Received date: 6 November 2013; Accepted date: 13 January 2014; Published date: 28 June 2014
Academic Editor: Niki John Agnantis
Cite this Article as:
Faisham W. Ismail, Ng Thong Pin, M. Z. Nor Azman, Zulmi Wan, M. D. Salzihan and Mutum S. Samarendra (2014), "p53 Expression Immuno-histochemistry Index in Stage III Giant Cell Tumor of the Bone," JMED Research, Vol. 2014 (2014), Article ID 675393, DOI: 10.5171/2014.675393
We analyzed the p53 expression of 50 consecutive cases of stage III giant cell tumor to determine the clinico-pathological correlation. There were 29 male patients compared to 21 females. The mean age was 36.42 years and ranged from 19 to 66 years. Tumors were located mainly around the knee (48%) followed by distal radius (28%). Sixteen percent (16%) had local recurrence, and twenty four percent (24%) presented with or eventually developed lung metastasis. There were 3 patients who had both local recurrence and pulmonary metastasis. The expression of p53 antigen was evaluated by immuno-histochemical staining techniques, using the avidin-biotin perioxidase complex method, using an LSAB2 kit (Dako, Glostrup, Denmark). The scoring was done by counting the positively stained cell in the background of 1000 mononuclear stromal cells. Data was analyzed using PASW version 18.0. The mean value of p53 index obtained as a percentage of 1000 background cells was 37.68 (ranged 1.00 — 20.0), with standard deviation of 28.33. The p53 index of recurrent tumor was 65.38 compared to 32.42 of those without recurrence, and was statistically significant (mean difference of 32.97 with p value in independent t test of 0.002). The p53 index was also statistically significant in the presence of pulmonary metastases with the mean value of 66.92 compared to 28.45 of those without metastasis (mean difference of 38.47 with p value in independent t test of 0.001). In conclusion, p53 expression is a good prognostic marker to predict the risk of local recurrence and lung metastasis in the giant cell tumor of the bone.
Keywords: p53, staged III, giant cell tumor of the bone.
Introduction
Giant cell tumor (GCT) of the bone is an infrequent and unpredictable bony lesion [Faisham WI et.al 2003]. Although numerous attempts have been made to predict the clinical behavior of GCT, there are no definite biological or histological parameters to determine the prognosis or aggressiveness of this lesion [Gupta R et. al 2008 & Faisham WI et. al 2010]. Aggressive lesions (stage III Campanacci) are common among the oriental population, and the GCTs within this population have been found to have higher risk of recurrence and pulmonary metastasis, compared to those occurred in Caucasian population [Faisham WI 2006, Lim YW 2005, Sung HW 1982 & Takeuchi A 2011].
p53 or protein 53 is a tumor suppressor protein that is encoded by the TP53 gene located on the short arm of chromosome 17p13.1. p53 regulates the cell cycle and acts as tumor suppressor where it helps to conserve stability by preventing genome mutation. p53 has strong impact on survival and predicted risk of local recurrence and pulmonary metastases in a majority of malignant tumors [Soussi T 2007 & Wadayama B 1993]. p53 was shown to correlate with the biological behavior and risk of pulmonary metastases in a few reported cases of GCT of the bone [Papanastassiou I 2010, Wu Y 1997 & Masui F 1998]. However, there are no reported studies to identify the effectiveness of this marker in correlation with the aggressiveness and prognosis of the disease.
The aim of this study is to identify the effectiveness of p53 as a prognostic marker and in predicting the risk of local recurrence and pulmonary metastases in the aggressive (stage III) GCT of the bone. Material and Method
Fifty (50) consecutive patients with histologically proven giant cell tumor, seen at our institution between January 1999 and December 2010, were included. The clinical and radiological records of all the patients were reviewed. Tissue diagnosis and immuno-histopathological study was obtained in all cases from the surgical specimens. Stage III or aggressive GCT in this study is defined as symptomatic, rapidly growing extraosseus lesion [Campanacci M et. al. 1987]. Bone scans showed intense activity that often extended beyond the lytic area on radiograph, and magnetic resonance imaging (MRI) showed tumor infiltration of the surrounding soft tissue, which was confirmed histologically by tumor that has breached the cortex and extended into the surrounding soft tissue.
