Received date: 12 May 2014; Accepted date: 4 August 2014; Published date: 12 February 2015
Academic Editor: Deniz Necdet Tihan
Cite this Article as:
Ruslan Abdullayev, Sinan Hatipoglu, Mehmet Duran, Omer Burak Kucukebe, Bunyamin Ozturk, Demet Pepele and Abuzer Uludag (2015)," Multiple extremity blocks in a multi traumatic patient ", JMED Research, Vol. 2015 (2015), Article ID 654241, DOI: 10.5171/2015.654241
Objective: Regional anesthesia for operative procedures on extremities has lots of advantages over general anesthesia like sparing anesthetic drugs and mechanical ventilation, good postoperative analgesia, increased blood supply to the extremity. But sometimes regional anesthesia is indispensable because of the conditions like full stomach, difficult airway, pulmonary comorbidities. Few reports only exist in literature with simultaneous blockade of more than one extremity. We represent a case with simultaneous blockade of three extremities for surgical anesthesia. Case Report: A 56 year old male admitted to the hospital after a traffic accident. He had left radius and ulna fracture, right hand tendon and soft tissue damage, left femur fracture and pneumothorax on the left side. The patient was scheduled for the operation on the second day of admission and regional anesthetic technique was chosen because of the concern of possible pulmonary complications. Left infraclavicular block, right regional intravenous anesthesia for the arm and spinal anesthesia were performed at the same seance. The surgical procedure was completed without any complications. The patient was discharged at the postoperative day 2. Conclusion: We have successfully performed three different kinds of neural blockade for three extremities of a patient at the same seance. It is important to evaluate the patient individually and calculate the total local anesthetic doses before performing these kinds of procedures. We advise to execute the surgery on different days if there is a risk of systemic toxicity from local anesthetics with the calculated doses exceeding maximal doses acceptable.
