1Preventive Dentistry Research Center, Research Institute of Dental Sciences, Community Oral Health Department, Dental School, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Hamadan University of Medical Sciences, Hamadan, Iran
3The international Branch of Shahid Beheshti Medical University, Tehran, Iran
Received date: 4 December 2013; Accepted date: 15 April 2014; Published date: 27 May 2014
Academic Editor: Georgios E. Kallergis
Cite this Article as:
Arezoo Ebn Ahmady, Shabnam Seyedzadeh Sabounchi, Hoori Mirmohammadsadeghi and Angelayalda Rezaei (2014), "A Suitable Model for Breaking Bad News: Review of Recommendations," JMED Research, Vol. 2014 (2014), Article ID 776618, DOI: 10.5171/2014.776618
Most physicians experience difficulty when required to deliver bad news. Therefore, recommendations for facilitating breaking bad news were reviewed and a suitable model was described in this study. We performed a search with keywords “breaking bad news”, “strategy”, “protocol”, “guideline” and “model” as the primary descriptors, and limiting the sources to English language articles with abstracts and guidelines, published since 1961 to March 2013. Two trained authors independently reviewed titles, abstracts and full texts of articles after a pilot inter-rater reliability assessment. All articles dealing specifically with breaking bad news were examined; they were descriptive and analytical studies. Recommendations and best models for facilitating breaking bad news from these articles were explored; sorted into discrete categories, summarized and framed as the best model for breaking bad news. The latest models, tools, steps and recommendations (e.g., delivering the bad news at a suitable and calm environment, giving the news with empathy and …) were examined. Although many articles have discussed the topic of breaking bad news, those that occurred repeatedly throughout these articles were summarized. Finally, the reference steps as according to the most important models for breaking bad news were presented. It is suggested that for more effective investigations, studies regarding interactional approaches in patients—medical team relationships be conducted on breaking bad news interventions.
Keywords: Breaking bad news, protocol and guideline.
Introduction
Successful communication is an absolute need at every stage in clinical interview that cannot be overlooked. Evidence shows that healthcare fails without having a conscious informed effort of communication, which is the personal and professional responsibility of everyone concerned with the care of the patient (Kumar et al, 2005). The average medical interviews that a primary care physician will perform during a 40-year career are at least two million; although health care delivery system changes should be taken into account (Epstein et al, 1993).
Effective communication is the basis of mutual understanding and trust, and also malpractice claims are often related to miscommunication between doctors and patients (Epstein et al, 1993). Furthermore, optimal communication has been recognized by patients and their families as one of the most important aspects of medical care at the end of life and breaking bad news situations (Parker et al, 2007; Steinhauser et al, 2001; Wenrich et al, 2001).
Bad news can be categorized in the range of the need to undergo further laboratory or radiological tests to confirm a trivial diagnosis up to inform the patient of a life-threatening disease, such as cancer or informing the family or friends of death or disastrous morbidity of their patient (Salem et al, 2013). Many clinicians have difficulty, or lack the necessary skills in providing this type of care (Amiel et al, 2006; Dosanj et al, 2001). According to the findings from the studies assessing, interactions between patients and clinicians imply that the consequences of breaking bad news poorly can affect both the patient and the doctor involved (Baile et al, 2000; Stiefel et al, 2010; Walsh et al, 1998). Stress related to these incidents can add to burn-out, lack of job satisfaction and anxiety in doctors (Ramirez et al, 1995; Stiefel et al, 2010; Brown et al, 2009). For the patient, poorly communicated bad news can also increase their stress and anxiety, poorly adjust them to the bad news and result in poorer health outcomes (Baile et al, 2000; VandeKieft et al, 2001; Lobb et al, 1999).
Patients claim that physicians do not listen well; much has been written lately on the importance of listening to the patients’ stories. Often, these stories reveal the facts of pain that could never be exposed by the technological marvels of the laboratory and radiology departments. It is not only the stories themselves that are so revealing, but the way these stories are told (Engel, 1977; Reames et al, 1989; Shapiro et al, 1989; Epstein et al, 1993; Walker et al, 1995: Silverman et al, 2005).
