Volume 2023,
Article ID 935166,
Journal of e-health Management,
14 pages,
DOI: 10.5171/2023.935166
Received date: 24 March 2022; Accepted date: 11 November 2022; Published date: 25 January 2023
Academic Editor: Małgorzata Cygańska
Cite this Article as:
Kirathimo MURUGA and Tatjana VASILJEVA (2023)," A Traditional Literature Review on Physicians’ Dual Practice – Literature Review", Journal of e-health Management, Vol. 2023 (2023), Article ID 935166, DOI:10.5171/2023.935166
Research motivation: The current study seeks to establish the trends in physicians’ dual practice and present existing knowledge gaps that need to be filled based on studies done in other contexts.Research Design/methodology: The desktop research review approach was used in the investigation. This entailed a thorough evaluation of publications on practitioners’ DP. To establish the feasibility of the problem for investigation, 3 selection processes were conducted on the topic under investigation. Main findings: Thus, premised on the foregoing results, the present research believes that an investigation of dual practice is important and beneficial in order to expand on the stream of information accessible. Furthermore, the study should seek an in-depth investigation of dual practice because the study found that dual practice has negative consequences on the health care system. This results in the reduction in workforce in the public sector and cases such as poor primary healthcare seem to scale up. There is no agreement on the overall results of moonlighting in the healthcare industry and, likewise, no single and easy solution to the issue of whether this profession should be governed by the ministry of health. In a nutshell, the argument revolving around dual practice is still unclear and unsatisfactory on whether to allow it or disallow it. Its disadvantages have been commonly raised by many researchers, to affect the public healthcare delivery, therefore, requiring further investigations. Despite the above, dual practice in the health sector attracts the most interest because it seeks the eye of all the relevant stakeholders to work together to ensure the balance between public and private health care provision. Contributions to Practice: This is a preliminary investigation in Kenya that other writers from Sub-Saharan Africa might utilize as a foundation for subsequent research. The study ‘s conclusions might help create legislation in the area of regulating agreements for doctors in DP. The present approach is ineffective, nonstandard, and inconsistent because implementation is left to independent clinics. The data will aid in the development of a management framework for the rates of DP and the parameters that contribute to it in Kenya.
Dual practice (DP) is a common phenomenon in which public representatives labor both inside and beyond the governmental domain. Private employment may be done inside or outside governmental establishments, but it is done for personal gain or as part of a profit-sharing deal with the appropriate state entity. DP is prevalent among, but not limited to, the healthcare practitioners; instructors, professors, government defense personnel, and potentially any paid specialist may do private work alongside their state job. Nevertheless, DP in the healthcare system piques the most attention since it addresses a global concern that may be exceedingly expensive, is fundamentally unreliable, and relies on the supply of expert care (Bloom et al. 2008). Besides, with the high ranking of the latest government financed attempts to enhance healthcare quality (Ravishankar et al. 2009) and flourishing study attention in human assets for medical care (Ranson et al. 2010), public practitioners, particularly practitioners, have paid close focus to DP (Kiwanuka et al. 2011).
DP is prevalent in nations with varying levels of growth and socioeconomic position, political systems, and population and healthcare issues. The UN (where it is uncommon) and Canada (where it is technically prohibited) are 2 different outliers, although overt or covert DP is frequent even in countries or nations where it is formally prohibited. The prevalence of DP in the medical industry varies greatly; in certain countries, most of the general populace practitioners also operate commercially, whilst in others, only leading practitioners or experts do that (Garcia-Prado & Gonzalez, 2011). Reports of healthcare worker behaviors in a number of South and East Asian countries indicate DP by practitioners throughout the area (Garcia-Prado & Gonzalez, 2011). Nevertheless, there is very little proof of its effectiveness. Their fear is that DP will limit health-care accessibility, reliability, and efficacy, yet there are both philosophical and pragmatic arguments why DP may be beneficial altogether.
DP is common in many medical care regimes. The phenomenon has received recognition in conjunction with debates concerning its harmful influence on government medical care service. The prohibition or limitation of DP is often proposed. Socha (2010) analyzed and extensively evaluated scientific and philosophical results on DP and its consequences for public health care delivery. The researcher stated that scientific information on the influence of DP on medical care delivery is limited. Nevertheless, philosophical investigation demonstrated that DP might have both beneficial and harmful consequences. The author found that more study was necessary to determine why practitioners partake in DP and if the prospective expenditures of DP outweighed the expenses/costs of implementing DP (dual practice) limits.
Privately-owned firms control a large and rising portion of the medical support providing sector. For example, in forty emerging nations, fifty-five per cent of doctors engaged in the commercial domain, and twenty-eight per cent of medical system facilities were commercial facilities (Ferrinho et al., 2004). Asia accounted for more than sixty per cent of private industry inputs to medical funding and is the region of the globe where the business industry traditionally plays a major contribution. For instance, in Malaysia, the percentage of clinicians in the commercial sector rose from forty-three per cent in 1975 to seventy per cent in 1990. In Indonesia, fifty per cent of the clinics are independently owned and operated. Thailand’s commercial medical bed occupancy increased from five per cent in 1970 to seventeen per cent in 1989.
