework since it is not legally binding. Unique contribution to theory, practice, and policy: The study recommends the policy makers to design legally binding contractual agreement within the policies that enable the health care practitioners engage in dual practice. This involves re-evaluation and re-shaping of the existing policy in the area of managing contracts for physicians in dual practice. Currently it has been noted that the existing policy is weak, not standard and not uniform, since the application is left to the individual hospitals. Given that the study found the health care providers are more concerned with internal organizational factors such as working environment as opposed to income, the study recommends the ministry of health to improve the working environment of the public health care facilities. In addition, the MoH is recommended to ensure that the public health care facilities are in good working condition.
Keywords: Perception, health care practitioners, dual practice
Introduction
Multiple job holding is a common trend of public servants employed concurrently from within the public sector framework. Part time work may be performed either inside or outside public buildings, but is carried out either solely for personal advantage or as part of a benefit-sharing agreement with the relevant government jurisdiction. Dual practice (DP) is growing within but not limited to healthcare practitioners (Hipgrave & Hort, 2014). Teachers may subsequently provide private schooling such as tuition while researchers may consult privately. Public security personnel and, conceivably, any qualified professional or other public service provider may perform private work in addition to private work additional to their government contract. However, DP in the health sector attracts the most interest because it concerns an issue of universal importance that can be extremely costly, is inherently unpredictable, and assumes the availability of skilled care (Bloom et al. 2008).
Such dual practice (DP) is present in both high-and low-and middle-income economies across the globe, with different levels/extents of accommodation. Healthcare professionals engaged in multiple health-related activities are, among other things, one form of trend that has more consequences for different kinds of service provision and has been a factor by several researchers (Moghri et al., 2016). Garcia-Prado and Gonzalez have defined various types of dual practice based on two variables: the essence of the two workers (public versus private) and the contractual agreement in effect (García-Prado & Gonzalez, 2007).
Dual practice is used widely in health care systems in numerous European and Asian countries and exerts a direct or indirect impact on health labor supply, health care quality, waiting time, and health service expenditure. In addition, WHO reports that Dual practice is very common among certain categories of specialized nurses and doctors. In the United Kingdom of Great Britain and Northern Ireland, over 60% of public hospital doctors conduct private practice alongside their National Health Service work; in Spain, 20% of public sector doctors have a second job and about 25% of public hospital doctors in Norway reported holding a private sector job (McPake et al., 2016). In the regions of Angola, Cambodia, Indonesia, Peru, Syria, and Vietnam, most doctors have dual practice in the public and private sectors. And both urban physicians and rural physicians join dual practice in Egypt and South Africa (Ferrinho et al., 2004).
While in low-income nations it is often stated as a coping strategy to cover for low salaries in the government sector, in well developed countries physicians prefer to perceive DP as an opportunity to gain clinical autonomy and fulfill professional ambitions/mileage (Ferrinho et al., 2004; Humphrey & Russell, 2004). In addition, DP may be driven by the potential to provide more interaction with patients in the private sector, to treat fewer patients with more resources and time, to have facilities that are not accessible in the public sector, and to obtain more ultimate experience in relation to exclusive public practice (Jumpa et al., 2007; Alaref et al., 2017).
However, Dual practice (DP) is most likely to have negative consequences in lower- and middle-income countries, where regulation of doctors’ behaviour is often weak. Weak regulation of DP threatens equitable, universal access to healthcare (Hipgrave & Hort, 2014). Health officials in both the advanced and developing countries are becoming receptive to the adoption of a DP policy to improve quality healthcare and provide a wider scope for more patients’ access to high-quality health resources to minimize the scarcity and unwarranted allocation of health resources and address issues of inadequate outcome, low efficiency and lassitude for physicians in public health institutions. It can cause a change in human health services, leading to disparities between urban and rural areas, public and private health agencies, and hospitals and community health agencies (Chen et al., 2016). Policymakers and healthcare agencies typically use a dual practice strategy (for instance, to prescribe the number of working hours for medical personnel in public hospitals and to maintain the maximum salary levels for doctors in private hospitals and to administer periodic quality assessments) as a method to account for the low income of medical staff and reduce health costs. Some researchers have argued that dual practice is a government action that requires healthcare providers’ personnel to work to ensure the wellbeing of patients and private health facilities (Biglaiser & Albert, 2007; (García-Prado & González, 2011; Deng & Zhang, 2016).