So, there seems to be a wide consensus as to the importance of learning communication skills in the different stages of medical education (Meyer et al, 1997). However, education on delivering bad news effectively is dependent on the reliable and firm base of evidence (Paul et al. 2009). Considerable amount of education and research information now exist regarding breaking bad news. (Faulkner, 1998; Hawken, 2005; Abel et al, 2001 Back et al, 2007). Many reports deal with the impact that bad news has on the deliverers (Brown et al, 2009) and the recipients (Amiel et al, 2006), and others contain useful guidelines and recommendations about what to do and say (Baile et al, 2000; Barnett, 2004; Buckman, 1992; Hawken, 2005). Therefore, in this study recommendations for facilitating breaking bad news were reviewed, and a suitable model was described for deliverers of bad news.
Methods
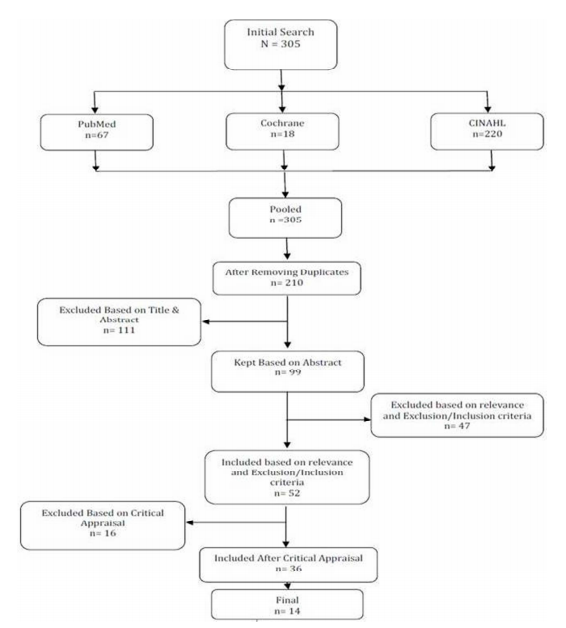
Articles included in this review were obtained through a search in MEDLINE, CINAHL; Cochrane library using the index terms “breaking bad news”, “strategy”, “protocol”, “guideline” and “model” and our initial search was limited to English language articles published from 1961 to March 2013 with abstract. A manual search of the references of identified papers was also performed to include any further applicable literature. This procedure resulted in more than 200 references (Figure 1). Retrieved articles were reviewed separately by two trained and calibrated authors. In order to reach reliability, a pilot inter-rater reliability assessment was conducted, and the inter-rater reliability was 80%. We also excluded articles from consideration which were on topics other than patients and medical team transactions and models for breaking bad news. No limitation was conducted on the study design or type of study included in systematic reviews. Studies which had key terms in the title, abstract, article or MeSH heading were retained. Inclusion criteria were for studies dealing with medical team delivering bad news to patients and their relatives. Such as all healthcare provider types (e.g. physicians, counselors, students and nurses) were included.
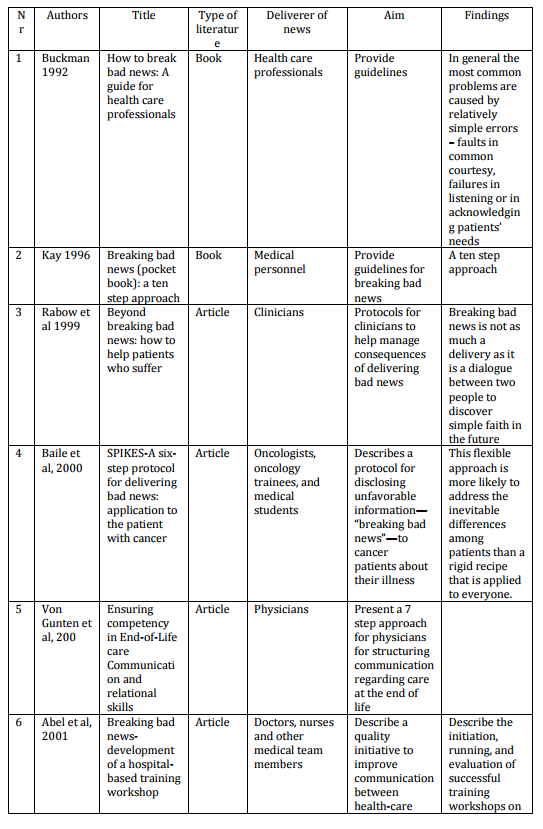
After critically appraising the 52 included articles, only 36 studies were left for consideration. We examined and sorted the final 36 studies, but only studies making recommendations, suggestions or providing guidelines on delivering or communicating bad news were included; so that only 14 sources were inserted to the literature table (Table 1). Although, recommendations were diverse, we summarized those that were repeated across the articles. Recommendations about how best to deliver bad news were relatively dependant on disease type (medical condition) or psychological status of the patient or family. However, general and usual similar conditions were taken into account when categorizing the recommendations according to studies.
