Received date: 8 September 2013; Accepted date: 30 October 2013; Published date: 22 November 2013
Academic Editor: Kyoung Ho Park
Cite this Article as:
Fumiyuki Goto, Tomoko Tsutusmi, Kaoru Ogawa and Masaru Mimura (2013), " The Effect of two Different Selective Serotonin Reuptake Inhibitors in Patients with Chronic Tinnitus", JMED Research, Vol. 2013 (2013), Article ID 995972, DOI: 10.5171/2013. 995972
Objective: Serotonin selective re-uptake inhibitors (SSRI) are well-known antidepressants. There has been no report on the different benefits that different SSRIs may confer on tinnitus patients. We conducted a retrospective chart review comparison study of the clinical effect of 2 different SSRIs (paroxetine, fluvoxamine) on tinnitus patients. Methods:Fluvoxamine was prescribed to 26 cases (defined as group F), and paroxetine to 33 patients (defined as group P). We evaluated depression and tinnitus severity with questionnaires. We evaluated the clinical effect with the Clinical Global Impression-Improvement scale (CGI-I). Results: The imipramine equivalence of the prescribed paroxetine was 92.6 ± 24.5 and that for fluvoxamine was 81.4 ± 29.3.We determined no statistical difference in each value between the groups. There was statically significant deference in THI before and after the treatment in both group P (P<0.05) and group F (P<0.05). The CGI-I scale scores were 2.5 ± 1.3, and 2.9 ± 1.2 for group F and group P, respectively. Both SSRIs were equally effective to the patients with tinnitus. The CGI-I scale and initial THI were correlated only in paroxetine-treated patients (R = -0.60, P < 0.05). Conclusions: Fluvoxamine and paroxetine affect tinnitus patients differently due to their differing pharmacological effects.
Tinnitus is a relatively non-specific symptom of several disorders. Tinnitus is known as one of the somatic symptoms of depression (Folmer and Shi, 2004), whereas most patients with tinnitus are neither depressed nor seriously bothered by their tinnitus (Dobie, 2003). Tinnitus may result from very different pathological states. There are subjective and objective forms. While objective tinnitus results from sounds in the body, subjective tinnitus results from abnormal neural activities, which are not formed by sounds(Belli et al., 2012).The patients who complain bitterly of tinnitus are often found to have a major depressive disorder. It has been reported that antidepressants benefit the treatment of tinnitus. Indeed, antidepressants are sometimes prescribed for tinnitus (Robinson, 2007). There is no indication that one specific type of antidepressant is more likely to have a beneficial effect on tinnitus than another (Robinson, 2007).
The aim of the present study was to assess a retrospective comparison of the clinical and adverse effects of 2 different SSRIs (paroxetine, fluvoxamine) on patients with tinnitus.
Methods
The subjects were patients with chronic tinnitus persisting for more than 3 months who visited our hospital (Hino Municipal Hospital) from 2003 to 2008 and were intractable to conventional therapy. All tinnitus was not objective but subjective. We carried out initial evaluation that included pure tone audiometry and magnetic resonance imaging. After these evaluations, we explained the possible mechanisms of tinnitus and treatment strategy to the patients. Then, conventional pharmacological therapy with vitamin B12 was continued for 4 weeks. If we observed no improvement, we prescribed an SSRI after receiving informed consent. Fluvoxamine was prescribed to 26 cases (defined as group F), and paroxetine to 33 patients (defined as group P). 5 patients in group F and 8 patients in group P could not continue the treatment. We evaluated tinnitus distress with the Tinnitus Handicap Inventory (THI) and measured depression with the Self-Rating Depression Scale (SDS). Zung (1965) developed the SDS (Zung et al., 1983, Zung, 1965) (Goto et al., 2012). We instructed the patients to visit our department every 2 weeks for observation and prescription. We prescribed the minimum doses of all of these drugs and increased them to the relevant doses if we observed no adverse reaction. We initiated fluvoxamine from the minimum 50-mg dose, and increased it to the maximum dosage of 100 mg if there were neither side nor adverse effects. We started with paroxetine doses of 10 mg, and increased dosages to the maximum 20 mg if we observed neither side nor adverse effects. After 6 weeks, we used the Clinical Global Impression-Improvement scale (CGI-I) (Guy, 1976) (Goto et al., 2012), and THI to carry out the final evaluation. The CGI-I scale was graded as follows: 1, very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; and 7, very much worse. We performed statistical analysis with an unpaired t-test using GraphPad Prism 3 (GraphPad Software, Inc., CA, USA). We considered results statistically significant if the P value was less than 0.05. We also calculated the correlation coefficient. The study was carried out in accordance with the guidelines of the ethics committee of the Hino Municipal Hospital and the Declaration of Helsinki.
