Volume 2023,
Article ID 763131,
Journal of Human Resources Management Research,
9 pages,
DOI: https://doi.org/10.5171/2023.763131
Received date: 29 May 2023; Accepted date: 2 August 2023; Published date: 2 October 2023
Academic Editor: Dounia Joualy
Cite this Article as:
Jaafar EL BARDAI and Amina AOMARI (2023)," Planned Behavior and Voluntary Departure: A Qualitative Study of The Public Health Sector in Morocco ‘, Journal of Human Resources Management Research, Vol. 2023 (2023), Article ID 763131, https://doi.org/10.5171/2023.763131
The shortage of human resources is a worldwide phenomenon that affects every organization, impacting on the smooth running and performance of its structures. Health establishments are no exception, and are in turn faced with a growing shortage of the two key players in healthcare systems responsible for the care offered to citizens, namely doctors and nurses. A number of factors linked to the individual and his or her working environment influence the decision of public sector doctors to leave their jobs. With this in mind, and in order to identify the various determinants and factors responsible for the process of voluntary departure, a qualitative study was carried out with several stakeholders and experts in the healthcare sector to anticipate this behavior, which negatively affects the performance of these care structures. Analysis of the study results highlighted a number of important concepts for further study, namely insecurity at work, geographical remoteness and the lack of leadership and management procedures and standards.
Keywords: Intention to leave, theory of planned behavior, JD-R model, work–family conflict.
Introduction
In Morocco, the primordial role played by human resources was solemnly affirmed by His Majesty King Mohamed VI, on the occasion of the 2nd conference on health, inviting all player parties to surround the issue of human resources in this vital sector, while giving it the attention it deserves. To this end, the Kingdom of Morocco has set up a number of initiatives to develop the skills of these resources, in order to help the population realize one of its most fundamental human rights: the right to better healthcare, without discrimination or marginalization. However, like most healthcare systems in the African continent, the Moroccan healthcare system is experiencing a shortage of human resources. The World Health Organization pointed out in its 2014 report that indeed African countries are experiencing a real shortage in terms of resources in the health fields, and that government states must remedy this in order to alleviate the population’s need in this sense. This crisis is worsening over time, and the shortage of healthcare personnel could increase from 7.2 million to 12.9 million by 2035. This is the very purpose of our research, namely to understand the factors responsible for this shortage of human resources, and specifically the factors encouraging the withdrawal of healthcare personnel, in this case doctors.
A number of authors have argued that, in order to explain voluntary departure behavior, or any other behavior, we must first look at the concept notion of the intention to leave, which constitutes a real conceptual framework for predicting organizational withdrawal behavior – a real challenge for any organization.
It is with this in mind that we set out to answer the following question: What factors explain the intention to leave of public-sector doctors in Morocco?
In the course of this research, we will first identify the various concepts and theories mobilized. From the concept notion of voluntary departure (turnover), the basis for explaining the shortage of human resources, to the theory of planned behavior, the JD-R model, and finally, work-family conflict, which will certainly constitute, for all managers and executives, fundamental elements for predicting the departure behavior of different employees. We will also present the results of our qualitative study of various managers and stakeholders in the Moroccan national healthcare system.
Contextual Framework
Morocco’s national healthcare system faces a number of challenges, not least especially those relating to human resources management. One of these obstacles is the shortage of human resources (doctors and nurses), which is one of the major concerns of the Moroccan public health sector. This shortage of human resources has negative effects and consequences on the quality of care provided to the population (George, 1979; Hart and Moore, 1989; Jones, 1990b), reducing both the efficiency and productivity of care delivery (Price and Mueller, 1986).
Thus, the ultimate goal of the Ministry of Health and Welfare is to overcome this major challenge. With this in mind, the Ministry has launched a number of projects to tackle the problem. Among the projects launched are the new framework law 06-22 on the national health system, aimed at reforming the health sector, and the signing of the framework agreement on the implementation of the program to increase the health sector’s workforce by 2030. These fundamental projects will provide a solution to this shortage. It’s true that it’s necessary to implement such actions to overcome the HR shortage problem issue, but above all, it would be wise to understand and provide logical explanations for the behavior of the various doctors who are leaving the civil service, in this case the public health sector. In 2022, 288 doctors in all specialties left the civil service, an alarming figure that only accentuates this crisis.
