Namshan A Algarni1, McLaughlin Patrick2, Nouf M Alqarni3 and Majed Mutlag Alotaibi4
1King Saud university – College of Business Administration, Saudi Arabia
1,4King Khalid Military Academy- National Guard
2,3 Cranfield university, Cranfield, United Kingdom
Volume 2020,
Article ID 790792,
Journal of Organizational Management Studies,
18 pages,
DOI: 10.5171/2020.790792
Received date: 26 June 2018; Accepted date: 7 September 2018; Published date: 17 December 2020
Academic Editor: Susan Chin
Cite this Article as:
Namshan A Algarni, McLaughlin Patrick, Nouf M Alqarni and Majed Mutlag Alotaibi (2020)," The Effects of Cultural Aspects and Leadership Practices on the Healthcare Organizations’ Performance: The Case of Saudi Arabia”, The Journal of Organizational Management Studies, Vol. 2020 (2020), Article ID 790792, DOI: 10.5171/2020.790792
This article aims to investigate the effects of cultural factors and leadership practices towards organisational performance development in healthcare organizations. A case study of one of Saudi Arabia’s key healthcare providers was used. This study investigated the leadership practices, organizational culture, and performance improvement in the case study of healthcare organisations using qualitative interpretive paradigm to explore, explain and describe “the current state” based on the perceptions and opinion of individuals. Constructive-interpretivism philosophical approach is used for this study, employing a qualitative strategy. The study is specifically sought to determine the factors that promote and inhibit leadership performance improvement culture. Results suggest the heavy influences of organisational culture and other factors in the case study sector such as religious and national cultures, on the leadership performance. Research participants indicate that positive and negative behaviours of leaders and executives in top management affect the performance of employees and shape the organisational culture. The implications of these findings are highlighted, as well as the need to further explore how cultural factors and leadership practices can affect the level of productivity in this vital sector.
Keywords: healthcare performance, Saudi Arabia, leadership practices, culture, management practices, communication
Introduction
Recently, a number of studies have examined the effects of leadership practices and organizational culture on the productivity of healthcare organisations (Holden et al., 2015). According to McDonald (2014, p. 227), “There is a trend in healthcare systems around the world to place great emphasis and faith in improving leadership”. Furthermore, leadership development is increasingly recognised as fundamental to efficient and high-quality healthcare (King, Commission on Leadership and in the NHS, 2011),(A. West et al., 2014a). Also, leadership development is a key strategy for building cultures that value the experiences of patients and staff, learning and safety, (Francis report, 2013), quality (King, Commission on Leadership and in the NHS, 2011), (Berwick et al., 2008), effectiveness and knowledge translation (Kitson et al., 2008). Cultures that provide high-quality care are characterised by shared values translated into agreed ways of working that embrace care, compassion and support. Such cultures are developed through a leadership that recognises collective endeavours rather than command and control (A. West et al., 2014b; Washington et al., 2016). Organizational culture and leadership can be seen as two sides of the same coin, to the extent that leadership affects culture as much as culture influences leadership (Schein, 2010).
Earlier studies show a strong and consistent association amongst workplace characteristics that facilitate improvement. For example, Fottler (1981) discusses how the different constraints that characterise different sectors are likely to affect the performance of managerial functions (planning, organising, leading, and controlling). Studies have also identified some healthcare leadership characteristics that can inspire enthusiasm in others to include; a positive vision, inspiring core values, emotional intelligence, courage, and an engaging and inclusive leadership style (Bilimoria et al., 2005). In particular, charismatic House (1996), transformational Bass and Riggio (2006) and visionary leadership (Sashkin, 1988) theories have inspired volumes of research and numerous training programs for business managers (Thach and Thompson, 2007).
However, reviewing related literature showed a lack of understanding and research on the impact of leadership and culture on the productivity of organisations in Saudi Arabia particularly (Aseri, 2015; Khan and Varshney, 2013). Precisely, the limitation of social research towards organizational and structural reforms in the services of the healthcare sector has also been alluded by Al-Borie and Abdullah (2013). Thus, emphasising a need to investigate and understand the impact of leadership practices and organisational culture on the productivity of healthcare sector organisations.