Results
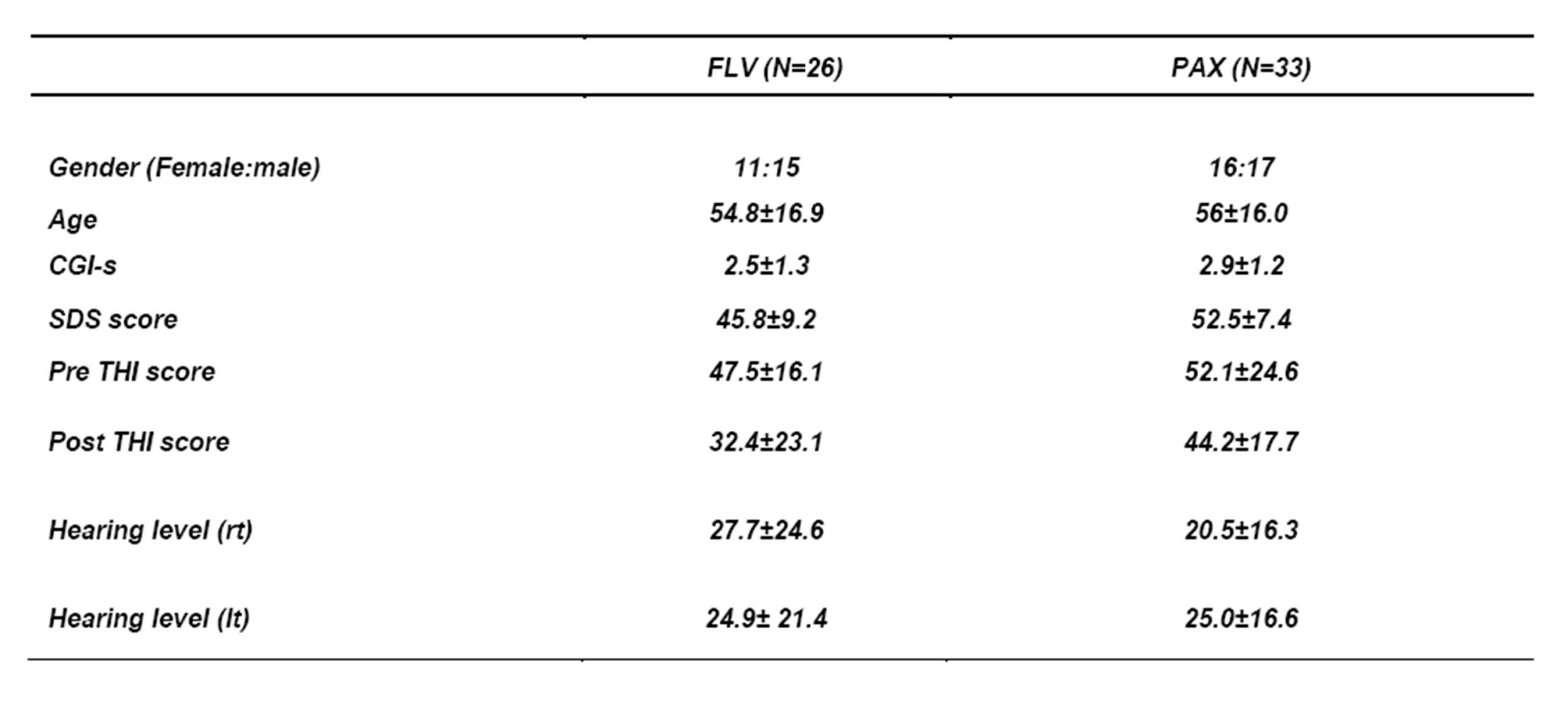
We have listed the subjects’ profiles and the overall effect of SSRIs as evaluated by the CGI-I scale in Table 1. We determined no statistical difference in each value between the groups. There was statically significant deference in THI before and after the treatment in both group P (P<0.05) and group F (P<0.05). There was no relation between the THI and CGI-I scores in group F, but the scores were related in group P (R = -0.60 P < 0.05). We found no correlation between the SDS score and clinical effect measured by the CGI-I scale in groups F or P. We observed adverse reactions in 15.4% (4/26) of group F. These were nausea (N = 1), drowsiness (N = 1), dizziness (N = 1), and numbness (N = 1). We observed adverse reactions in 21.2% (7/33) of group P, which included nausea (N = 4), drowsiness (N = 1), constipation (N = 1), and heart palpitations (N = 1). The imipramine equivalence of the prescribed paroxetine was 92.6 ± 24.5 and that for fluvoxamine was 81.4 ± 29.3.
Discussion
The CGI-I scale measured better improvement in patients with high THI scores only in group P. It is reasonable to assume that paroxetine had alleviated suffering that was itself due to tinnitus.
We would explain the observed different effects between paroxetine and fluvoxamine by some of the pharmacological differences of these drugs. The difference between groups P and F is the intensity of serotonin reuptake. An in vitro study indicated that paroxetine is stronger and more selectively reuptaking serotonin(Thomas et al., 1987) (Salvi et al., 2009). The paroxetine was effective in treating tinnitus patients with depression and anxiety by reducing their tinnitus severity as well as their depression and anxiety (Oishi et al., 2010) as reported before. Basic research has reported the possibility that rostral serotonergic neurons contribute to changes in neural function during tinnitus (Caperton and Thompson, 2010). SSRIs may have an effect on this site and have beneficial effects on tinnitus.