Conversely, DP in the medical field piques the most attention since it addresses a global issue that may be exceedingly expensive, is fundamentally unexpected, and implies the availability of expert care. According to studies, permitting physicians to practice simultaneously is expensive and has a detrimental influence on the efficiency of government medical services (Gonzalez et al., 2018; Vejdani, et al., 2020). The growing DP and departure of medical personnel endangers the medical program’s efficacy (Gacevic et al., 2018). This is linked to consequences such as physician burnout, which is linked to self-reported medical mistakes and completely undermines the provision of quality care. Physician job discontent is linked to lower client experience (Rathert et al., 2018). Having allowed DP may also offer to lessen clinical long waiting periods or enhance health care accessibility, particularly for poor residents/members of the public. However, the public-private interplay may have opportunity schemes to cut operating hours, divert service users/patients to personal health centers robbing the public hospitals of the public income and quality of care (Moghri, 2017).
However, theoretically, dual practice might bring both positive and negative effects. Thus, there is need for further research as to why physicians are engaged in dual practice and whether potential costs of dual practice outweigh the costs of enforcing restrictions on dual practice. Chen et al. (2016) revealed that 63.0% of the respondents supported dual practice. Medical staff who belonged to the surgical department or held positive belief of dual practice were more willing to participate in dual practice. Likewise, the practice could lead to the transfer of expert knowledge (knowledge spill over) from the private sector since they have enough financial resources to acquire sophisticated technology (Barnett et al., 2020; Moghri et al., 2017).
Thus, given the two possible outcomes, dual practice tends to rely on the policy recommendations of the given health system. That is, there is no consensus on the net effects of dual practice in the health sector, and there is no unique and simple answer to the question of whether this practice should be regulated. These are open questions that continue to be debated by health economists, health policy researchers, and policy makers (Garattini & Padula, 2018; Xu et al., 2022). The lack of consensus forms the background of the current paper.
Statement of the problem
Medical DP is a regular occurrence, with clear consequences for practitioners’ labor availability, quantity of national healthcare output, and effectiveness of medical care operations (Garattini & Padula, 2018; Mahendradhata et al., 2017; Moghri, 2017; Xu et al., 2022). Dual practice consequences for government medical care are given special consideration. The reality that a physician offers medical services both in the government and non-government sectors is the primary cause of contention in the governance discourse, as the presence of doctor DP is regarded to be in conflict with the ideal labour force structures pertaining to the labour contracts. As a result, the necessity for legislative mechanisms governing medical DP is frequently emphasized (Khim, 2020). The socioeconomic research on medical DP and its implications for the state healthcare system is immature and sparse. According to the research, DP has both beneficial and bad consequences on universal healthcare, and determining the net impact is challenging (Pouliakas, 2017).
Several negative impacts of dual practice have been pointed out including absenteeism (Pouliakas, 2017) and shirking during official work hours. To that extent, patients are forced into the private sector by dual practitioners preferring private work. To promote private care, the behaviour has led to the alteration of quality of care or processing hours (Khim, 2020; Muhudhia, 2017; Xu et al., 2022). Other effects of DP include inadequate delivery of services in the government domain with instances of recurrent and debilitating physicians’ demonstrations, unrestricted or downright misappropriation of goods from government institutions, or misuse of public service, care professionals, or infrastructure for privatized customers (Ongori, 2019; Waithaka et al., 2020). There is a dearth of information regarding how information from DP overflows affect productivity (Barnett et al., 2020; Glied & Hong, 2018, Moghri et al., 2017).
During the ending year of 2011 and ending year of 2012, Kenya saw two large countrywide physicians’ strikes, both of which resulted in tragic deaths and economic disruption (Muhudhia, 2017). By the start of 2015 and thought the first quarter of 2017, several individuals succumbed or became disabled as a result of a lack of accessibility to healthcare (Masika, 2017). Likewise, many individuals were obliged to pursue medical treatment from private entities, assuming significant budgetary liabilities. Even during demonstrations, medical professionals advocated for more pay, a healthier workplace climate, advancements, and enough facilities. The examples highlight a distinct aspect in Kenya’s medical system that necessitates such research. A managerial framework/model was, thus, essential for achieving an equilibrium between the private and public medical fields.
Additionally, there is little empirical data available in the Kenyan setting for the technique, raising many questions even though it has drawn both good and unfavorable criticism. For example, Khim et al. (2020) studied doctors in Cambodia, Bayat et al. (2018) examined Iranian healthcare experts, and Atinga (2021) examined uninsured clinics in Ghana; as a result, the conclusions from these studies could not be extrapolated to other African nations, creating a contextual gap. Iran served as the setting for the Bayat et al. (2018) investigation. This investigation thus exhibits a conceptual flaw since, according to others, it does not consider religion in its whole. The present investigation bases its analysis of the effects of clinicians’ DP on the medical industry on this principle. The research aims to add/contribute to the body of knowledge about how DP of both government and commercial physicians affects the Kenyan healthcare framework, in order to advance to the national conversation about these issues and their assessment, administration, management, and evaluation.