Theoretical Framework
The set of theories and concepts mobilized in the course of our research, namely turnover, intention to leave, the theory of planned behaviour, the Jobs-demands resources model and finally Work-Family Conflict (WFC).
Voluntary departure and intention to leave
Voluntary departure is a form of turnover. According to Price and Mueller (1986), turnover can be divided into two categories: voluntary and involuntary. Voluntary turnover is when an employee decides to leave the organization. Involuntary turnover, on the other hand, occurs when an employee is forced to leave his or her organization by the employer. The study of this phenomenon has multiplied in view of its consequences. Price and Mueller (1986) assert that staff turnover in healthcare establishments reduces both the efficiency and productivity of care delivery, and increases the cost of labor in running the establishments. This phenomenon can also affect the continuity of care services, thus impacting on the quality and cost-effectiveness of the patient care (George, 1979; Hart and Moore, 1989; Jones, 1990b; Phillips, 1990; O’Brien-Pallas et al., 2006).
The individual who decides to leave his job certainly goes through a process of reflection, based on an evaluation of his behavior and stimulated by an idea and intention that precedes it. It is therefore necessary for leaders and managers to predict and understand this behavior. Intention to leave is in fact considered a “proactive” indicator of voluntary turnover (Hayes et al., 2006).
It is therefore interesting to study and identify this concept as the most obvious means of predicting employee departure behavior. Indeed, according to Ajzen and Fishbein’s theory of reasoned action, an intention refers to “a psychological precursor of any behavioral act” (1975), which explains why the intention to leave is considered a determinant of the decision to leave an organization (Porter and Aymen, 2010). It is the last attitudinal manifestation preceding the act of leaving the organization (O’Neil and Mone 1998). It corresponds to the individual’s estimated probability of leaving his or her job in the near future (Bigliardi et al., 2005), thus considered the essential determinant of voluntary employee departure (Griffeth et al., 2000).
Intention to leave and the theory of planned behavior
A multitude of intention-based explanatory theories of behavior have been developed, largely stemming from social psychology (Godin, 2013). These theories, have emerged with the aim of looking at the behaviors of individuals attempting to conduct an explanation, for example, “why do individuals go to an amusement park or not, why do they practice a sporting activity or don’t they practice a sports activity..?”.
Ajzen’s Theory of Planned Behavior (TCP) (1991) fills in the gaps and enhances the work on the theory of reasoned action. To this end, in addition to attitudes and subjective norms, Ajzen has introduced a new dimension, namely perceived behavioral control.
Attitudes refer to the individual’s degree of evaluation, favorable or unfavorable, of the desired behavior, as well as the plausible consequences of carrying it out (Ajzen, 1991). Subjective or social norms refer to the social influences exerted by the individual’s entourage – friends, family, colleagues – on the performance of the behavior in question (Ajzen, 1991). Finally, perceived control refers to the ease or difficulty of performing the behavior desired by the individual (Ajzen, 1991).
TCP has been adopted in several fields of research to understand the adoption of various behaviors, namely: studies relating to the field of health, the practice of sport (Armitage and Conner, 2001), product consumption (the intention to purchase a car, bags, watches, etc.) (Mannetti et al. 2002). TCP has also been called upon in the IS field, to help understand the use and acceptance of information system tools by users.
As a result, the theory of planned behavior may appear to be a theoretical framework for defining the withdrawal intention of public-sector doctors, as determined by the three factors mentioned above.
Contribution of the Job Demands-Resources model in explaining intention to leave
The JD-R model is based primarily on job characteristics, i.e., demands and resources, with the aim of understanding burnout and disengagement, the consequences of which are of great interest to researchers. A number of studies have demonstrated the need for managers to anticipate the phenomenon of occupational stress and its adverse effects (absenteeism, intention to leave, voluntary departure…) (Elchardus and Cohen, 2002; Firth, Mellor, Moore and Loquet, 2004; Hansez et al., 2005) and to promote commitment to work and its positive effects (performance, well-being, intention to stay…) (Meyer and Allen, 1991; Meyer, Paunonen, Gellatly, Goffin and Jackson, 1989).