Results
This search resulted in 305 titles of articles; of which after removing duplicates, 210 articles remained. Out of remaining articles, 111 were excluded based on title and abstract, and 99 remained. However, 52 articles were included based on exclusion/inclusion criteria, and 36 were finally entered after critical appraisal (Fig 1). Then, again only 14 studies had directly mentioned or recommended protocol, steps or guideline for delivering bad news.
Figure 1: Search and Selection Results
All 14 studies have been demonstrated in Table 1. Among these final studies, six main models or protocols were seen or repeated such as SPIKES, Kay’s ten step approach, a 7 step approach for end of life news, PEWTER, BREAKS and “In person, In time” (Buckman, 1992; Kay, 1996; Von Gunten et al, 2000; Nardi et al, 2006; Narayanan et al, 2010; Sobczak, 2013).
Table 1: Characteristics of Final Studies Included for Recommending Suitable Model for Breaking Bad News (n=14)
Evidence on Breaking Bad News
Patient’s emotional reactions to the hearing bad news are variable. According to Butow et al. (1996) the most frequent responses to the cancer were feeling shocked (54%), frightened (49%), accepting (40%), and unhappy (24%). A small number of patients (15%) were not worried (Butowet al, 1996).
In most fields of medicine, excluding emergency department, there is a space of time spent by patients in receiving different opinions from different physicians and conducting paraclinical tests; so that health care deliverers may get ready in advance for delivering bad news (Mehta 2008). However, in critical care setting regarding its conditions and dynamics, teamwork with patients’ family members, nurses; social workers are required apart from thorough attention and planning (Watson 2008). As existing models do not consider the exclusive aspects of the critical care setting; the proposed critical care model for communicating the news of death of a loved one incorporates and modifies steps from other models intended to convey bad news to patients, and give death notifications in the community (Watson 2008).
In order to describe the stress related to delivering bad news, Ptacek and Eberhardt (1996) suggested a model that describes the medical care giver’s experience to that of the patient (Ptacek et al, 1996). They proposed that the care giver’s stress before breaking bad news reaches to its highest amount, while the patient’s stress rises a little while later on (Ptacek et al, 1996; Lee et al. 2002).
Some worried physicians may stay away from delivering bad news, and this may lead to not conveying upsetting information such as a weak prognosis or getting across unnecessary optimism to the patient. Instructions for verifying patient’s intentions on involvement in decision-making, and an approach for reducing their distress on the delivery of bad news can raise assurance and self-confidence of medical care givers, and reduce their burn out and stress in these type of procedures (Baile et al, 2000). On the other hand it can also persuade patients to accept difficult treatment planning (Baile et al, 2000).
In a retrospective study on 54 family members of 48 patients, who had died in an intensive care/emergency setting, the importance of different elements related to receiving bad news, were evaluated. Factors related most were recorded as: attitude of the deliverer of news (72%), the transparency of the message (70%), confidentiality (65%), and awareness or ability of the deliverer in answering questions (57%) (Jurkovich et al. 2000).
Paul et al, assessed the progress of the evidence base in breaking bad news to cancer patients. In total, the retrieved relevant publications were 245 that 55.5% supplied new data and 16.7% were intervention studies which aimed more on enhancing provider skills rather than patient outcomes (9.8% of studies) (Paul et al, 2009).
Review of Protocols
In the following paragraphs, the most important protocols in “Giving Bad News” have been demonstrated.
SPIKES model, suggested by Buckman in 1992, is an organized and effective procedure for communicating bad news. His 6 steps were the following: (a) start off well, (b) find out how much the patient/family knows, (c) find out how much the patient /family want to know, (d) share the information, (e) respond to patient’s/family feelings, and (6) plan and follow through (Buckman 1992).
This model was modified in 2005 to P-SPIKES (Table 2) which is a protocol for delivering unfavorable information to cancer patients about their illness (Kim et al. 1999; Baile et al. 2000, Buckman 2005). Users of this model have reported more confidence in their ability to discuss unfavorable medical information with their patients (Watson 2008).