Literature Review
Russo et al. (2018) aimed to comprehend physicians’ DP and the motivations behind their dual employment. Following the methodological procedures of Arksey and O’Malley and the PRISMA criteria, the investigation reviewed caregivers’ DP. The survey found that amongst the cited motivations for partaking in these behaviors were the chance to enhance a meager wage, but also discontent with the primary employment and the versatility given by various work-holding situations.
In their 2018 study, Bayat et al. sought to understand the scope and character of dual practice participation among Iranian medical experts, employing survey polls to gather information from healthcare professionals at 925 clinics in Iran. Particularly in full-time regional experts, Iran healthcare experts were observed to have a rather significant degree of DP. Nevertheless, they are completely outlawed and obtain additional compensation for working full-time; stringent laws and monetary support alone may not be sufficient to eradicate DP in professionals, and it now must be remedied in accordance with the circumstances of each region and its specific countries.
Drawing on a healthcare-based investigation of 483 doctors at 10 government institutions in 4 regions of Vietnam, Do and Do (2018) examined the impact of DP for public clinic doctors in that country. Nevertheless, the plurality of double-working clinicians, according to the survey, said that they would be prepared to leave up their private practices provided certain requirements were satisfied, including an increment in their base pay or non-cash perks. This paper highlights the considerable obstacles to DP, especially its potential monetary costs and consequences on accessibility to and the effectiveness of medical care.
Khim et al. (2020) evaluated the DP of doctors in Cambodia. Nearly 50% of the participants work multiple jobs. Clinicians who work in both the public and private domains are more satisfied with their remuneration than those who solely work in the public sector. Our study of UHS trained doctors revealed a high rate of simultaneous employment ownership in Cambodia, which adds to the conversation as crucial data that may be applied to significant transformation.
In all 3 dimensions of the 3 categories, simultaneously working doctors, as per Atinga (2021), valued private clinics more than public institutions, leading them to participate in DP. Leadership qualities, administration, and favourable workplace circumstances in privatized as opposed to governmental institutions had a significant impact on the patient-centeredness and dedication to client experience of simultaneously working doctors. In privatized institutions, psychological capital had a significant impact on simultaneously working doctors/dual practitioners’ client satisfaction, but not on government venues.
Chen et al. (2016) investigated variables impacting medical personnel and outpatients’ perceptions of DP in China. The research sought to investigate the perceptions and acceptability of DP among hospital personnel and outpatient care, as well as the elements that influence individuals’ perceptions. According to the report’s results, 63 percent of participants endorsed DP. Medical professionals who worked in the surgery section or who believed in DP were more inclined to engage. Furthermore, the public relations operations of DP and the HRM framework/system of clinics were significant variables influencing health facility personnel attitude. According to the findings of an aftercare assessment, 44.5 percent of participants stated that DP may make it easier to visit a specialist. Furthermore, demographic variables impacted AFTER-CARE/outpatients’ perceptions considerably. Because the investigation was done in China rather than Kenya, generalizing its conclusions to the Kenyan setting was impracticable.
Abera, Alemayehu, and Herrin (2017) investigated the effect of DP among clinicians in Ethiopia. A cross-sectional research study employing mixed techniques was done in 6 regionally comparable government hospitals. From 31 doctors and 449 individuals, 90.3 percent were involved in some form of DP, 51.6 percent owned commercial clinics beyond the government institution, 16.1 percent operated part-time in commercial hospitals, and 22.6 percent in the public hospitals. Monetary augmentation was the key motivation given by 100 percent of the clinicians for participating in DP. Doctor preservation in the government sector was one of the beneficial consequences of DP from the views of both management and doctors. 20.3 percent were recommended from a private hospital just previous to their present admittance cyclical while 19.8 percent were redirected by health staff in government facilities.
Methodology
Steps in Literature Review
The desktop research review approach was used in the investigation. This entailed a thorough evaluation of publications on practitioners’ DP. To establish the feasibility of the problem for investigation, 3 selection processes were conducted on the topic under investigation.
Identification and Searching process
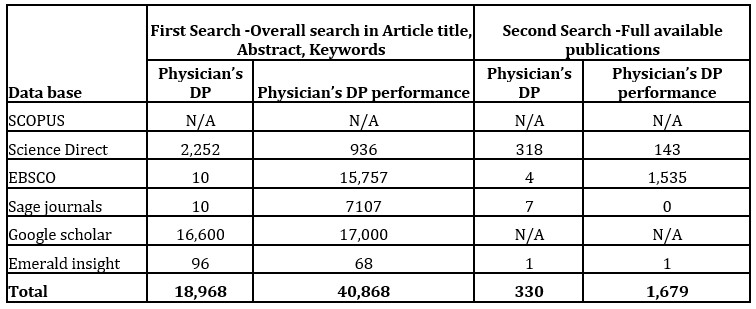
This is the initial step, which included the preliminary recognition of all publications from various data sets that were founded on DP. The initial scan was performed in a generalized manner by examining the papers by topic, synopsis, and their keywords. A subsequent scan focused on fully accessible papers on the topic of doctors’ DP. A total of studies that were studied totalled to three hundred and thirty (330) articles. The Web of Science data base was not accessible to the researcher due to limitations in the rights to the database and as such the researcher opted to not pursue that direction.
Table 1: Searching processSource: (Research Survey Data gathered on 30th August 2019).