On a personal level, however, Ferrinho et al. (2004) have ascertained that dual practice contributes to brain drain, specifically public-to-private brain drain. The standard of their work is constrained by the fact that public sector health workers are holding multiple jobs in private practice. Furthermore, in most instances, the use of public transport, office facilities and staff sources reflect significant secret cash flows, often in due to dual practice. As such, DP can lead to unethical actions on the part of health workers. In certain cases, this forms a de facto financial obstacle to access health care. It de-legitimizes the provision of health care services in the public sector and jeopardizes the required relationship of trust between patient and provider. Clinicians in dual practice have to compete for patients with themselves, which is an incentive to lower the quality of the care they provide in the public services (Hipgrave & Hort, 2014).
Therefore, depending on how Dual practice is defined, an individual’s limit to perform two or more jobs/tasks at the same time has some implications either on the primary job or the part-time job. These implications can either be negative as well as positive. However, the extent to which the outcomes steer the public provision of healthcare service varies with the motivation behind it as well as the regulations underlying the industry. These, according to the Herzberg’s Two-Factor Theory, are referred to as the presence of motivators (intrinsic factors) or the absence of hygiene factors (extrinsic factors). Therefore, based on the premise of profit maximization for patients and health-related social cost minimization and given the developing economy of Kenya, it is imperative for a deeper look into the perceptions of the health care providers (HCPs) on the engagement in dual practice. Contextualizing the study to Kenya provides a deeper understanding of the best way to meet the needs of the HCPs in public hospitals for better service provision. The current study, therefore, took that approach in bid to find out the perceptions of the healthcare providers in Kenya public hospital and the engagement in dual practice.
Statement of the Problem
Physician multiple job holding is common and generally perceived to have significant consequences for the labor supply of doctors, the rate of production of health care and the quality of health care services (García-Prado & González, 2011). Specific attention is paid to the impact of multiple job holding on the public delivery of health care. The fact that a particular practitioner delivers health services to both the public and private sectors is the primary source of contention in the policy debate, where the presence of concurrent medical practice is in conflicts with the ideal labor market structures for the employer-employee partnership. As a result, there is a strong focus on the need for policy measures for dual medical practice (WHO, 2000). Economic literature on the topic of multiple job holding and its impact on the public health sector is relatively young and not voluminous. The general inference from the literature tends to be that multiple job holding has both positive and negative effects on the delivery of public health services and that the net impact is difficult to assess (Alaref et al., 2017).
A variety of adverse effects of dual practice have been noted, including absenteeism (Pouliakas, 2017) and shirking during official working hours, patients being forced into the private sector by dual practitioners preferring private work, manipulating the standard of healthcare or increasing waiting time in order to promote private care, leaving the poor people with limited access to health treatment, limited access to services in rural areas, as dual practitioners are allowed to live in urban areas, free-riding or theft of supplies from public hospitals or use of public administration or nursing staff or hospitals for private patients, treat private patients in public areas and have worse public-sector treatment to promote patients to go private (Garcia-Prado & Gonzalez, 2011; Caruso, 2014).
In the last decade in Kenya, between December 2011 and September 2012, there has been two major longest Nationwide Doctors’ strike with devastating lives and economic losses (Muhudhia, 2017). Between January 2015 and March 2017, many patients died or suffered from disability because they could not access care (Masika, 2017; Waithaka et al., 2020). During the same period, many patients were forced to seek health care services from private hospitals, incurring catastrophic financial liability. There is a lack of quality evaluative evidence regarding the consequences of dual practice on the delivery of services of healthcare and management organizations (Muhudhia, 2017; Ongori, 2019). The overall impact of dual practice remains an open question that warrants more attention from researchers and policy makers alike (García-Prado & González, 2011). Therefore, based on the above backdrops, the current study sought to investigate what factors exactly influence the physicians into taking private jobs. This was done to investigate the perceptions of health care practitioners on dual practice in Kenya.
Literature Review
In response to the opportunities they face, Berman and Cuizon (2004) indicated that healthcare providers engage in multiple job holding for a variety of reasons. Increasing income has been noted to have the probability to the main reason, however, institutional, and professional considerations as well come into play. And even the assumptions regarding growing wealth do not provide strong conclusions that this will necessarily lead to violence or denial of treatment to the vulnerable. Public providers keeping alternative private sector jobs may view these jobs as being comparable with, or complementary to, their private industry or some of them. According to Ferrinho, Van Lerberghe, Fronteira, Hipólito & Biscaia, (2004), the reasons for dual practice are contextual. Health staff are now dependent on individual coping mechanisms to compensate for insanely low wages. In many developing countries, this often leads to frequent doctors’ unrest and strikes. Many physicians combine paying public-sector clinical jobs with a fee-for-service personal clientele. This dual activity is also a method through which HCPs seek to meet their livelihood needs, reflecting the failure of health ministries to guarantee sufficient wages and conditions of employment. On the other hand, dual practice enables practitioners to have a standard of living that is similar to what they expect, as well as a standard of practice that is similar to their own standards of good professional practice, resulting in higher professional satisfaction.