There is little empirical evidence of the contribution of leadership practices in shaping the effectiveness of healthcare in the Gulf Cooperation Council (GCC) countries and particularly in the KSA (Khoja et al., 2017). The GCC consists of six member states; Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, and United Arab Emirates (UAE). These countries are currently experiencing an increased demand for healthcare services due to immense population growth, increasing life expectancy (Al-Bosaily et al. 2017).
The role of Islam as the first tenet of Saudi culture is largely established based on the Qur’an (the holy book) and the Sunna (the sayings and practices of the prophet Mohammed, peace be upon him) (Tønnessen, 2016, Aldraehim et al., 2012). These two sources unify the Islamic world and Saudis through Sharia law, which affects both the morality and the practice of employees in the workplace.
However, leadership is a major area of interest within the field of healthcare performance development Almgren (2017), Armit et al., (2015), and delivering improvements in the quality and safety of healthcare remains an international challenge (Turner, 2017; Taylor et al., 2014). Significantly, the Kingdom’s SR 270 billion healthcare plan under Vision 2030 will set Saudi Arabia on a fast trajectory to growth in the sector, projected to be a SR 92.6 billion market by 2020 (Saudi Embassy in the USA, 2017). Hence, the Saudi Vision 2030 presents certain challenges to the healthcare sector in terms of achieving Saudization targets and reducing dependence on foreign workers (Al-Bosaily et al., 2017). Expatriates currently make up much of the professional workforce, such as doctors, but Saudi Vision 2030 requires increased employment of Saudi nationals in these positions. This shows that education standards in the Kingdom, including those for medical and nursing degrees, will need to be raised to facilitate the achievement of that vision (Saleh and Otaibi, 2017).
This exploratory study was an initial stage of a research project designed to develop a framework to facilitate a culture of leadership performance improvement in the healthcare sector. An initial objective of the project was to understand the current situation by identifying the aspects that promote and those that inhibit leadership performance improvement culture in the healthcare sector in Saudi Arabia. This is in line with Weber and Joshi (2000) who indicate that cultural assessment functions can help the leaders of healthcare organisations to facilitate the desired change. According to Weber and Joshi (2000), this can be achieved by answering three crucial questions; first, what is the current culture? Secondly, what is the desired culture? and thirdly, what gaps exist and how can they be bridged? This study aims to address these questions by investigating the factors/aspects that promote and those that inhibit the improvement culture of leadership performance in the healthcare sector of Saudi Arabia. Our study therefore provides insights into how cultural aspects and leadership practices affect management performance in the healthcare sector.
Methodology
Schein’s model of organisational culture was employed in this study to gain an understanding of the culture improvement in the field study. Schein’s view focuses on what artefacts and values reveal about underlying assumptions (Schein, 2010). Schein argues that culture is a perceptual structure of underlying assumptions that have been discovered, developed, or improved by a given group as it learns to cope with its challenges of external adaptation and internal integration (Schein, 2016).
Understanding the philosophical position underlying the research is critical to choosing the most appropriate research design for research projects (Broad, 2014; Collins, 2017). However, this study investigates the aspects of the use case environment and explores how the use case environment’s culture ultimately affects the performance of its top-ranking officers. Top management teams create organizational culture based on their histories and personalities (Schein, 2010), this explains why research has extensively addressed the impact of founders or leaders on organizational culture (Klein et al., 2013; Nguyen and Mohamed, 2011; Sarros et al., 2002; Schein, 2010).