Like the two previous models from 2001 and 2004, this model is characterized by the interaction between the two job characteristics, resources and demands. This interaction can lead to the emergence of different scenarios or processes: a first process relating to a state of exhaustion, engendered mainly by poorly designed jobs or high job demands (Bakker and Demerouti, 2007), then a second process which focuses on the development of motivation in the workplace, through the availability of professional resources leading to high commitment to work (Bakker and Demerouti, 2007).
The new JD-R model of 2007 proposes another postulate relating to the interaction between work demands and resources. Thus, it is envisaged that work resources alleviate work stress, or even burnout, engendered by high work demands (Bakker et all., 2003c), thus playing a buffering role (Karasek, 1979).
The JD-R model seems relevant in explaining the intention to leave of doctors in the public sector, in the sense that they are confronted in their work environment with high demands and low professional resources. This imbalance affects doctors negatively, through the emergence of increased professional stress or burnout, as well as feelings of disengagement and demotivation, which can impact on their decision to stay or leave the public sector.
Work-Family Conflict, an indispensable variable in explaining physicians’ intention to leave
Work-family conflict (WFC) has been defined by Netemeyer et al (1996) as the interference caused by general work constraints to the detriment of family-related responsibilities. In other words, WFC refers to an individual’s difficulty in meeting family demands because of work obligations. This variable is indeed relevant in the healthcare sector, as public-sector doctors are confronted on the one hand with the demands and requirements of the profession, and, on the other, must also satisfy marital demands and requirements. This confrontation between roles (professional profession, family) makes it difficult for doctors to satisfy the demands of both fields (Burke and Greenglass, 1987; Greenhaus and Beutell, 1985).
It has been shown that the caregiving professional, in a situation of WFC, can thus face high levels of professional stress, fatigue and depression (Takeuchi and Yamazaki, 2010). WFC can also lead to a more delicate situation, namely burnout (Leineweber et al., 2014b; Wang, Chang, Fu, & Wang, 2012). In addition, various findings have reflected the plausible repercussions of WFC on the health of healthcare professionals (Berkman et al., 2015). However, numerous studies have established the existence of a positive correlation between the WFC and the turnover or voluntary departure of healthcare staff (Grzywacz et al., 2006; Webster, Flint, and Courtney, 2009) – a worrying situation for any national healthcare system.
The World Health Organization affirmed in 2008 that WFC is recognized as one of the major factors in the shortage of human resources. Moreover, according to studies carried out in Germany, Italy and Greece, healthcare professionals in general, and doctors in particular, are the people most likely to face a high risk of WFC.
All the highlighted consequences of work-family conflict seem interesting to study. However, we’re going to focus on occupational stress and burnout on the one hand; two explanatory dimensions of the intention to leave, and of course the direct association of WFC with behaviours of withdrawal from the structure and organization, in this case the intention to leave voluntarily. Similar studies have shown that the WFC has various negative effects on employees’ well-being at work, such as stress and burnout, leading to a decline in health, and consequently higher absenteeism and higher intentions to leave (Amstad et al., 2011).
Methodology
The epistemological position adopted in this study to respond to our problem is critical realism, which combines two approaches, namely positivism and constructivism. Our objective is to conduct a qualitative study, characterized by an iterative process of back and forth between theory and fieldwork, with the aim of understanding the phenomenon of voluntary departure, which is linked to the shortage of human resources. This qualitative study will enable us to draw up our conceptual model and related hypotheses, so that we can test our conceptual model in the field through a quantitative study, the second objective of our epistemological positioning, which will continue in order our research.
The qualitative study relating to the exploratory phase of our research was carried out by interviewing managers in the healthcare sector using interview guides, until semantic saturation was reached (ten interviewees). The sampling technique used was non-random expert sampling. The axes of this guide, which were coded using NVivo12 software, were defined and referred to the challenges facing the national health system in terms of human resources, the impact of these challenges on the performance of this system and the quality of care provided to the population, the determining factors of these challenges, among others, the voluntary departure of doctors from the public sector, and, also, the influence of work-family conflict on the voluntary departure of doctors, and finally the measures undertaken and to be undertaken by the health department to counteract this phenomenon.