Chen (2016) examined the factors that affect the understanding of dual practice by medical workers and outpatients in Shanghai, People’s Republic of China. In addition, medical staff who were affiliated to the Surgical Department or assumed that dual practice would minimize the burden of visiting a doctor indicated a more likelihood to engage in dual practice. In addition, the presence of promotional events and a more versatile clinical human resource management program was found to likely increase the ability of doctors to enter dual practice. The doctors perceived dual-practice outpatients to be influenced by their professionalism, age, monthly salary, self-rated health status, and the burden of health spending. Therefore, while devising DP policies, policymakers and associated health care agencies need to factor in the demographic characteristics of medical staff and outpatients just as much as the professional characteristics are and take reasonable steps to improve the ability of medical staff to engage in dual practice. Moghri et al. (2017)indicated that DP is a versatile phenomenon and has dissimilar implications in different contexts and settings and there is not a single recipe for it. Understanding the nature, prevalence, reasons, and the implication of DP is the first step toward designing appropriate policies and interventions for the management of this phenomenon.
In Iran, Bayat et al. (2018) sought to investigate the extent and nature of dual practice engagement among medical specialists. From the study, 11638 that is 47.7% of the specialists were engaged in DP on total. Female specialists had 0.78 times less DP chance; faculties compared to non-faculties had 0.65 times more DP chance and full-time geographic specialists compared to non-full-time specialists had 0.15 times more DP chance. The level of DP is relatively high among Iran medical specialists, especially in geographic full-time specialists. However, they are totally banned, and they receive extra payment for being full-time; restrictive regulations and financial incentives without considering other factors might not eliminate DP in specialists and it should be addressed based on conditions of each country and regions inside the country. With the objective to conduct a review on nurses’ dual practice, Russo, Fronteira, Jesus & Buchan (2018) conducted a qualitative study by reviewing nurses holding multiple jobs. While holding multiple jobs was not always a leading factor to dual activity, a variety of ways were discovered for public-sector workers to participate concurrently in public and private jobs, both in regulated and informal casual fashions. Some of these types have been reported to be especially prevalent, from more than 50 per cent in Australia, Canada, and the United Kingdom, to 28 per cent in South Africa. The ability to raise the modest wage, but also the discontent with the main job and the flexibility provided by a variety of work-holding arrangements, were among the reasons given for these activities. Flexibility of additional part-time employment seems to be another key factor for Australian and UK nurses, since nursing is a typically female profession, and some female workers have a strong preference for part-time flexible jobs, in comparison to their male peers.
Eze (2019) examines the perceived effects of DP on the public healthcare system in Enugu Urban area, Nigeria, and the burden on patient finances. Benefits of DP were identified as speedier attention, reduced bureaucracy in private practice and reduction of pressure in public hospitals, among others. Reported disbenefits included low commitment to public patients, late reporting, and absence of doctors from work, and sharp practices. The main motives for DP were seen as income enhancement followed by prestige and fringe benefits enjoyed in the public system.
Yu et al. (2020) studied the effect of public hospital managers’ risk and gain perception on their attitude towards physician dual practice in China. The study found that the majority of Chinese public hospital managers are in favor of allowing or implementing PDP with restrictions. Although gain perception is comparatively weaker than risk perception, a stronger influence in determining public hospital managers’ support for physician dual practice is demonstrated. Khim et. al. (2020) assessed dual practice among physicians in Cambodia and indicated that the vast majority (87%) of respondents are public sector employees (with 61.9% in public sector only and 25.4% in both public and private sector). For income satisfaction, physicians employed in both sectors have higher satisfaction than physicians employed in the public sector only.
Therefore, recognizing the high prevalence of multiple job holding in the health sector (as evidenced in previous empirical and practical studies) can contribute to the debate by policymakers on possible schemes that can be developed toward meaningful health system reform.
Methodology
The current study adopted the descriptive method of study. The goal of descriptive research is to describe a phenomenon and its characteristics (Gall, Gall & Borg, 2007). The concern is on WHAT rather than how or why something has happened. Thus, the current study sought to find out how health care practitioners in Kenya perceive dual practice (Patricia & Rangarjan, 2013). The study targeted all health care practitioners from the Kenya Medical Practitioners and Dentists Council (KMPDC) doctors’ retention register. The selection was scientifically guided using Fishers’ formula (Fisher, 1956, Fisher, 1962). The Fisher formula is as follows:
Where;
n= sample size
z= the standard normal deviate value for the level of confidence, for instance 95% level of confidence =1.645.
d= margin of error or level of precision at 0.1 for CI at 95%
p= proportion to be estimated, Israel and Duffy (2009) recommend that if you don’t know the value of p then you should assume p=0.5.