Filtration Process
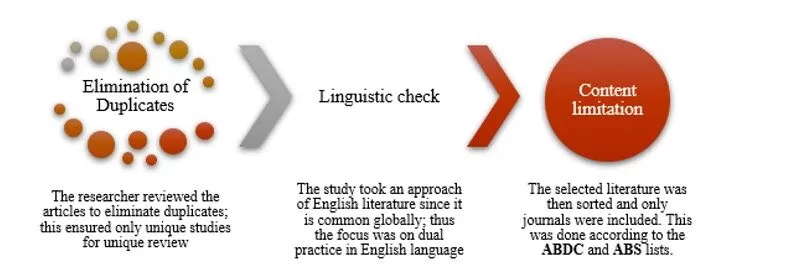
Fig 1: Filtration process (by the authors)
The screening procedure was carried out based on the articles’ currency (2014 to 2019). This subsection describes the method used by the research to analyze the research. The investigator evaluated the publications to remove repetitions, ensuring that only original investigations were examined. Because English language is widely used around the world, the investigation focused on DP in English. The reviewed publications were considered once the collected material was filtered. This was carried out in accordance with the ABDC and ABS listings.
Selection Process
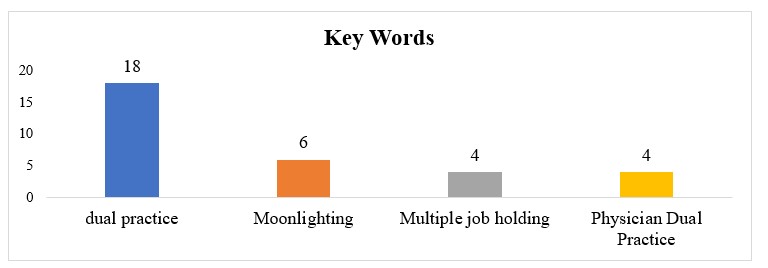
Following the screening, the 3rd (third) phase involves selecting completely accessible articles. Restricting the material to just completely available journals produced precision and enabled the author to concentrate on papers relating to DP, which were divided into top key terms as described in Figure 2.
Top Key words
Fig 2: Top keywords (by the authors)
The author found thirty-two publications were acceptable for evaluation after doing an extensive exploration using the leading key terms. The investigation delivered the data in tables and figures which were analyzed employing Excel spreadsheet techniques.
Findings: What Makes Physicians’ Dual Practice Research Promising?
Total Publications by Year
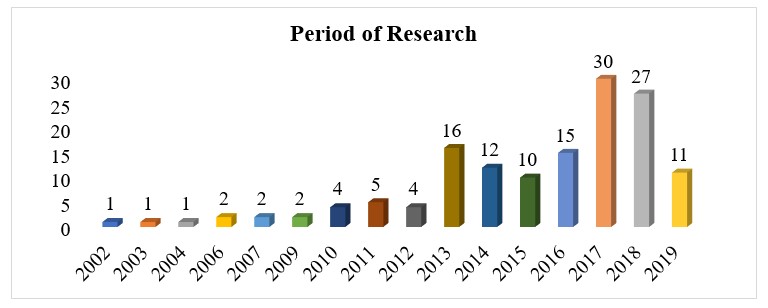
The research aims to determine the overall quantity of articles on the topic of study from the year 2002. The emphasis, nevertheless, was from the year 2014 to the year 2019. The results were reported in fig 3:
Fig 3: Annual publications based on the analyzed key words
According to the entire amount of study evaluated, the majority of the publications (thirty) on DP were undertaken in 2017, while twenty-seven of them were undertaken in 2018. The plurality of the research was conducted between 2013 and 2018, showing that the issue is still relevant in the present era.
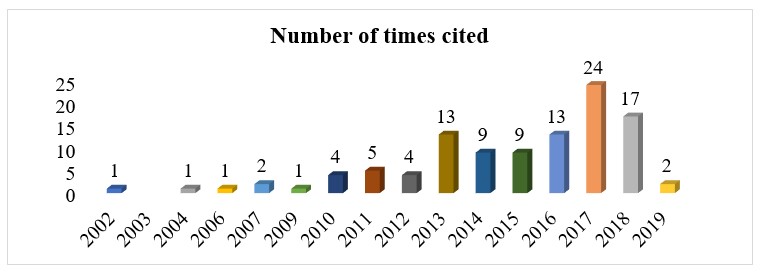
Sum of Times Cited by Year
The study sought to further look into the key word analysis of “Physicians’ dual practice” in different data bases based on the sum of times cited by year.
Fig 4: Sum of Times Cited by Year
The findings revealed that the majority of the articles under survey were most cited in the year 2017 (24) and 2018 (17). Generally, the study noted that most of the articles were most cited between 2013 and 2018.