Results
NVivo 12 software was used to analyze the content of the various interviews conducted with these managers. The output is presented in the form of clouds and surfaces, enabling us to visualize in a synthetic and global way the elements most cited and raised by the said managers.
Challenges facing the national health system in terms of human resources
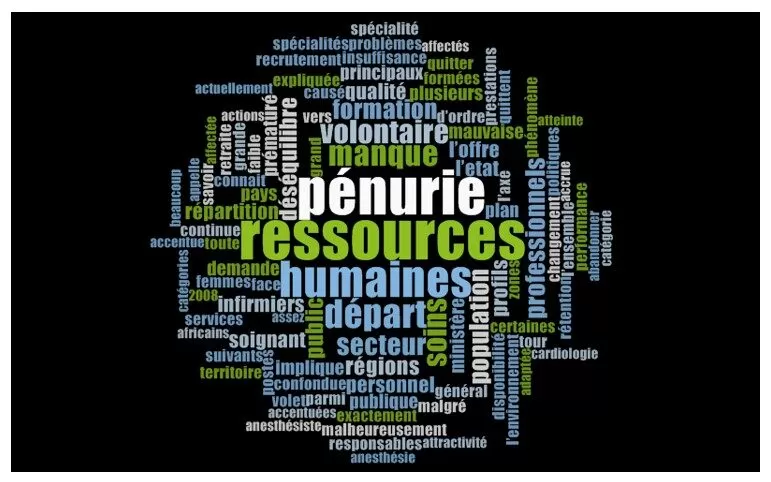
The first analysis provided by NVivo focuses on the human resources challenges faced by the national health system. The results of our analysis of interview guides with Ministry officials corroborated the relevance of our research, supporting the existence of a real shortage of human resources, affecting firstly doctors, then nurses – two key players in any healthcare system. This shortage was essentially explained by the voluntary departure of these health professionals, and the lack of production or training of these profiles.
Fig 1. Nvivo output – SNS challenges
Impact on national health system performance
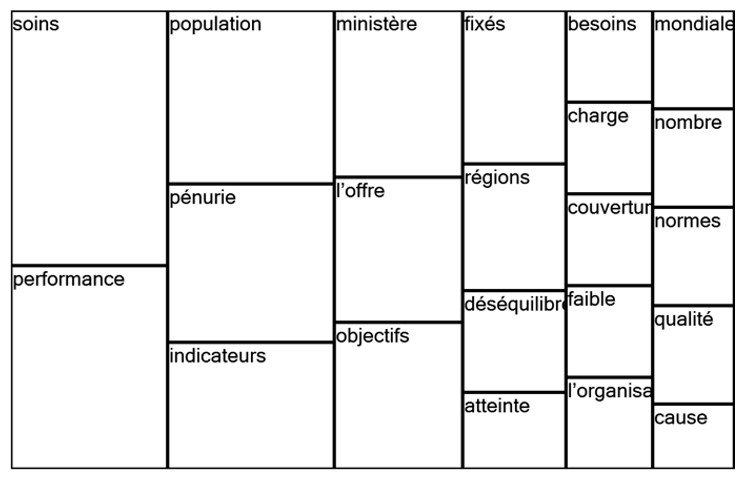
This shortage of doctors certainly affects the performance of healthcare systems. Indeed, all the interviewees affirmed this existential relationship between the shortage of human resources and performance, explained by the difficulty of delivering the care expected by the population, which is reflected in the failure to achieve the objectives and indicators set by the Ministry and health establishments. The result is an imbalance in healthcare provision and coverage between the different regions of Morocco.