There were 29 male patients compared to 21 females. The mean age was 36.42 years and ranged from 19 to 66 years. Tumors located mainly around the knee 24 cases (48%), followed by distal radius 8 cases (16%), and sacrum 4 cases (8%). All cases were stage III based on Campanacci staging system. 37 cases were treated with resection and reconstruction and 9 cases were treated with intra-lesional surgery. There were 2 patients who underwent amputation — one above knee amputation due to extensive proximal tibia tumor with vessel involvement and another one Ray’s amputation of metacarpal. Sixteen percent (8 cases) had local recurrence. 6 cases were treated initially with intra-lesional surgery, and subsequently underwent wide resection margin and were free of disease. 2 patients who underwent wide resection had soft tissue recurrence, had wide resection of the recurrence and subsequently were tumor free. 24% presented with or eventually developed lung metastasis. There were 3 patients who had both local recurrence and pulmonary metastasis. Evaluation of p53 Immuno-histochemical Expression
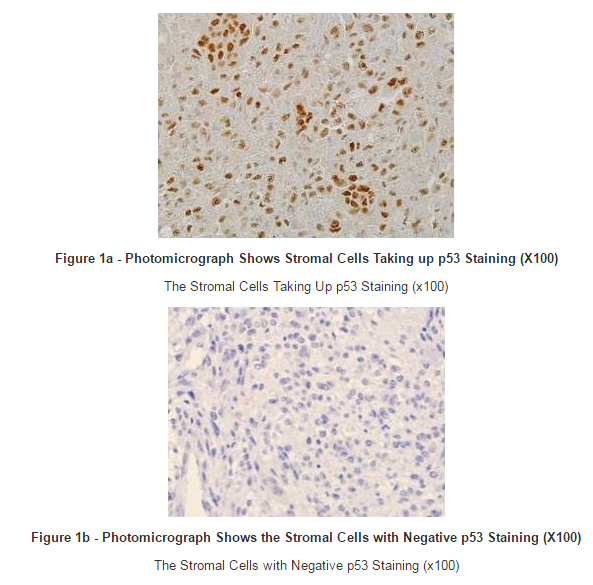
The expression of p53 antigens was evaluated by immuno-histochemical staining in all representative sections from each patient. Serial sections, 5 mm thick, were cut and immuno-histochemical techniques were carried out using the avidin-biotin perioxidase complex method using an LSAB2 kit (Dako, Glostrup, DenmarkR). The primary antibody used in this study was p53 (M3629Clone 318-6-11, dilution 1:25; Dako). The expression of p53 in the nuclear area of the tumor cells was evaluated microscopically from 1000 tumor cells. The labeled-cell count of p53 was determined in ten high-power fields at 400 magnifications by two blinded independent observers. (Figure 1a, 1b). Data was analyzed using PASW version 18.0
Result
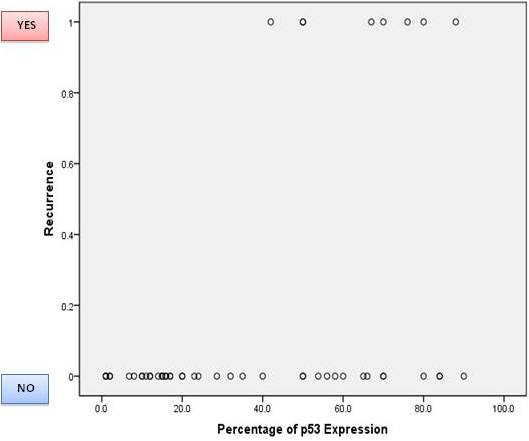
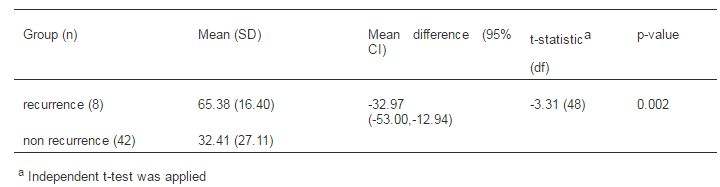
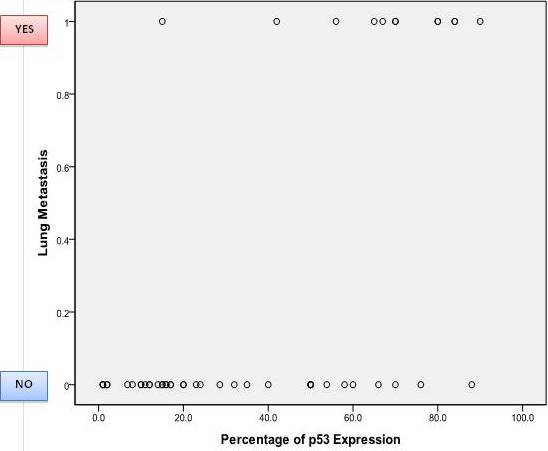
The mean value of p53 index obtained as a percentage of 1000 background cells was 37.68 (ranged 1.00 — 90.0), with a standard deviation of 28.33. The p53 index of recurrent tumor was 65.38 compared to 32.42 without recurrence, and was statistically significant (mean difference of 32.97 with p value in independent t test of 0.002). The p53 index was also statistically significant in the presence of pulmonary metastases with the mean value of metastases group of 66.92, compared to 28.45 without metastases (mean difference of 38.47 with p value in independent t test of 0.001). (Figure 2,3)
Figure 2: a) Scatter Plot Graph of Percentage p53 Expression with Recurrence and Non-Recurrence Cases. b) Comparison Mean of p53 Expression with Independent T-Test.