An exploratory study was designed to determine the effects of leadership style and practices on the job performance of leaders in Saudi Arabia’s healthcare sector. Hence, this study used a constructive-interpretive philosophical approach, applying a qualitative strategy to answer its questions and achieve the objectives of the research. Qualitative analysis was employed in this study to gain insights into the aspects that dominate the field study (use case domain) practices, as this could help identify and characterise the real situation of phenomena. According to Yin (2013, p .14), “a distinctive need for case study research arises out of the desire to understand complex social phenomena”. According to O’Leary (2017), qualitative data are represented through words, pictures or icons and analysed using thematic exploration; quantitative data are represented through numbers and analysed using statistics. Given that the present research into social phenomena is exploratory and interpretative in nature, qualitative methods are, as stated above, the most appropriate for it (O’Leary, 2017; Denzin and Lincoln, 2017; Alvesson and Sköldberg, 2017). To gain a sufficient understanding of the participants’ thinking and their views about leadership, qualitative research is often effective and efficient (Lincoln and Denzin, 1994; Bryman and Bell, 2015). Furthermore, Cassell and Symon (1994), Alvesson and Sköldberg (2017), also suggest that the qualitative method is particularly useful if the research question is related to organisational processes. This study has utilised interviews, informal chats, field notes, journals/magazines, observations to collect the required data. According to Padgett and Deborah (2016), in qualitative research, the potential data come from different sources, such as formal and informal interviews, participant observation and document analysis.
Before the fieldwork began, ethical clearance was obtained from Cranfield University. Data were collected over several months between June 2015 to February 2017. Other qualitative methods, such as a focus group and observations, were considered essential in this task to improve the validity of findings.
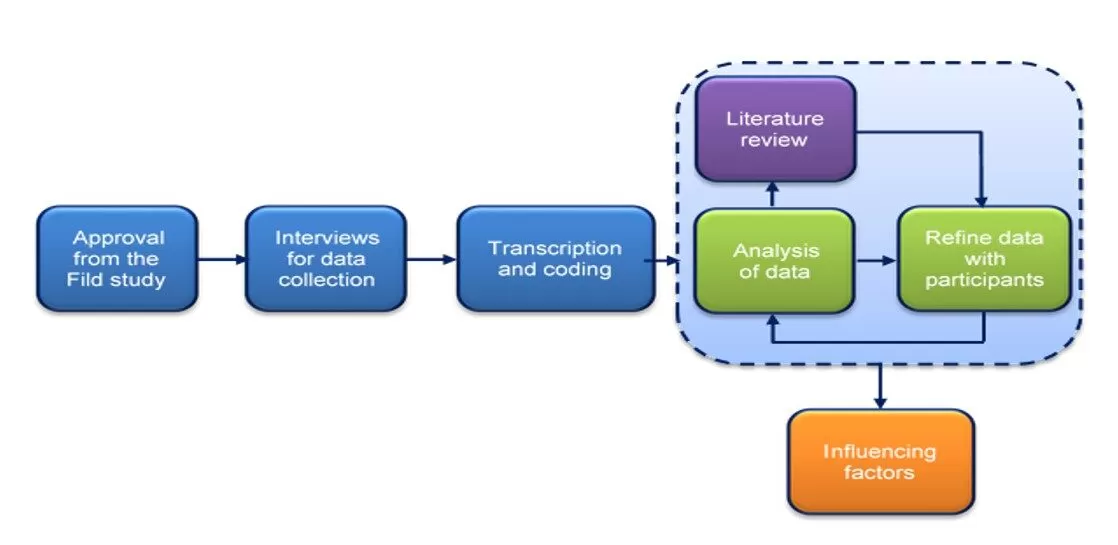
By following guidelines from Binder and Edwards (2010, p. 241), research participants were continually recruited and interviewed until the point at which no new data were produced that added new information or insights for constructing the theory. Figure 1 below illustrates graphically the overall data collection process of the study. However, throughout the iterative steps in data collection, theoretical sampling was followed to determine a certain level of saturation, as shown in Figure 1.
Figure 1: Data collection process
An issue focus (Sackmann, 1991) enables the surfacing of the hidden components of culture. Furthermore, an issue-focus method introduces a specific context that forces participants to draw on their existing knowledge (McLaughlin et al., 2005). This method helped the research to identify and understand the aspects that influence the culture of the organisation.