Fig 2. Nvivo output – Impact on performance
Determining factors influencing the voluntary departure of doctors from the public sector
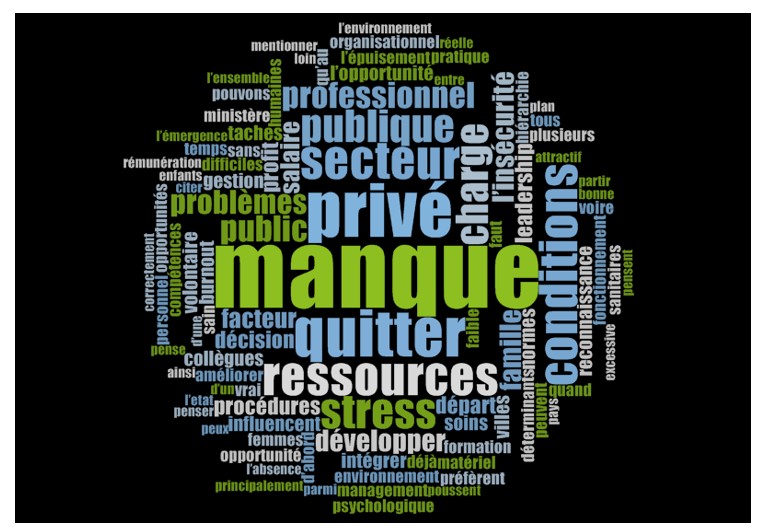
The voluntary departure of doctors from the public sector was explained by a number of factors. The majority of managers pointed to working conditions, which include a lack of resources in the workplace, as well as a workload described as excessive, caused by the shortage of human resources. Stress and burnout were also identified as factors prompting these doctors to leave the public service. In addition to these factors, job insecurity, job risk, violence and harassment at work were identified as dimensions characterizing the Moroccan context, and in particular the health structures where public sector doctors work. Despite the efforts made by the Ministry in terms of salary, i.e., the granting to doctors of the 509 index increasing their salary, most of those interviewed said that this was not enough, compared with the opportunities available in the external environment, i.e., the private sector or European countries or elsewhere.
Other factors brought to light by this analysis, such as the lack of leadership, management procedures and standards, as well as the lack of recognition by the hierarchy; all factors that can reinforce the voluntary departure of these doctors.
Add to this the fact that most of these managers raised the important point that public sector doctors are generally women, and that women are the most likely to be affected by these factor
Fig 3. Nvivo output – Determining factors
Influence of the social environment on the voluntary departure of doctors from the public sector
This figure shows the influence of the social environment on doctors’ decisions to leave or stay in the public sector. Thus, NVivo’s results show the role played mainly by the family, in this case the wife, the husband, the spouse and parents, as well as work friends or former colleagues who have already taken the decision to leave the public sector, encouraging them to seize the opportunities available in the private sector, especially in terms of profits and benefits. Small families can also influence doctors to leave the public sector if they practice and work in areas far from their families.
Fig 4. Nvivo output – Influence of social environment
Influence of the individual’s personal perception and beliefs regarding the voluntary departure behavior of public-sector physicians
As for the following figure, it highlights the role of favorable attitudes towards quitting behavior. These are expressed by the degree of desirability and motivation developed by public sector doctors, while taking into consideration the means and resources available to carry out the desired behavior. Thus, before deciding to leave the public sector, doctors assess the feasibility of the behavior, studying the possible alternatives and opportunities available to them for substituting the public sector.
Fig 5. Nvivo output – Personal perceptions and beliefs
Influence of work-family conflict on the voluntary departure of physicians from the public sector
The results of the NVivo analysis concerning the role played by work-family conflict in doctors’ decisions to leave or stay in the public sector are interesting. In the sense that the majority of interviewees linked this dimension to a recurring problem that affects the majority of Moroccan doctors in the public sector, and frequently women. This is none other than the place of assignment and work in remote areas; geographically far from their families’ place of residence. In other words, this survey established the existence of a link between the WFC and the geographical distance between the workplace and the family’s place of residence. This is explained by the fact that doctors who are far away from their families cannot ensure or fulfill their family or marital duties, which can lead to marital problems, violence and even divorce, especially when there are children and parents to be taken care of.
Fig 6. Nvivo output – Influence of WFC
Interpretation of the NVivo software results consolidated and affirmed the importance of the variables identified in the theory. In addition, these results enabled us to bring out new elements and variables, taken into consideration for the elaboration of our conceptual model and research hypotheses. We refer, for example, to work-related occupational risks and to the distance or proximity between doctors’ workplaces and their families’ home towns. This variable was mainly correlated with work-family conflict.