Substituted as in:
Therefore:
n = 68 respondents
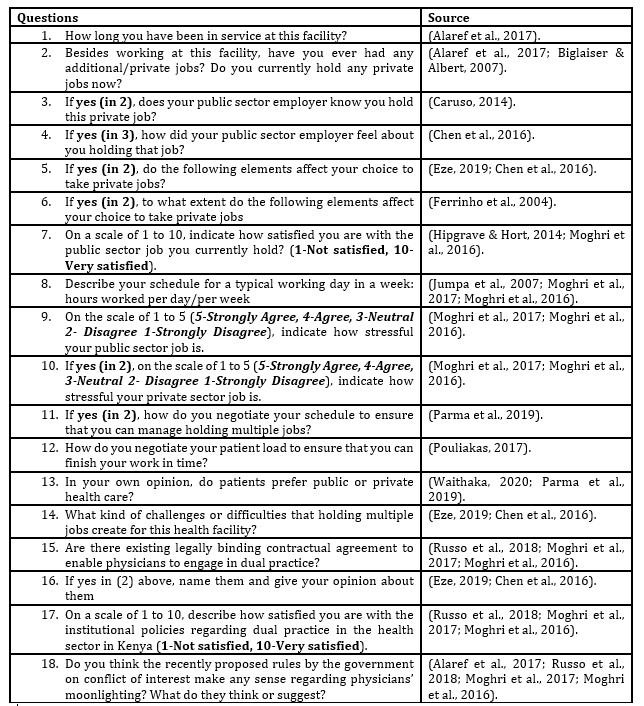
They were targeted purposively. Data collected were primary and qualitative. The data were collected using a semi-structured interview guide. Below are how the questions in the interview guide were sourced and structured:
Table 1: Source of Questions
The collection involved issuing out the interviews via e-mails to the respondents and consistent follow-ups made. Qualitative data collected from the field were analyzed using content analysis which involved identification of recurring themes, patterns, or concepts and then describing and interpreting those categories. The analysis was aided using Excel 2016. Furthermore, the coded data were presented using themes, frequencies, percentages, averages, or standard deviations, among others.
Findings And Discussions
Response Rate
Table 2: Response Rate
Source: Author (2020)
The results in Table 2 show that 68 questionnaires were given out and 49 were properly filled and returned. This return saw 72% response rate which is adequate. This is so because according to Allen (2016) and Rindfuss (2015), a response rate of above 50% is adequate for a descriptive study.
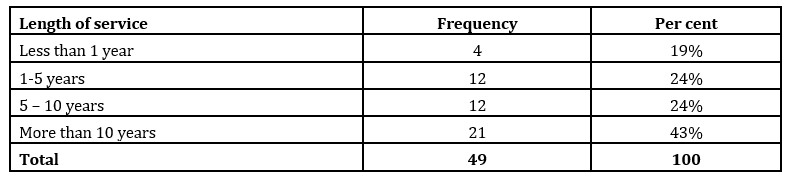
Length of service
The health care providers were asked to indicate their length of tenure in the hospitals. They responded as shown in the table below.
Table 3: Health care practitioners’ length of service
Source: (Survey Data gathered during April 2020)
The findings indicated that 48% of the health care providers have worked in the hospitals for between 1 and 10 years while only 43% of them have been in service for more than 10 years. This indicates that the healthcare providers are professionally experienced in dealing with health management issues.
Holding of Private jobs
Table 4: Responses reading Health care practitioners’ dual Practice
Source: (Survey Data gathered during April 2020)
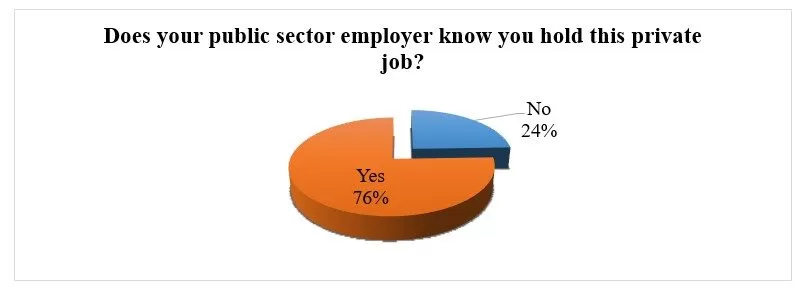
However, the findings noted that there was a Cuban doctor who did not engage in the dual practice. The following was the reason, “Under the contract between Cuban-Kenyan contract-full time doctor in public hospital”. In addition, the respondents were asked to indicate if their public sector employers knew if they held the above stated private jobs. They responded as follows:
Figure I: Knowledge of the public sector employer on holding a private job
Source: (Survey Data gathered during April 2020)
The findings indicate that among the multiple jobholders in the public health care sector, 76% of their employers know they hold the jobs while 24% of them have preferred to moonlight privately without informing their public health sector employer. Nevertheless, for those practitioners who held private jobs with the knowledge of their employers, the researcher asked them to indicate how their public sector employer felt about them holding that job. Respondent 2 responded as follows: “All medical specialists are given Official part-time license to practice privately”.