The other difference between these 2 drugs is their action on the sigma-1 receptors. There is a novel role for sigma-1 receptors in the active mechanisms of fluvoxamine(Hashimoto, 2009). Sigma-1 receptors can modulate cognitive function. The fluvoxamine was effective in treating tinnitus patients to help improve cognitive outcomes in patients (Hindmarch and Hashimoto, 2010) as reported before.
The other possibility is that serotonin transporter promoter polymorphism might exist and may confound clinical results. It is known that the 5-HTT gene—linked polymorphic region (5-HTTLPR) genotype is related to clinical responses to paroxetine and fluvoxamine. We could not control the patients in our study completely, and there may have been differences in the 5-HTTLPR genotype in the patients. These possible gene differences could have confounded our results.
Paroxetine is more effective in tinnitus patients with high THI scores. Conversely, we observed no similar trend in patients treated with fluvoxamine. We conclude that fluvoxamine and paroxetine have different effects on patients with tinnitus due to their different pharmacological qualities. Further double-blind controlled studies will be required to confirm these differences.
Table1 Subjects and results
Acknowledgements
This research was supported in part by The Yuumi Memorial Foundation for Home Health Care 2010.
FOLMER, R. L. & SHI, Y. B. (2004) SSRI use by tinnitus patients: interactions between depression and tinnitus severity. Ear Nose Throat J, 83, 107-8, 110, 112 passim.
GUY, W. (1976) CGI Clinical Global Impressions. IN ROCKVILLE, M. (Ed.) EC-DEU Assessment Manual for Psychopharmacology, Revised. U.S. Department of Health, Education, and Welfare