This research took place in one of the largest governmental healthcare providers in the KSA. Health affairs of the Ministry of the Saudi National Guard were involved as samples of this study. To make each interviewee feel as comfortable as possible, the interviewer maintained good interactions and relationship with participants prior to each interview. The interviews with the research participants generated 23 hours of audio recording and 624 pages of transcription for analysis. Theoretical saturation was reached after 33 interviews, the interviews were transcribed and translated into English and then analysed. The data management and analysis tool selected was NVivo software. This qualitative data analysis package was used for coding and to facilitate the analytical processes.
The data of this study were collected and then triangulated – semi-structured interviews were checked against the findings from a focus group discussion and direct observation.
According to Golafshani (2003, p. 604), “To improve the analysis and understanding of construction by others, triangulation is a step taken by researchers to involve several interpretations of the data by several investigators or peer researchers at different times or locations”. In addition to that, triangulation is needed to ensure trustworthiness of a study and to identify potential alternate explanations (Lincoln and Guba, 1989).
To achieve the aim and objectives of this research, the following phases have been identified.
Phase One: Exploring the Literature Review
Tasks
Conduct a comprehensive review of the literature in order to understand the various aspects of the research and to establish a comprehensive understanding of the field of research topic, as well as other related areas. This includes covering the related concepts, definitions, models and frameworks.
Methods
Conduct a literature review of articles and documents. Attend conferences; meet and discuss the topic with experts and colleagues. This phase is to identify key aspects, main authors and writers, as well as specialised journals and organisations.
Phase Two: Carrying Out Pilot Studies
Tasks
To determine in detail the main research problem in the field study that will be investigated in this research. Also, explore the existing enablers and inhibitors that influence leadership performance in the healthcare sector of the KSA and its characteristics. First, the researchers conducted a pilot study between June and July 2015.
Methods
The researcher designed and conducted a pilot study in the KSA as an initial step in order to help in clarifying the research problem issues and key elements. This study used interviews (issue focus) with selected interviewees among the health affairs of the Ministry of Saudi National Guard.
The fieldwork of the first stage of the study consisted of nine semi-structured interviews with participants from different job/position levels to elicit their beliefs and experiences. The questions aimed to identify the factors that relate to performance level, as encouragers or inhibitors of performance improvement.
Before the fieldwork began, ethical clearance was obtained from Cranfield University. The face-to-face interviews of the pilot study each lasted between 45 and 92 minutes. In an attempt to make each interviewee feel as comfortable as possible, the interviewer tried to build a good relationship with participants prior to each interview.
At the start of data collection, the participants received a description of the purpose of the study. All of the participants agreed to the audiotaping and transcription of the interviews, which produced a total of 515 minutes of speech and over 187 pages of transcripts. The interviews were first conducted in Arabic, and then the interviews were transcribed and translated into English. The study aimed to investigate what aspects in particular of the field under study and its culture ultimately affect the performance of its top-ranking officers. The data were collected and then triangulated – semi-structured interviews were checked against a document review and the findings from a focus group discussion and direct observation.
Jick (1979) explains the term ‘triangulation’ as the use of multiple techniques for data collection and analysis to investigate the same phenomenon from different viewpoints. Verbatim quotations representative of the data were selected (McAlearney, 2006). However, the researcher allowed the data to tell their own story, not spinning them to cover any specific topic. The researcher immediately wrote notes about every interview as soon as it ended.
After the first phase of interviews had finished, the researcher began to analyse the data to discern the main themes, phenomena and problems in the field in order to focus upon, explore and better understand them in the succeeding phases. After transcribing the recorded interviews and collecting the relevant documents, the researcher re-read the data several times to ensure an in-depth understanding of the case study. Following this, coded them and compared them with each other (theoretical sampling). These codes/concepts were then categorised and the categories, in turn, were compared and verified. The data were read again to enrich and/or confirm the categories.