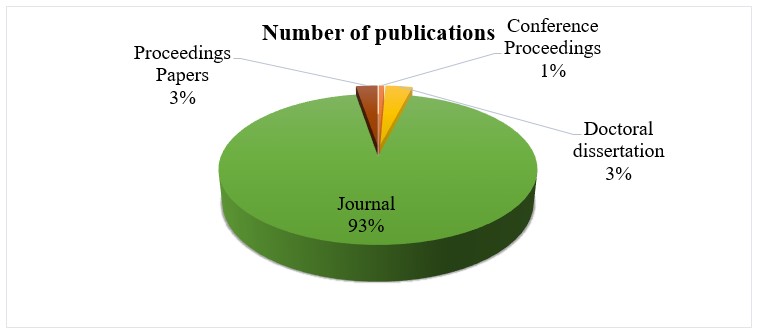
Number of publications
Fig 5: Number of publications
According to the examination of the number of papers published with regard to the principle/main phrases, the bulk of the research (ninety-three per cent) were research papers posted/published on multiple journal websites. Furthermore, the survey noted that 3 percent of the papers were both conference manuscripts and doctorate dissertations, whereas just 1 percent were conferences’ hearings. This implies that research on DP adds significantly to scholarly understanding regarding DP and so appears to be a relevant topic for discussion.
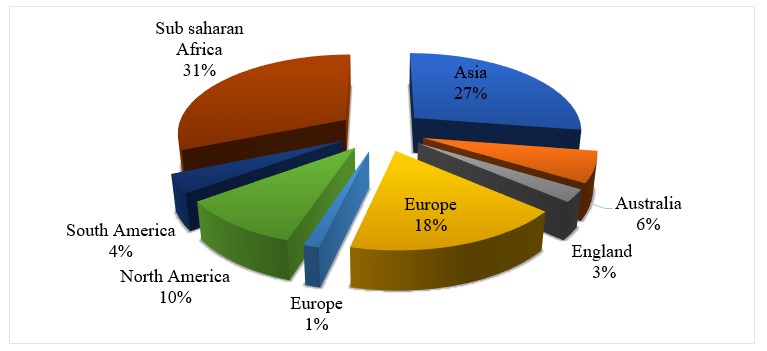
Geographic origin of key studies on Physicians’ dual practice
Fig 6: Geographic origin of key studies on Physicians’ dual practice
The findings indicated that the majority of the studies (58%) have been carried out in the Sub-Saharan and Asian region that is 31% and 27% respectively, while 10% of them have been conducted in the North American region, while 6% have been conducted in Australia. This proves the need of studies to be carried out in low and middle earning countries of which most are situated in the Sub-Saharan and Asian region. These findings are in line with those of Hipgrave and Hort (2014) whose study was based in South and East Asia. Their study noted that, if properly controlled, DP can increase healthcare accessibility, the breadth of treatments available, and physician experience. Conversely, poorly governed DP could have a detrimental impact on government health‐care availability, quality, effectiveness, and equality, since physicians frequently want a blend of government and privatized practice that optimizes their pay and other advantages. This is an indication that the subject under dual practice has been of significance to many of these countries and since Kenya is one of the countries, this warrants more research on the same subject in order to contribute to solving the problem surrounding the practice especially in the heath sector.
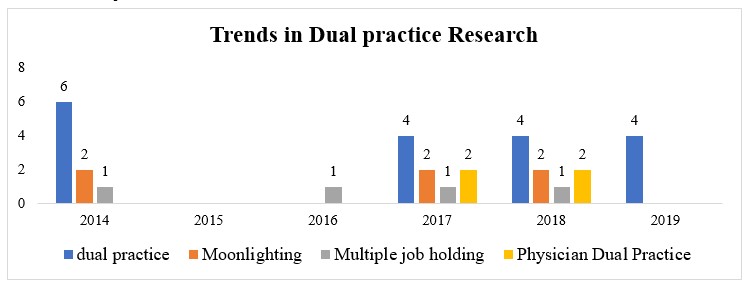
Historical Trends in Dual practice Research
Trends in Dual practice Research
Fig 7: Trends in Dual practice Research
Over the period the studies were researched, the study found that Dual practice was the most researched in 2012 and 2014. Multiple Job holding was likewise found to be the most researched subject between 2017 and 2018. From 2017 to 2019, the subject under study was mainly dual practice. It was likewise noted that physicians’ dual practice surfaced in 2017. Thus, based on the findings, it can be deduced that the subject of dual practice is a relevant topic that keeps on gaining prominence over the years warranting further studies on the same subject in the current year (2019).
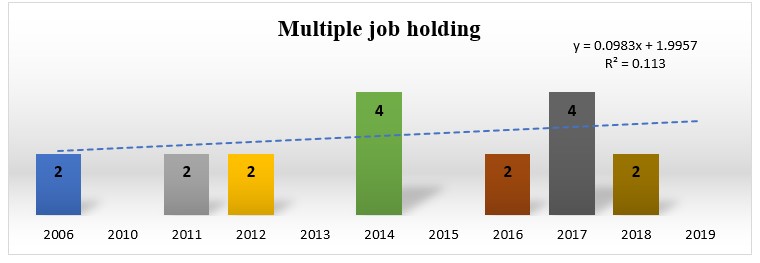
Multiple Job Holding
Fig 8: Trends in Multiple Job Holding
From the trend analysis done based on the subject ‘multiple job holding’, it was discovered that there has been an upward trend as indicated by a positive beta value of 0.394. However, it was noted that in the year 2019, there were no studies done on the same subject, thus presenting a gap that needs to be filled.