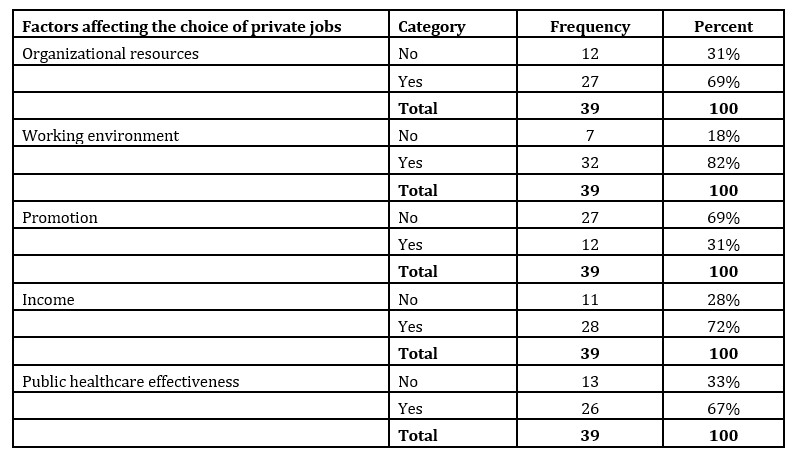
Choice to take private jobs
Table 5: Factors affecting the choice of private jobsSource: (Survey Data gathered during April 2020)
Regarding the factors that have led the health care providers to engaging in multiple jobs, the findings indicate that the majority agreed that the above-named factors have had a significant role to play in influencing dual practice. Aside from all the respondents who indicated that working environment was one of the factors that contributed to their engagement in dual practice, 69%, 82%, 62% and 67% indicated that organizational resources, Income and Public healthcare effectiveness influence their choice of private jobs. However, only 28% of the respondents disputed the argument and stated that income was not a significant factor to consider. This is an indication that the respondents are well remunerated and as such their income is not a factor to consider. In addition, the study notes that working environment is a major factor that, if not taken seriously by the public health facilities, would aggravate the multiple job holding.
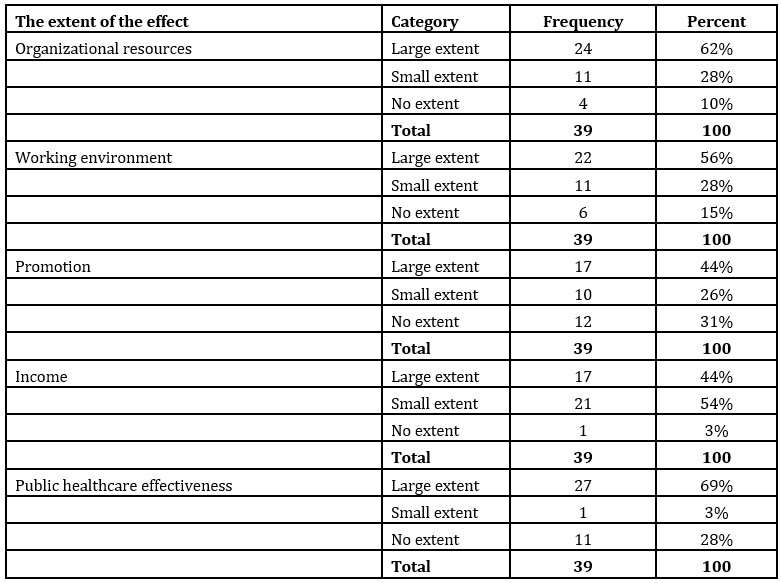
Table 6: Extent of the effect of the factors affecting the choice of private jobs
Source: (Survey Data gathered during April 2020)
The results in table 6 indicate the findings of the extent of the factors that contribute to engaging in multiple job holding. It was indicated that all the factors; 62% of the respondents indicated that organizational resources affect the choice of private jobs to a large extent; 56% of the respondents indicated that working environment affects the choice of private jobs to a large extent; 44% of the respondents indicated that promotion and income affect the choice of private jobs to a large extent while 69% of the respondents indicated that public healthcare effectiveness affect the choice of private jobs to a large extent.