This study also highlighted the importance of studying the gender of doctors in our quantitative phase. It turns out that women make up the majority of doctors in the healthcare sector. They are the most likely to be affected by the variables studied, thus influencing their decision to leave or remain in the public sector.
Conclusion
The human dimension is recognized as one of the most important key components of success, but also as one of the main causes of failure (Kotter and Cohen, 2002; Bareil, 2004). It is therefore essential for any structure or organization to focus its attention on the human factor, more specifically, to improve the retention of human resources and counteract the phenomenon of voluntary departure or withdrawal of personnel. This challenge is particularly acute in the healthcare sector. A healthcare system that has difficulty retaining its human resources loses performance, and this has a direct impact on the health of its citizens.
The voluntary departure of the Moroccan medical corps is a major challenge for officials at the Ministry of Health and Social Protection, despite the various human resources development projects launched by this department. It is therefore important to understand why Moroccan doctors are leaving the public sector (civil service) for better opportunities. To this end, and in order to anticipate this behavior, which is detrimental to the performance and smooth running of health establishments, it is necessary to anticipate it and study its motivational factors, through the study of behavioral intention, characterized as the primary predictor of any behavior performed.
Thus, the main aim of this research was to study and list, in a non-exhaustive way, the different determinants and factors that can influence Moroccan doctors’ intention to leave. On the one hand, sociological determinants, through the integration of the theory of planned behavior, and, on the other, the study of organizational elements; the interaction of work demands and resources, through the mobilization of the Job-demands resources theory.
From the above, the conceptual model seems rich, and could be improved by integrating other constructs and variables already mobilized in other studies that influence the intention to leave, to finally have an exhaustive conceptual model adapted to the Moroccan context, and finally propose plausible solutions to overcome this phenomenon linked to the voluntary departure of Moroccan doctors.
Bibliography
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In Action control(pp. 11-39). Springer, Berlin, Heidelberg.
Ajzen, I. (1991). The theory of planned behavior. Organizational behavior and human decision processes, 50(2), 179-211.
Amstad, F. T., Meier, L. L., Fasel, U., Elfering, A., & Semmer, N. K. (2011). A meta-analysis of work–family conflict and various outcomes with a special emphasis on cross-domain versus matching-domain relations. Journal of occupational health psychology, 16(2), 151.
Armitage, C. J., & Conner, M. (2001). Efficacy of the theory of planned behaviour: A meta‐analytic review. British journal of social psychology, 40(4), 471-499.
Bakker, A. B., & Demerouti, E. (2007). The job demands‐resources model: State of the art. Journal of managerial psychology, 22(3), 309-328.
Bakker, A.B., Demerouti, E. & Schaufeli, W.B. Dual processes at work in a call centre: An application of the Job Demands–Resources model. European Journal of Work and Organizational Psychology,2003c,12, 393–417.
Berkman, L. F., Liu, S. Y., Hammer, L., Moen, P., Klein, L. C., Kelly, E., … & Buxton, O. M. (2015). Work–family conflict, cardiometabolic risk, and sleep duration in nursing employees. Journal of occupational health psychology, 20(4), 420.
Bigliardi, B., Petroni, A., & Dormio, A. I. (2005). Organizational socialization, career aspirations and turnover intentions among design engineers. Leadership & organization development journal, 26(6), 424-441.
Burke, R. J., & Greenglass, E. R. (1987). Work and family.
Elchardus, M. et Cohen J. (2002). Attitude et attentes en rapport avec la fin de carrière professionnelle. Rapport partiel 2 : Le cours de la vie et transition vers la pension en Belgique, Groupe d’études TOR, VUB.
Firth, L., Mellor, D. J., Moore, K. A., & Loquet, C. (2004). How can managers reduce employee intention to quit?. Journal of managerial psychology, 19(2), 170-187.
Fishbein, M., Ajzen, I., & Belief, A. (1975). Intention and Behavior: An introduction to theory and research.
George, D. L. (1979). … a shortage of nurses who will work… AJN The American Journal of Nursing, 79(5), 878-879.