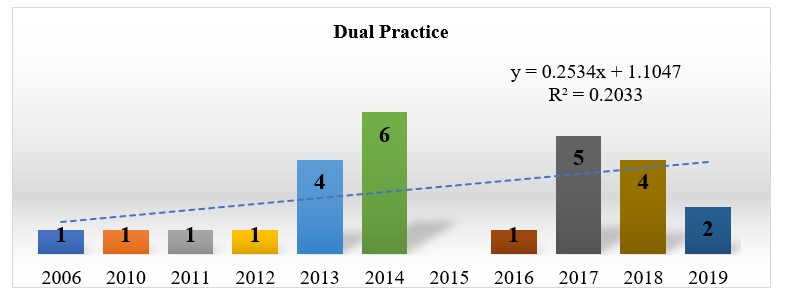
Dual Practice
Fig 9: Trends in Dual Practice
From the trend analysis done based on the subject ‘Dual Practice, it was likewise noted that there has been an upward trend in the research done on the subject. Since the current study focused on studies since the year 2014, the study noted the majority of the articles were done in the year 2014 indicated by 6 journal articles, followed by 2017 with 5 articles. In the year 2019, only 2 articles have been researched on based on the subject under review. This warrants more studies in the same area in order to fill the existing gap.
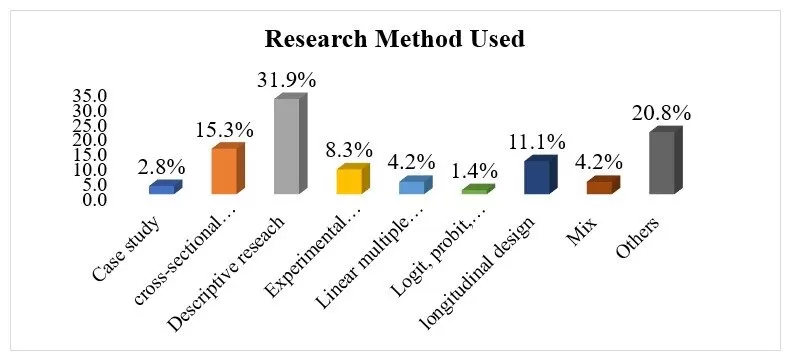
Published Empirical Research
The study sought to investigate the methodologies used by the studies under research. The findings were presented in the figure below:
Fig 10: Research methods used
It was revealed that the majority of the studies that were done based on the subject ‘dual practice’ used the descriptive research design (31.9%). This was followed by other methods that were used represented by 20.8%, while cross-sectional design was noted to be used by 15.3% of the studies. This means that the majority of investigations on DP have recognized the significance of explanatory study methodology. The conclusions are congruent with the findings of Nassaji (2015), who recognized descriptive study architecture as a credible strategy for exploring particular themes and as a forerunner to larger quantitative investigations. Although there are some legitimate issues regarding statistical significance, provided the scientist understands the limits, this sort of experiment is a useful scholarly instrument. This research focuses on what happened rather than how or why it happened. As a result, evaluation and assessment procedures are frequently utilized to obtain statistical findings/information (Gall et al., 2007). In such investigations, information may be obtained subjectively but is frequently objectively evaluated using counts, percentages, probabilities, or other probabilistic approaches to determine correlations. However, subjective research is more methodical and frequently necessitates a thorough gathering of information from numerous perspectives to gain a better knowledge of specific respondents’ ideas, emotions, and perspectives. A qualitative study analyzes knowledge in a comprehensive way, including the use of content and narrative to expound to the outcomes of a particular survey.
Research Gaps
The gap produced by variations in contextual features is known as the contextual gap. Fiallos Rivera (2014), for example, focused on dual practice in the setting of the Emergency Department. Although the results emphasize precision, the research focus that extends beyond the Emergency Department/unit of any one medical care provider remains unresolved. Adebo (2013) demonstrated that having several occupations had no detrimental medical consequences for producers. This is a beneficial discovery for farmers, and the study may have consequences in other situations as well. As a result, the present research tries to generalize the DP in the medical industry, particularly in Kenya.
Geographical gaps are knowledge gaps that take into account future opportunities or absent scientific material in a geographical region which has not previously been investigated. Abera, Alemayehu, and Herrin (2017), for example, were geographically centered on North Ethiopia, therefore, although providing factual data on the incidence of DP, the conclusions were determined to be restricted in bounds and require generalization to apply to other adjoining nations. This was due to the fact that the investigation only ever used four hundred and forty-nine (449) individuals in the 6 Ethiopian study facilities.
Paina Bergman (2014) sought to advance the application of systems thinking in healthcare sector by exploring dual practice and its management in Kampala, Uganda. Given the close link and share of a lot of characteristics between Kenya and Uganda, the findings of the study provide applicable findings to be embodied. However, there are some economic and political variations between the two countries which warrants a study to be done specifically in Kenya in order to ascertain the link. Considering the proximity of relationship and shared traits of Kenya and Uganda, Bergman’s (2014) results offer appropriate conclusions to be incorporated. Nevertheless, there are significant institutional and socioeconomic differences between the 2 nations that necessitate research conducted exclusively in Kenya to determine the relationship. Ologbon (2017), on the other hand, chose 100 participants as the population of measurable elements, which is far too little to be extrapolated to Nigeria, let alone another neighboring country. The present research therefore recognizes the methodological problem and tries to fill in the discrepancy to tackle the dilemma on a broader scale.