Satisfaction with the public sector job
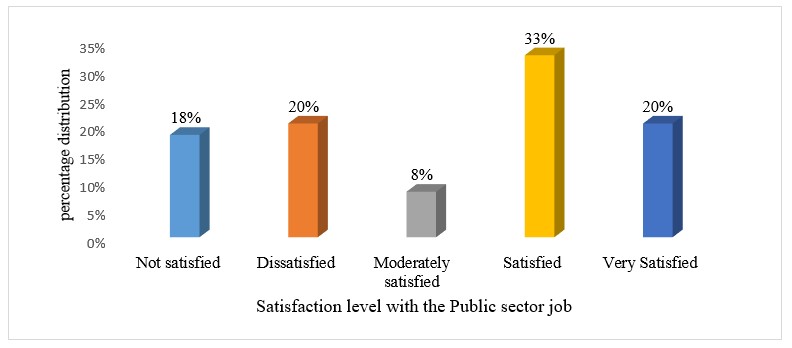
The respondents were further asked to indicate how satisfied they are with the public sector job they currently hold. Given the scale of 1 to 10, 1 and 2 were grouped as 1; 3 and 4 as 2; 5 and 6 as 3; 7 and 8 as 4; while 9 and 10 as 5. They responded as shown in the figure below:
Figure 2: Distribution of the satisfaction of the HCPs with the public sector job
Source: (Survey Data gathered during April 2020)
The findings from the table above indicate that from the 49 respondents analyzed, 53% (33% + 20%) of them acknowledged that they were satisfied with their current public health jobs. This indicates that there is still a milestone to go for the HCPs to be satisfied with the public sector jobs. Therefore, the current study attributed the satisfaction to factors such as organizational resources, working environment, promotion, income as well as the public healthcare effectiveness of the HCPs which were found to have a large extent effect on the choice of private jobs. In addition, the HCPs were requested to describe their schedule for a typical working day in a week that is the number of hours worked per day/per week. Most of them indicated that they worked for eight hours a day in their public jobs which accumulated to 40 hours per week. However, one of the respondents recorded fourteen hours daily working hours.
Stress level at the job
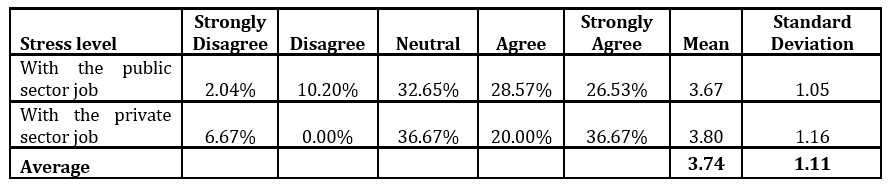
Table 7: Percentage responses of the HCPs’ stress level at their job
Source: (Survey Data gathered during April 2020)
The study findings in Table 7 indicate the responses of the HCPs’ stress level at their job. The findings indicate that the majority of the respondents (55.10%) agree that they are very much stressed by the public sector job while only 56.67% agreed that they were stressed with the private sector jobs. This indicates that they are very much satisfied with holding a private job compared to being in the public sector job. These findings are consistent with the findings in table 3 and 4 which reveal that most of the HCPs are concerned with organizational factors, healthcare effectiveness as well as working environment, which are not sufficiently available in the public health sector.
In addition, the respondents were asked to indicate how they negotiate their schedule to ensure that they can manage holding multiple jobs. These were some of their responses:
Respondent 1: I have committed specific duties I am required to deliver within a specific time on some days and others availed myself for a specified period. Then remain on call as need arises.
Respondent 2:During weekdays I work for the Government and during weekends I work for my Private clinic and Hospital.
The respondents were further asked to indicate how they negotiate their patient load to ensure that they can finish their public work on time. They responded as follows:
Respondent 1: On some days, it depends on the open to close time. Others are on appointment/ schedule for a specified period. Others are on a call basis – particularly emergencies.
Respondent 2:I just work to finish the patient load. We book patients and close the entrance at the designated time.
Respondent 4:Scheduled appointments
Patients’ Preference
The Key health care practitioners were asked to rank patients’ preferences regarding acquiring medical care and their responses were coded as shown below:
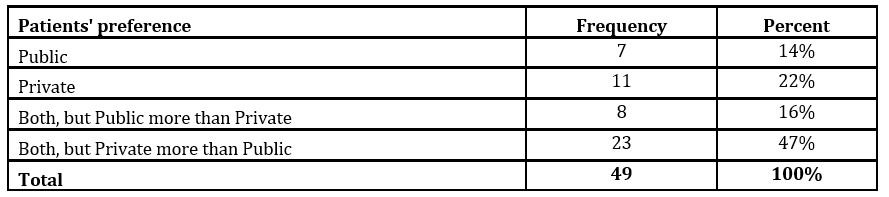
Table 8: Patients’ preferences between Public and Private hospital services
Source: (Survey Data gathered during April 2020)
The findings show that 47% of the health care practitioners indicated that most patients prefer to visit a private hospital and rank a private hospital more than a public hospital respectively. In addition, it was noted that none of them indicated the patients to prefer public hospital more than private healthcare facilities. This implies that the preference of many patients to private healthcare motivates the health care practitioners to set up private health care facilities where they can administer the services alongside the public healthcare services.