It is a known phenomenon that regional anesthesia for operative procedures on extremities has lots of advantages over general anesthesia. Some of these advantages are sparing anesthetic drugs and mechanical ventilation, good postoperative analgesia, increased blood supply due to sympathectomy. Sometimes regional anesthesia is indispensable because of some conditions like full stomach, difficult airway, and pulmonary comorbidities. However, few reports only exist in the literature with simultaneous blockade of more than one extremity for surgical anesthesia (1-4). Here in our paper we present a multi-trauma patient undergoing multiple surgical interventions. We aimed to demonstrate important aspects of multiple regional anesthesia procedures at the same session.
Case Report
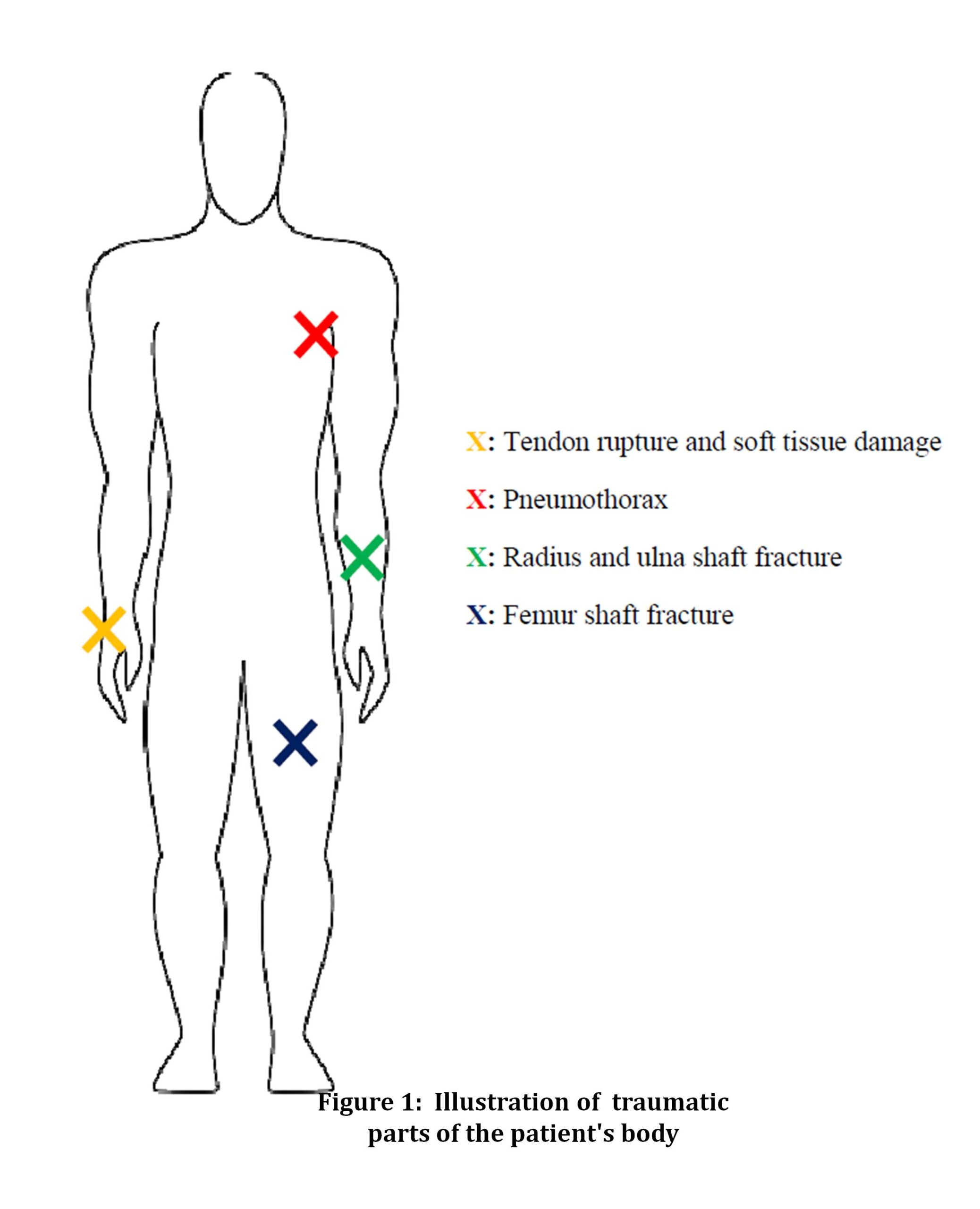
A 56 year old male admitted to the hospital after a traffic accident with tractor. The patient’s weight was 60 kg, height 165 cm. He was smoker. The patient had no chronic diseases. He had previous operation on left femur 5 years ago under regional anesthesia without complications. Laboratory examination revealed only elevated CK and CK-MB (819 and 106 U L-1 respectively) with mild leukocytosis (17.5 K -1). On the physical examination left femur fracture, left radius and ulna fracture and a laceration with tissue defect on the right dorsal part of the hand was observed with no injuries on the right leg (Figure 1). Radiological examination revealed left femur fracture together with old internal fixator, left radius and ulna fracture and mild pneumothorax on the left side. Consultation to the general surgery revealed 15% pneumothorax on the left and no need for chest tube placement. The patient was scheduled for the operation on the second day of admission by the general surgeon and orthopedist. Regional anesthetic technique was chosen because of known advantages over general anesthesia and concern of the possible pulmonary complications.
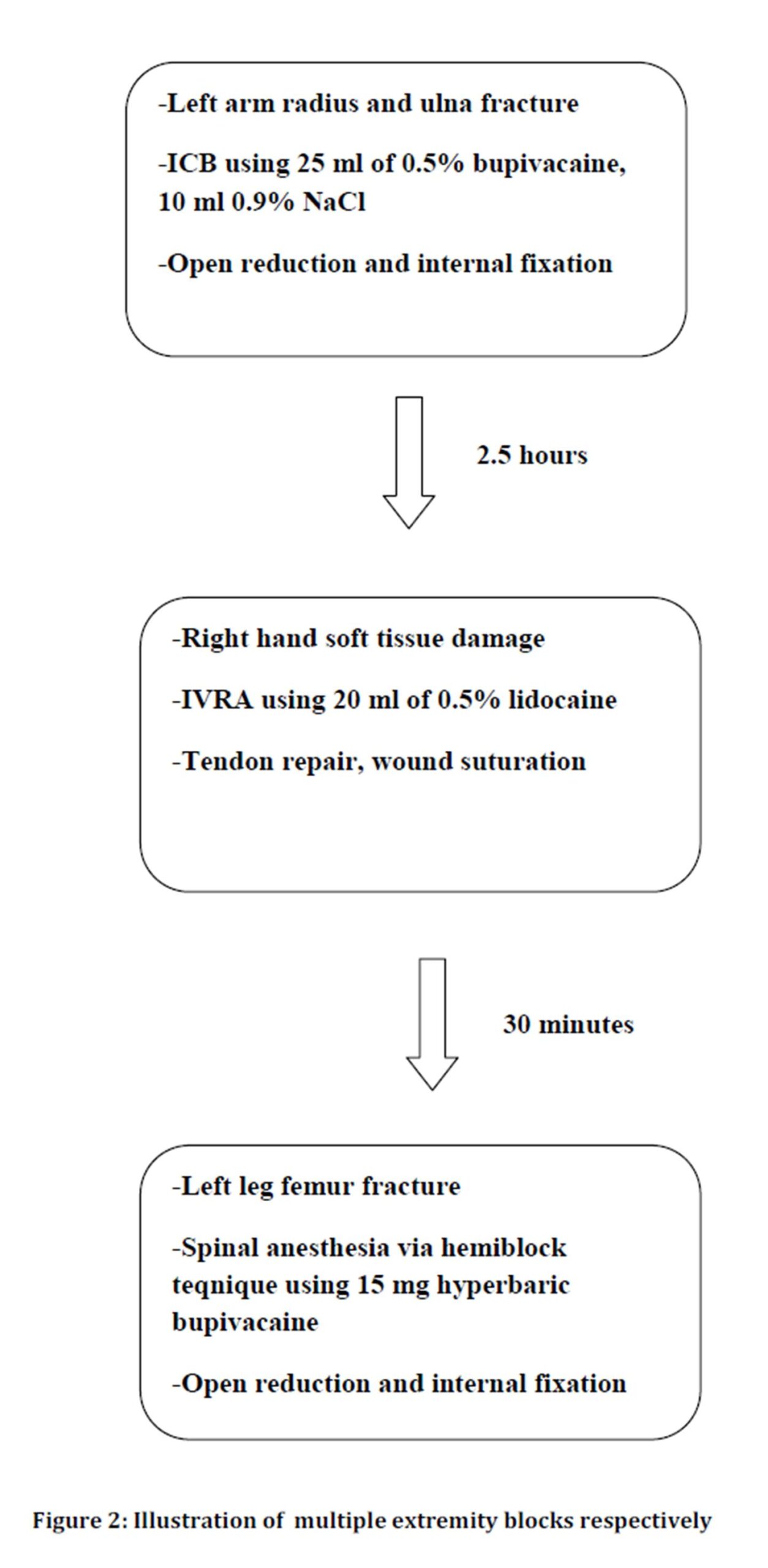
Intravenous access was established on the right foot with the non-invasive blood pressure monitoring on the same extremity. After completing the monitorization with ECG and SpO2 the patient was premedicated with midazolam 3 mg iv. The anesthesia was started with left infraclavicular block (ICB), (Figure 2). A neurostimulator (Stimuplex, B.BraunMelsunger, Germany) was used. The initial adjustment of the neurostimulator was as impulse duration 0.1 ms, frequency 2 Hz and current 3 mA. The brachial plexus was found on the third attempt after about 6 minutes searching and local anesthetic solution was injected after obtaining the flexion response of fingers with a threshold of 0.35 mA. A total of 35 ml of local anesthetic (LA) solution mixed with physiologic saline was used (25 ml of 0.5% bupivacaine, 10 ml 0.9% NaCl).