Greenhaus, J. H., & Beutell, N. J. (1985). Sources of conflict between work and family roles. Academy of management review, 10(1), 76-88.
Griffeth, R. W., Hom, P. W., & Gaertner, S. (2000). A meta-analysis of antecedents and correlates of employee turnover: Update, moderator tests, and research implications for the next millennium. Journal of management, 26(3), 463-488.
Grzywacz, J. G., Frone, M. R., Brewer, C. S., & Kovner, C. T. (2006). Quantifying work–family conflict among registered nurses. Research in nursing & health, 29(5), 414-426.
Godin, G. (2013). Les comportements dans le domaine de la santé. Les presses de l’Université de Montréal.
Hansez, I., Bertrand, F., De Keyser, V., & Perée, F. (2005). Fin de carrière des enseignants: vers une explication du stress et des retraites prématurées. Le travail humain, 68(3), 193-223.
Hart, S. K., & Moore, M. N. (1989). The relationship among organizational climate variables and nurse stability in critical care units. Journal of Professional Nursing, 5(3), 124-131.
Hayes, L. J., O’Brien-Pallas, L., Duffield, C., Shamian, J., Buchan, J., Hughes, F., … & Stone, P. W. (2006). Nurse turnover: a literature review. International journal of nursing studies, 43(2), 237-263.
Jones, R. C. (1990). Technical personnel shortages in construction industry. Journal of professional issues in engineering, 116(1), 16-26.
Karasek Jr, R. A. (1979). Job demands, job decision latitude, and mental strain: Implications for job redesign. Administrative science quarterly, 285-308
Leineweber, C., Westerlund, H., Chungkham, H. S., Lindqvist, R., Runesdotter, S., & Tishelman, C. (2014). Nurses’ practice environment and work-family conflict in relation to burn out: a multilevel modelling approach. PLoS One, 9(5), e96991.
Mannetti, L., Pierro, A., & Livi, S. (2002). Explaining Consumer Conduct: From Planned to Self‐Expressive Behavior 1. Journal of Applied Social Psychology, 32(7), 1431-1451.
Meyer, J. P., Paunonen, S. V., Gellatly, I. R., Goffin, R. D., & Jackson, D. N. (1989). Organizational commitment and job performance: It’s the nature of the commitment that counts. Journal of applied Psychology, 74(1), 152.
Meyer, J. P., & Allen, N. J. (1991). A three-component conceptualization of organizational commitment. Human resource management review, 1(1), 61-89.
Netemeyer, R. G., Boles, J. S., & McMurrian, R. (1996). Development and validation of work–family conflict and family–work conflict scales. Journal of applied psychology, 81(4), 400.
O’Brien-Pallas, L., Griffin, P., Shamian, J., Buchan, J., Duffield, C., Hughes, F., … & Stone, P. W. (2006). The impact of nurse turnover on patient, nurse, and system outcomes: a pilot study and focus for a multicenter international study. Policy, Politics, & Nursing Practice, 7(3), 169-179.
O’Neill, B. S., & Mone, M. A. (1998). Investigating equity sensitivity as a moderator of relations between self-efficacy and workplace attitudes. Journal of Applied Psychology, 83(5), 805.
Phillips, J. D. (1990). The price tag on turnover. Personnel Journal, 69(12), 58-61.
Porter, S., & Ayman, R. (2010). Work flexibility as a mediator of the relationship between work–family conflict and intention to quit. Journal of Management & Organization, 16(3), 411-424.
Price, J. L., & Mueller, C. W. (1986). Absenteeism and turnover of hospital employees. JAI press.
Takeuchi, T., & Yamazaki, Y. (2010). Relationship between work–family conflict and a sense of coherence among Japanese registered nurses. Japan Journal of Nursing Science, 7(2), 158-168.
Wang, Y., Chang, Y., Fu, J., & Wang, L. (2012). Work-family conflict and burnout among Chinese female nurses: the mediating effect of psychological capital. BMC public health, 12(1), 1-8.
Webster, J., Flint, A., & Courtney, M. (2009). A new practice environment measure based on the reality and experiences of nurses working lives. Journal of Nursing Management, 17(1), 38-48.