The methodological gap is the difference that appears as a consequence of constraints in the study methodology and processes. Zhang and Liu (2018) used a cross-sectional approach to target 136 major institutions throughout 31 states and 2498 doctors. To acquire meaningful and truthful facts about DP, the analysis unit was suitable. Unfortunately, the research did not clarify whether either quantitative or qualitative data would be used. Furthermore, no supplementary information was used to enhance the findings. As a result, the research lacked rigour and, to a large part, reveals pathways in skewed outcomes.
Similarly, using an experimental approach, it can be seen in the research by Schubert et al. (2017) that the utilization of trials misses to discuss/analyze descriptive info/data, which needs subject answers to be given exactly as they are. This is due to the fact that experimentation includes the modification of an autonomous factorvis a vis the predicted variable, which may jeopardize the originality of a study. Although being driven by a descriptive study design, Kadri (2016) sought all doctors specialized and/or licensed in the United States to date . Because the exact figure was not stated, the investigation had a constraint in the extent of its observational unit. Additionally, considering the benefits of using mixed approaches in researching, Aziz’s (2015) work was seen as a model for how to properly examine dual practice. Nevertheless, the investigation’s sample was far too small (18 medical healthcare professionals) to merit quality/robust scientific investigation and generalization of the conclusions to the full community.
A conceptual gap occurs when there is a mismatch between the patient’s cognitive representation of the program and how the system really functions. For example, the results’ idea of Njiru’s (2013) study varied from the current investigation in that the target was overall personnel productivity, but the present analysis concentrates on DP. Aziz et al.’s (2015) study was also focused on health professionals’ workplace conditions and employment contentment. Scientifically, the investigation provided a method for how the medical care industry might enhance medical employees’ contentment by changing their working circumstances. The results, nevertheless, revealed no indication of how the factors contribute to DP.
Paina (2014) concentrated solely on government health personnel. This excludes the contribution of private health care professionals in the industry. Laschinger, Zhu, and Read (2016) developed an in-depth and supply-side perspective to doctor engagement in medical care departments. Nonetheless, the results might have been useful if they had been slanted in favor of their point of view on DP. Because dualism has a detrimental impact on individual productivity, Schauer (2018) observed that well-implemented regulations can dramatically reduce dualism and imbalances while increasing welfare and performance. Unfortunately, because the research misses to confront dualism in the medical area, it is deemed too generic to give concrete conclusions.
Discussions, Conclusions and Recommendations
Trends in Research on Dual Practice
According to the literature study, the bulk of the research was published and referenced between 2013 and 2018, showing that the issue is still relevant in the present century. According to the data, the majority of the papers on doctors’ DP were from prestigious journals released on multiple publication portals. This demonstrates the patient’s legitimacy in the eyes of numerous researchers. Furthermore, the research study offers proof as to why the particular topic under evaluation is important in the African perspective, as most of the research findings were from the Sub-Saharan regions.
A pattern supported the preceding by revealing that, within the time period studied, numerous writers expressed worries about DP. This was based on an upward pattern in the keywords of the research from 2012 to 2019. Thus, based on the findings, it can be deduced that the subject of dual practice is a relevant topic that keeps on gaining prominence over the years warranting further studies on the same subject in the current year (2019). The study also discovered that descriptive research design was the most popular method for surveying studies on dual practice. This is because descriptive research focuses on what happened rather than how or why it happened. As a result, observation and assessment procedures are frequently utilized to obtain survey data (Gall et al., 2007). These investigations may capture information subjectively, but they are frequently statistically examined using numbers, proportions, ratios, or other statistical approaches to identify correlations. Quantitative investigations in descriptive analysis enable scholars to portray the research findings in an easier and understandable way. Inferential data analysis to find repeating patterns, trends, or theories, followed by description and interpretation of such groups, is how qualitative research gathers knowledge.
Conclusions
Thus, premised on the foregoing results, the present research believes that an investigation of dual practice is important and beneficial in order to expand on the stream of information accessible. Furthermore, the study should seek an in-depth investigation of dual practice because the study found that dual practice has negative consequences on the health care system. This results in the reduction in workforce in the public sector and cases such as poor primary healthcare seem to scale up. There is no agreement on the overall results of moonlighting in the healthcare industry and, likewise, no single and easy solution to the issue of whether this profession should be governed by the ministry of health. In a nutshell, the argument revolving around dual practice is still unclear and unsatisfactory on whether to allow it or disallow it. Its disadvantages have been commonly raised by many researchers, to affect the public healthcare delivery, therefore, requiring further investigations. Despite the above, dual practice in the health sector attracts most interest because it seeks the eye of all the relevant stakeholders to work together to ensure the balance between public and private health care provision.
Recommendations
This is a preliminary investigation in Kenya that other writers from Sub-Saharan Africa might utilize as a foundation for subsequent research.
The study’s conclusions might help create legislation in the area of regulating agreements for doctors in DP. The present approach is ineffective, nonstandard, and inconsistent because implementation is left to independent clinics.