20 minutes after the procedure total anesthesia and motor blockade was elicited and the surgery was started on the left upper extremity. After the completion of the operation on the left extremity (open reduction and internal fixation of radius and ulna, lasted 2 hours) the right arm was anesthetized by intravenous regional anesthesia (IVRA) using forearm tourniquet. Totally 20 ml of 0.5% lidocaine (100 mg) was used for this (Figure 2). After 5 minutes the anesthesia was established on the right arm and surgery was started. The surgical procedure was completed within 20 minutes. The tourniquet on the right arm was left inflated until another 30 minutes. Lastly spinal anesthesia was performed to the patient to establish anesthesia on the left lower extremity (Figure 2). 15 mg hyperbaric bupivacaine intratecally was used with the patient situated in the left decubitis position. Propofol infusion 50 µg-1 kg-1 min was started due to the patient’s agitation before the surgical procedure on the left lower extremity started. The patient was followed by facial mask with 2 L min-1 O2 supply with spontaneous breathing. The surgical procedure was completed within 2 hours.
The patient’s vital signs were in normal range during the whole procedure. No complications occurred. He was discharged at the postoperative day 2.
Discussion
Being smoker and having pneumothorax on the left side the patient forced us to choose regional technique for the anesthesia. This would prevent the patient from potential pulmonary complications. Infraclavicular block (ICB) was performed on the left side because of the need for complete anesthesia of the left arm distal to the shoulder and need for tourniquet. ICB provides good surgical anesthesia for the lower arm (5). We have waited 20 minutes before anesthetizing the right arm. This lag was important to observe if any systemic local anesthetic toxicity develops and to separate the peak plasma levels of local anesthetics applied. Maurer et al., (4) observed peak plasma LA levels 20-45 minutes after bolus administration. Sandbu et al., (2) also had 20 minutes brake between the two ICBs applied at the same session.