Table 2: Summary of SPIKES Steps Along with Suggested Phrases
Another practical and comprehensive model, synthesized from multiple sources, was developed by Rabow and McPhee that uses the simple catchword ABCDE: advance preparation, building a therapeutic setting /relationship, communicate well, deal with patient and family responses, encourage and authenticate feelings (Rabow et al. 1999).
PEWTER Model is specifically developed for emergency department personnel, which despite providing emergency care; may encounter delivering news of death, violent crimes, school shootings, natural disasters or terrorist attacks (Nardi et al. 2006; Watson 2008). The components of the PEWTER model are as follows; P: Preparing the one giving the news through education and training, and preparing the setting and the approach for giving the news, E: Evaluating what the listener already knows, W: Warning by making a brief statement followed by a moment of silence to prepare the listener for the bad news that comes next, T: Telling the news, E: Emotional response: paying attention to and responding appropriately to the listener’s emotional responses, R: Regrouping by helping the listener move forward with the next steps (Nardi et al. 2006)
Lee et al. (2002) in their study discuss that a multidisciplinary panel of experts endorse several recommendations on communicating bad news. Furthermore, they were rated as essential or desirable by more than 70% of 100 patients with cancer. Many of these recommendations can be found in published protocols, and can be summarized as these steps: 1. get ready for the encounter, 2. evaluate the patient’s perception of the situation and enthusiasm to receive the news, 3. reveal the news in an easy and straightforward approach, 4. react to the patient’s feelings by keeping quiet and still for him to communicate his emotions, 5. present readiness to talk about consequences of the news, including: Prognosis, Treatment alternatives, Consequence on quality of life, 6. Offer additional supportive resources including: Assistance talking to others, other support services. 7. Sum up the dialogue: reaffirm vital aspects, inquire if there are any other issues. 8. organize a follow-up interval for patient and family queries and fears, 9. keep a record of the argument in the medical record (Lee et al. 2002; Baile et al. 2000; Buckman 1992).
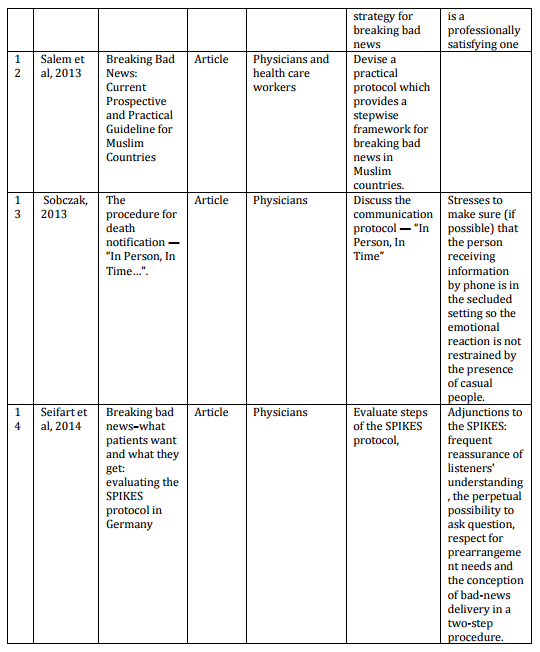
Several guidelines have been developed for Breaking Bad News in different countries, and two of them are demonstrated in Table 3 which have been prepared in the United Kingdom (National Council for hospice and specialist palliative care services 2003; Yorkshire cancer network 2005).
Table 3: Two Examples of Breaking Bad News Guidelines
McGuigan et al. in 2009 in their study on communicating bad news to patients have mentioned a ten-stage strategy that has been developed as a model, from the work carried out by Buckman (1992), Kaye (1996), Faulkner (1998) and Abel et al. (2001) “to support and assist nurses engaged in difficult conversations with patients”. They recommend that a reflective approach to care can assist nurses to learn from encounters and use their experience to converse bad news to patients in an appropriate manner. The ten strategies are as follows: 1. Getting ready, 2. Determine the knowledge of the patient, 3. Determine what the patient desires to know, 4. Give an alarming signal either orally or non-orally, 5. Converse bad news delicately, 6. Recognize distress and assist the patient in demonstrating his or her emotions 7. Recognize and categorize worries, 8. Assess the patient’s current information requests 9. Determine the patient’s help networks, 10. Establish what kind of help is available and what will take place subsequently (Buckman 1992; Kaye 1996; Faulkner 1998; Abel et al. 2001; McGuigan et al. 2009).