Challenges or difficulties of holding multiple jobs
The health care practitioners were further asked to indicate some of the challenges they faced while holding multiple jobs. Respondent 1 indicated: “Access to personnel, Maintenance of standards, Divided loyalty, Pressure to perform as competition irrespective of accessible resource, among others.” Along the same vein, respondent 2 stated the following: “Patients wanting to be seen during weekdays are made to wait or to see alternative doctors and that is very inconvenient. Services at Government hospitals are compromised because consultants are given part-time licenses to practice!” According to respondent 4, availability of time as well as resources limitation/inadequacy are the major problems that affected their moonlighting. Respondent 5 as well indicated that moonlighting creates staff insufficiency due to staff absence.
Dual practice legal framework
The researcher further sought to know if there existed legally binding contractual agreement to enable the health care practitioners engage in dual practice. The findings were presented in the table below:
Table 7: Existing legally binding contractual agreement to enable you engage in dual practiceSource: (Survey Data gathered during April 2020)
The findings indicated that 82% of them indicated there were no legally binding contractual agreement in place to enable the health care practitioners engage in dual practice. Among those who indicated that there existed legally binding contractual agreement to enable them to engage in dual practice, they were further asked to name them and give their opinion about them. One of the respondents indicated that they have a license for part time private practice which is issued officially.
Satisfaction with the existing institutional policies
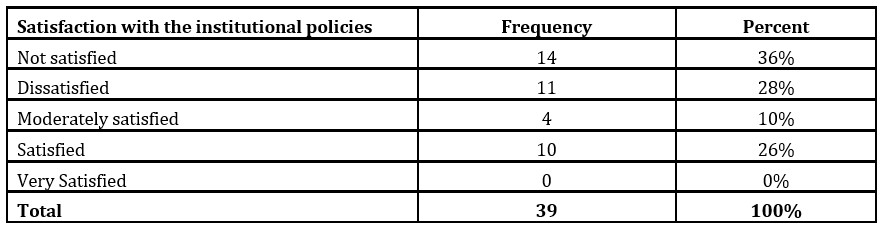
Table 10: Table presenting the responses of the health care practitioners regarding their Satisfaction with the institutional policies
Source: (Survey Data gathered during April 2020)
The health care practitioners were further asked to rate how satisfied they are with the institutional policies in place. The findings in the table above indicate that 64% of the health care practitioners in the survey indicated that they were not satisfied with the existing institutional policies, while only 26% indicated that they were satisfied with the existing policies. This implies that the practice of dual practice in Kenya is still weak to offer health care practitioners a room for moonlighting.
Conclusions And Recommendations
Conclusions
The study concludes that dual practice among Kenyan health care providers is prevalent. However, it is being carried out without optimum autonomy. Many of the healthcare providers fear losing their public health jobs. It has likewise been concluded that holding private jobs alongside public jobs in the health sector is influenced by various internal factors such as organizational resources, Income Public healthcare effectiveness and working environment. However, the extent of the influence is strong with respect to organizational resources’ effectiveness of public healthcare and working environment. The study, therefore, concludes that most of the Kenyan health care providers engage in dual practice due to the unwelcoming working environment and the ineffective public health care facilities.
Along such ineffectiveness comes the poor service delivery in the public health facilities such as long waiting lines at the hospitals. Therefore, most patients would rather prefer to visit the private hospitals where they are attended to professionally and on-time. This likewise contributes to the health care providers choosing to hold private health care jobs. It has likewise been noted that there is no legally binding contractual framework that optimizes the physician’s dual practice. The study thus concludes that the Kenyan legal framework is weak and thus the physicians have little faith in the existing framework since it is not legally binding.
Recommendations
The study recommends the policy makers to design legally binding contractual agreement within the policies that enable the health care practitioners engage in dual practice. This involves re-evaluation and re-shaping of the existing policy in managing contracts for physicians in dual practice. Currently, it has been noted that the existing policy is weak, not standard, and not uniform, since the application is left to the individual hospitals.
Given that the study found the health care providers are more concerned with internal organizational factors such as working environment as opposed to income, the study recommends the ministry of health to improve the working environment of the public health care facilities. In addition, the MoH is recommended to ensure that the public health care facilities are in good working condition.