ICB was chosen instead of supraclavicular block for the left extremity, as the latter is known to increase the risk of pneumothorax more than any other brachial plexus block (3). There are lots of ICB techniques illustrated in the literature (6). The main concern is that they vary according to the proximity of the needle insertion to the pleura and the blockade of the proximal braches of the brachial plexus. If one choose a technique that involves the more lateral needle insertion point he will probably not experience pneumothorax (7) but at the expense of possibility of sparing the proximal branches of the plexus. We chose Wilson’s method that involves needle insertion 2 cm medial and caudal to the coracoids process (8). Comlekci’s method (6) would have been selected as to not increase the risk of pneumothorax, but it was important for us to block the proximal branches of the plexus also.
We generally apply 40 ml of LA in our clinical practice for ICB. For the case a total of 35 ml of LA was used (25 ml 0.5% bupivacaine mixed with 10 ml 0.9% NaCl). For IVRA 100 mg lidocaine was used (5 ml 2% lidocaine mixed with 15 ml 0.9% NaCl). Total doses of bupivacaine and lidocaine used for all the three surgical procedures were 140 mg and 100 mg, respectively. Taking into account that maximum acceptable doses of bupivacaine and lidocaine are 3 mg kg-1 and 5 mg kg-1, respectively, the separated doses we had used were safe. But adding the doses of local anesthetics, we slightly exceeded maximum acceptable levels. However, this total dose was given in a long period of time, with the second half (i.e. IVRA) mixing with the circulation over nearly 1 hour time period. Franco et al., (3) and Maurer et al., (4) illustrated bilateral brachial plexus blockades with both exceeding total LA doses with no problems. They proposed that injecting LA over a period of time might have been protective. We had 20 minutes of anesthesia and 2 hours of surgery time for left upper extremity, so approximately 2.5 hours had passed before the application of the second dose of LA.
Spinal anesthesia was performed just after the both operations on the upper extremities completed. Propofol infusion was started because of the patient’s agitation. Propofol is known to treat systemic LA toxicity caused by lidocaine and bupivacaine (9, 10). Maurer et al., (4) routinely used propofol target controlled infusion to increase the threshold of LA central nervous system toxicity. Routine use of propofol infusion might be logical in these kinds of procedures.
It would be wisely to use USG for ICB as it may reduce the volume of LA (11). Sandbu et al., (2) applied bilateral ICB and used 20 ml of LA to each side with the help of USG. Bilateral infraclavicular catheter placement is also illustrated in the literature (12). It would have been wisely to put a catheter into the plexus area for postoperative pain management. Unfortunately we did not have that facility.
Although it was not measured, the patient’s α-1 acid glycoprotein (AAG) level was most likely elevated due to being an acute phase reactant. Plunkett et al., (13) proposed that it would account for the high total LA concentration for their patient. We think that the elevated levels of AAG might have bound free LA in the plasma having protective effect against the systemic toxicity.
We have successfully performed three different kinds of neural blockade for surgical anesthesia of three extremities of a patient at the same session. It is important to evaluate the patient personally and calculate the total local anesthetic doses before performing these kinds of procedures. We advise to execute the surgery on different days if there is a risk for systemic toxicity from local anesthetics with the calculated doses exceeding maximal doses applicable.
This case was the first in the literature, where the patient was operated on three extremities under regional anesthesia at the same seance. As it is an uncommon practice, we aimed to emphasize some important aspects of this procedure. This kind of procedure might be applied by some “brave” anesthesiologists, and they must be acknowledged by some important points.
First of all, the operating procedures must be separated (i.e. apllied at different days) if possible. Secondly, total anesthetic doses must be calculated and summed. Thirdly, maximum anesthetic doses may slightly exceeded if there is a big time lag between the irapplications. And finally, some measures must be taken to increase the treashold for the local anesthetic toxicity. The authors think that these important aspects will have contribution to the literature and be guiding for anesthesiologists.
Conflict of Interest
No conflict of interest wasdeclared by the authors.
5. Chin KJ, Singh M, Velayutham V, Chee V.(2010) “Infraclavicularbrachialplexusblockforregionalanaesthesia of thelowerarmpublished, in theCochrane Database SystRev”,2010, Issue 2. Art. No: CD005487.
6. Çömlekçi M, Başaranoğlu G, Süren M, Erkalp K, Aldemir T. (2009) “Humerusun Büyük Tüberkülü Referanslı Yeni BirİnfraklavikülerBrakiyalPleksus Bloğu YöntemininGeriye Dönük Değerlendirme Sonuçları”,J TurkAnaesthIntCare, 37(3): 145-51.
7. Gürkan Y, Özdamar D, Yılmaz AS, Toker K, Solak M.(2005) “Pediatrik Hastalarda İnfraklavikülar Blok Uygulamaları”, Türk AnestRean Der Dergisi, 33(6):480-483.