Scatter plot of Percentage of p53 Expression with non- recurrence and with recurrence cases
Comparison of Mean Percentage of p53 Expression between Recurrence and Non Recurrence Groups (n=50)
Figure 3: a) Scatter Plot Graph of Percentage p53 Expression with Lung Metastases and Non-Metastases Cases. b) Comparison Mean of p53 Expression with Independent T-Test
Scatter plot of Percentage of p53 Expression with lung Metastases and without Metastases
Comparison of Mean Percentage of p53 Expression between Lung Metastases and Non Metastases Groups (n=50)
Discussion
p53 is a tumor suppressor gene that senses and repairs DNA defects in cell cycle. The p53 protein acts to protect cells against the accumulation of mutations and subsequent conversion to a cancerous state. Failure of this mechanism increases the risk of malignant transformation and tumorigenesis. The cells that lack p53 have lost cell cycle control and presumably accumulate damage-induced mutations that result in tumorigenesis [Soussi T 2007 & Wadayama B 1993]. p53 alterations had contributed to tumor progression in bone tumors.
There are many studies done in finding the best parameters in attempts to predict the clinical outcome of the GCT [Gamberi G et. al. 2003]. However, most of the published studies had grouped the cases into one overall stage, while the fact is GCTs are variable in their clinical behavior. We had performed an earlier study on 31 cases of staged III GCT and quantified the value of Ki-67 index. The mean value of Ki-67 index was found to be statistically not significant when tested against the risk of pulmonary metastases and recurrence disease. This implies that the proliferative marker Ki-67 may not be useful to predict the risk for tumor recurrent or lung metastases [Faisham WI et. al. 2010]. Identification of p53 mutation had been suggested to diagnose potential malignant transformation of giant cell tumor [Saito T et. al. 2011]. p53 protein content and gene mutation also play an important role in the development of the neoplasm in the giant cell tumors of the bone [Wu Y et. al. 1997]. Recent study in the literature claimed that, the over expression of p53 had a correlation with lung metastasis and local recurrence in GCT of the bone [Papanastassiou I et. al 2010]. Recently, the overexpression of RANK (Receptor activator of nuclear factor kappa-B) and RANKL (Receptor activator of nuclear factor kappa-B ligand) has been observed in the GCT of the bone. It is found that the overexpression of RANKL by tumor stromal cells could be responsible for the formation of numerous osteoclasts within the tumor [Won KY et. al. 2011 & Roux S 2010].
In this study, we were able to quantify the value of p53 expression in order to achieve stronger evidence of correlation with lung metastasis and local recurrence. We found a statistically significant difference of p53 expression between lung metastasis and non-lung metastasis groups. There was also a significant difference in recurrent and non-recurrent group, statistically where the mean of p53 expression was higher in the recurrence group (p<0.005). The risk of local recurrences is multifactorial, the tumor grade, surgical margin and type of adjuvant treatment following curettage are few commonest caused correlates with this [Gupta R et. al 2008 & Lim YW 2005]. Our initial series on 20 patients had shown that despite aggressive wide margin surgery, local recurrence occurred in two patients. In our study, p53 had shown significant association to predict the recurrent [Faisham et.al WI 2006]. These results with bigger number and specifically in aggressive lesion strongly added weight to the previous studies done by other researchers [Papanastassiou I et. al 2010, Masui F et. al 1998]. Conclusion
In conclusion, p53 expression is a good prognostic marker to predict the risk of local recurrence and lung metastasis in giant cell tumor of the bone.