References
Alaref, J., Awwad, J., Araujo, E., Lemiere, C., Hillis, S. A., & Özaltin, E. (2017). To ban or not to ban? Regulating dual practice in Palestine. Health Systems & Reform, 3(1), 42-55.
Bayat, M., Zalani, G. S., Harirchi, I., Shokri, A., Mirbahaeddin, E., Khalilnezhad, R., … & Akbari-Sari, A. (2018). Extent and nature of dual practice engagement among Iran medical specialists. Human resources for health, 16(1), 1-10.
Biglaiser, G., & Albert Ma, C. T. (2007). Moonlighting: public service and private practice. The RAND Journal of Economics, 38(4), 1113-1133.
Caruso, C. C. (2014). Negative impacts of shiftwork and long work hours. Rehabilitation Nursing, 39(1), 16-25.
Chen, H., Li, M., Dai, Z., Deng, Q., & Zhang, L. (2016). Factors influencing the perception of medical staff and outpatients of dual practice in Shanghai, People’s republic of China. Patient preference and adherence, 10, 1667.
Eze, B. S. (2019). Dual practice of medical professionals in public hospitals in south-eastern Nigeria: an economic and policy analysis(Doctoral dissertation, Swansea University).
Ferrinho, P., Van Lerberghe, W., Fronteira, I., Hipólito, F., & Biscaia, A. (2004). Dual practice in the health sector: review of the evidence. Human resources for health, 2(1), 14.
García-Prado, A., & Gonzalez, P. (2007). Policy and regulatory responses to dual practice in the health sector. Health Policy, 84(2-3), 142-152.
García-Prado, A., & González, P. (2011). Whom do physicians work for? An analysis of dual practice in the health sector. Journal of health politics, policy, and law, 36(2), 265-294.
Hipgrave, D. B., & Hort, K. (2014). Dual practice by doctors working in South and East Asia: a review of its origins, scope and impact, and the options for regulation. Health policy and planning, 29(6), 703-716.
Humphrey, C., & Russell, J. (2004). Motivation and values of hospital consultants in south-east England who work in the national health service and do private practice. Social Science & Medicine, 59(6), 1241-1250.
Israel, S. E., & Duffy, G. G. (Eds.). (2014). Handbook of research on reading comprehension. Routledge.
Jumpa, M., Jan, S., & Mills, A. (2007). The role of regulation in influencing income-generating activities among public sector doctors in Peru. Human resources for health, 5(1), 5.
Khim, K., Goldman, L. N., Shaw, K., Markuns, J. F., & Saphonn, V. (2020). Assessment of dual practice among physicians in Cambodia. Human resources for health, 18(1), 1-8.
McPake, B., Russo, G., Hipgrave, D., Hort, K., & Campbell, J. (2016). Implications of dual practice for universal health coverage. Bulletin of the World Health Organization, 94(2), 142.
Moghri, J., Mohammad, A. R. A. B., Rashidian, A., & Sari, A. A. (2016). Physician dual practice: a descriptive mapping review of literature. Iranian journal of public health, 45(3), 278.
Moghri, J., Rashidian, A., Mohammad, A. R. A. B., & Sari, A. A. (2017). Implications of dual practice among health workers: a systematic review. Iranian journal of public health, 46(2), 153.
Muhudhia, S. O. (2017). Ethico-legal inquiry into strike action by doctors in Kenya(Doctoral dissertation).
Ongori, J. M. (2019). Human resource management practices influencing performance of nursing officers in Nyeri County, Kenya(Doctoral dissertation, KeMU).
Parma, F. A. S. D., Oliveira, R. A., & Almeida, F. A. (2019). Health Professionals’ Perceptions on the Integration of Medical Students’ Training in Family Health Care Units. Revista Brasileira de Educação Médica, 43(1), 175-184.
Pouliakas, K. (2017). Multiple job-holding: Career pathway or dire straits. IZA World of Labor.
Russo, G., Fronteira, I., Jesus, T. S., & Buchan, J. (2018). Understanding nurses’ dual practice: A scoping review of what we know and what we still need to ask on nurses holding multiple jobs. Human resources for health, 16(1), 14.
Waithaka, D., Kagwanja, N., Nzinga, J., Tsofa, B., Leli, H., Mataza, C., … & Molyneux, S. (2020). Prolonged health worker strikes in Kenya-perspectives and experiences of frontline health managers and local communities in Kilifi County. International journal for equity in health, 19(1), 23.
Yu, Y., Cho, W. C., Liu, Q., Fan, X., Chen, X., Yu, X., … & Zhang, X. (2020). Effect of public hospital managers’ risk and gain perception on their attitude towards physician dual practice: a cross-national study in 31 provinces of China. BMC Public Health, 20(1), 1-11.