Discussion
Bad news can be defined in different circumstances such as state of despair and no optimism regarding current disease situation, a risk to an individual’s health in any respect, a threat to disrupt a conventional routine of the daily life, or communicating the idea that a person has reached limitation on control of his or her days ahead (Bor et al, 2000; Barnett, 2004; Hawken, 2005).
Buckman (1992) suggested that the effect of bad news depends on the difference between the patient’s expectations and the reality of the situation. Circumstances that can give rise to difficult conversations in clinical settings include (Buckman, 1992):
Informing a patient that his or her operation has been cancelled.
Informing a patient that his or her treatment will be delayed.
Confirming a diagnosis that will affect a patient’s life expectancy and/or quality of life significantly.
Discussing a placement of choice for long-term care provision.
Surveys conducted from 1950 to 1970, revealed that when treatment prospects for cancer were hopeless, most physicians considered it damaging to the patient, to disclose the bad news about the diagnosis. Amazingly, while treatment advances have changed the course of cancer so that it is much easier now to offer patients hope at the time of diagnosis; they have also created a need for increased clinician skill in discussing bad news (Oken, 1961; Buckman, 1992). The interactions between end stage patients and the medical practitioners providing care to them have various aspects, and sound information on those relationships is limited (Wenrich et al. 2001). However, a review of studies on patient inclination regarding receiving of a terminal diagnosis demonstrated that 50% to 90% of patients preferred hearing all the details and few did not want to get hear it all (Ley 1988). Therefore, traditional medical training that focused on biomedical model resulted in less advanced communication knowledge, and skill in physicians leading to doubt and discomfort in breaking bad news and fleeing this responsibility (Ley 1988).
Silverman et al (2005) in their study summarized types of communication skills along with the related comments as follows (Silverman et al, 2005):
Content skills: What health care professional communicate
Process skills: How they do it
Perceptual skills: What they are thinking and feeling
Communication skills regarding delivering bad news to patients and their relatives are currently considered very critical and invaluable by physicians and health care providers. Research and investigation on facilitating strategies can be very helpful on the development and promotion of physician-patient interactions in breaking bad news. All the presented strategies have communal aspects in terms of general content, and experts’ consensus insist on compliance to these principles in delivering bad news.
Three common areas are observed in the reviewed guidelines or protocols in order to present a suitable recommendation in three categories:
Preparation (When)
Preparation of the physician: preparation regarding mental and spiritual aspects, consideration of time limitation and revision of the information to be communicated.
Preparing patients and their relatives: identifying whether patient desires to know the bad news, or is it better to deliver the news through close relatives.
Preparing the environment: Arrange a suitable emotional, social, and even scientific surrounding along with building a logical, fundamental relationship with patients and their relatives. An example would be suitable physical conditions, sufficient lighting, comfortable furniture and minimum noise pollution.
Delivering (What)
Evaluate patients’ and their families’ knowledge of their illness and condition.
Delivering the bad news professionally, wisely and thoughtfully to patients and their relatives through forming an appropriate humane and compassionate relationship in a simple and clear language without using incomprehensible and technical terms.
Taking control and managing consequences and aftershocks of delivering bad news through professional, technical, ethical and legal principles. For example keeping silent, letting the patient and their family express their emotions, offer real support and sympathy, controlling the amount of information transferred and time management. Mentally and emotionally be prepared to encounter a wide range of possible reactions considering patients’ and their relatives’ believes, thoughts, customs, culture and personalities.
Arrangement (How)
Make a prompt appointment with the patient or relatives after breaking bad news, preferably in the following days to revise the important transferred information.
Present information, brochures and supporting resources regarding the illness. Answer the probable questions raised by patients and their relatives.
Involve patient in decision making pertaining to the treatment process. Engage patients in supportive and preservative programmes to reduce their pain and restrain the disease.
It is noteworthy to point out the common aspects of the given solutions. They are general in terms of content, and denote experts’ consensus on the moment of delivering bad news. By studying these aspects, it is possible to promote the quality of physician-patient relationship specially while breaking bad news. The main limitation in this study was the deficiency of research on thorough experiences regarding reducing stress in patients and physicians before, after and while delivering bad news. Therefore, conducting studies with valid and reliable questionnaires on this aspect of breaking bad news can be very helpful and informative.
Kumar, P. J. & Clark, M. L. (2005). ‘Kumar and Clark Clinical Medicine; Ethics and Ommunication,’ Chapter 1. University of Michigan: Elsevier Saunders, Michigan, USA.