The data will aid in the development of a management framework for the rates of DP and the parameters that contribute to it in Kenya.
References
Abera, G. G., Alemayehu, Y. K., & Herrin, J. (2017). Public-on-private dual practice among physicians in public hospitals of Tigray National Regional State, North Ethiopia: perspectives of physicians, patients and managers. BMC health services research, 17(1), 713. https://doi.org/10.1186/s12913-017-2701-6.
Alaref, J., Awwad, J., Araujo, E., Lemiere, C., Hillis, S. A., & Özaltin, E. (2017). To ban or not to ban? Regulating dual practice in palestine. Health Systems & Reform, 3(1), 42-55. https://doi.org/10.1080/23288604.2016.1272980.
Atinga, R. A. (2021). Beyond wages: Why dual practice physicians discriminate care quality towards private patients in Ghana. International Journal of Healthcare Management, 14(4), 1221-1229. https://doi.org/10.1080/20479700.2020.1756102.
Barnett, M. L., Olenski, A., & Sacarny, A. (2020). Common Practice: Spillovers from Medicare on Private Health Care(No. w27270). National Bureau of Economic Research. https://www.nber.org/system/files/working_papers/w27270/w27270.pdf.
Bayat, M., Shokri, A., Khodadost, M., Fattahi, H., Mirbahaeddin, E., Harirchi, I. … & Khalilnezhad, R. (2018). Factors influencing medical specialists’ dual practice in the Islamic Republic of Iran. Eastern Mediterranean Health Journal, 24(9) 877–887. https://doi.org/10.26719/2018.24.9.877.
Bazyar, M., Rashidian, A., Jahanmehr, N., Behzadi, F., Moghri, J., & Doshmangir, L. (2018). Prohibiting physicians’ dual practice in Iran: Policy options for implementation. The International journal of health planning and management, 33(3), e711-e720. https://doi.org/10.1002/hpm.2524.
Garattini, L., & Padula, A. (2018). Dual practice of hospital staff doctors: Hippocratic or hypocritic? Journal of the Royal Society of Medicine, 111(8), 265-269. https://doi.org/10.1177%2F0141076818783332.
Gonzalez, P., Montes-Rojas, G., & Pal, S. (2018). Dual Practice of Health Workers: Theory and Evidence from Indonesia. IZA Discussion Papers, No. 11038, Institute of Labor Economics (IZA), Bonn http://hdl.handle.net/10419/171022.
Hipgrave, D. B., & Hort, K. (2014). Dual practice by doctors working in South and East Asia: a review of its origins, scope and impact, and the options for regulation. Health policy and planning, 29(6), 703-716. https://doi.org/10.1093/heapol/czt053.
Khim, K., Goldman, L. N., Shaw, K., Markuns, J. F., & Saphonn, V. (2020). Assessment of dual practice among physicians in Cambodia. Human Resources for Health, 18(1), 1-8. https://doi.org/10.1186/s12960-020-0461-6.
Mahendradhata, Y., Trisnantoro, L., Listyadewi, S., Soewondo, P., Marthias, T., Harimurti, P., & Prawira, J. (2017). The Republic of Indonesia health system review. Health Syst Transit. 7 (1): 1–292. https://apps.who.int/iris/handle/10665/254716.
Moghri, J., Mohammad, A. R. A. B., Rashidian, A., & Sari, A. A. (2016). Physician dual practice: a descriptive mapping review of literature. Iranian journal of public health, 45(3), 278. https://pubmed.ncbi.nlm.nih.gov/27141489/.
Moghri, J., Rashidian, A., Mohammad, A. R. A. B., & Sari, A. A. (2017). Implications of dual practice among health workers: a systematic review. Iranian journal of public health, 46(2), 15–164. https://www.ncbi.nlm.nih.gov/pubmed/28451549.
Nassaji, H. (2015). Qualitative and descriptive research: Data type versus data analysis. 19(2):129-132. doi:10.1177/1362168815572747.
Ongori, J. M. (2019). Human resource management practices influencing performance of nursing officers in Nyeri County, Kenya(Doctoral dissertation, KeMU). http://repository.kemu.ac.ke/handle/123456789/767.
Salmon, K., & Fan, J. (2019). An update on characteristics of dual PharmD/MBA programs in the United States: 2016–2017. Currents in Pharmacy Teaching and Learning, 11(5), 469-475. https://doi.org/10.1016/j.cptl.2019.02.009.
Vejdani, M., Kokabisaghi, F., & Moghri, J. (2020). Factors affecting physicians’ dual practice in Iran. https://doi.org/10.21203/rs.3.rs-80637/v1.
Waithaka, D., Kagwanja, N., Nzinga, J., Tsofa, B., Leli, H., Mataza, C., … & Molyneux, S. (2020). Prolonged health worker strikes in Kenya-perspectives and experiences of frontline health managers and local communities in Kilifi County. International journal for equity in health, 19(1), 1-15. https://doi.org/10.1186/s12939-020-1131-y.
Xu, D., Zhan, J., Cheng, T., Fu, H., & Yip, W. (2022). Understanding online dual practice of public hospital doctors in China: a mixed-methods study. Health Policy and Planning, 37(4), 440-451. https://doi.org/10.1093/heapol/czac017.