Constant comparisons with the literature and the collected data were carried on. The iterative steps of data collection from the participants was performed. During the second stage of the study, the second series of personal interviews were held between December 2015 and January 2016. The interviewees were asked to take part in refining the aspects that emerged in the initial stage of the study.
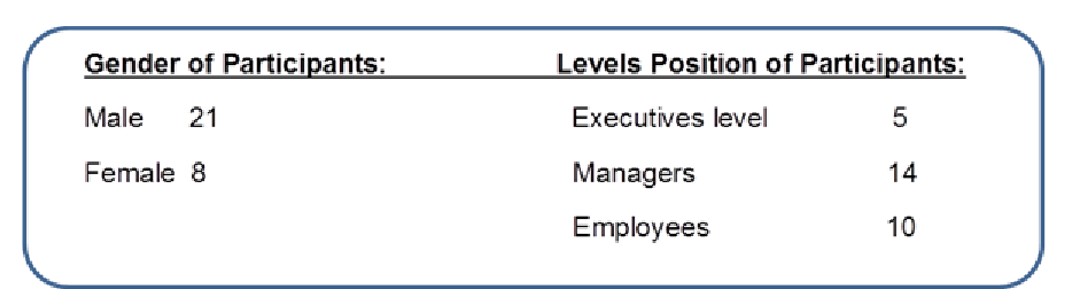
Figure 2: Participants demographic
Findings
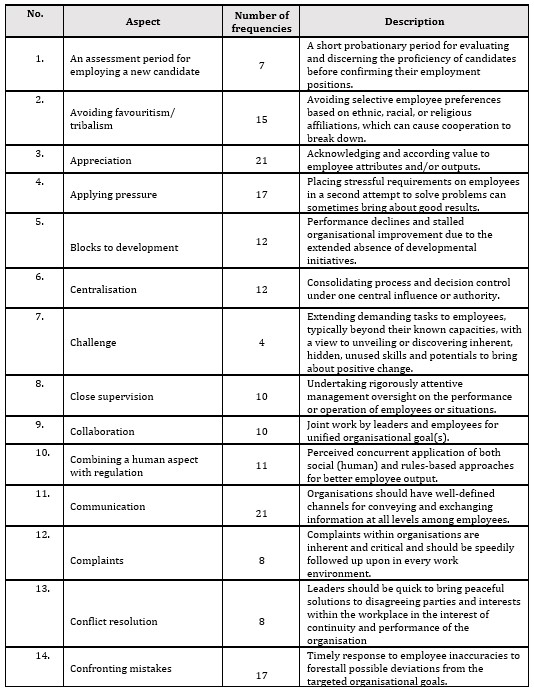
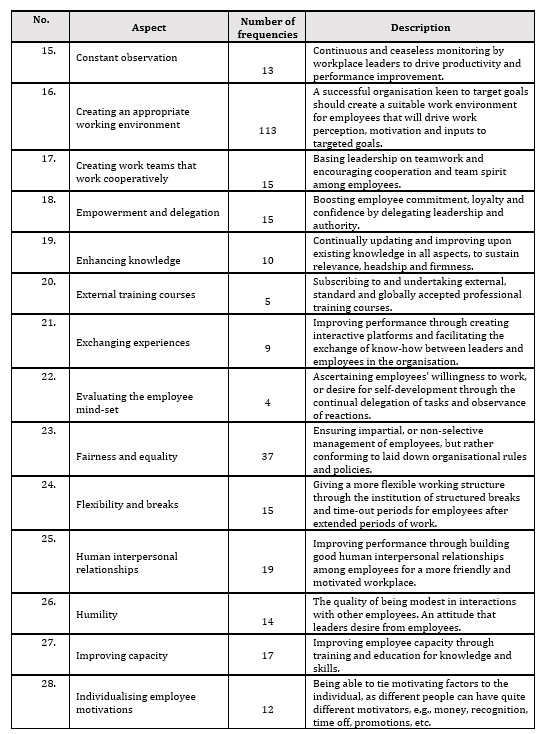
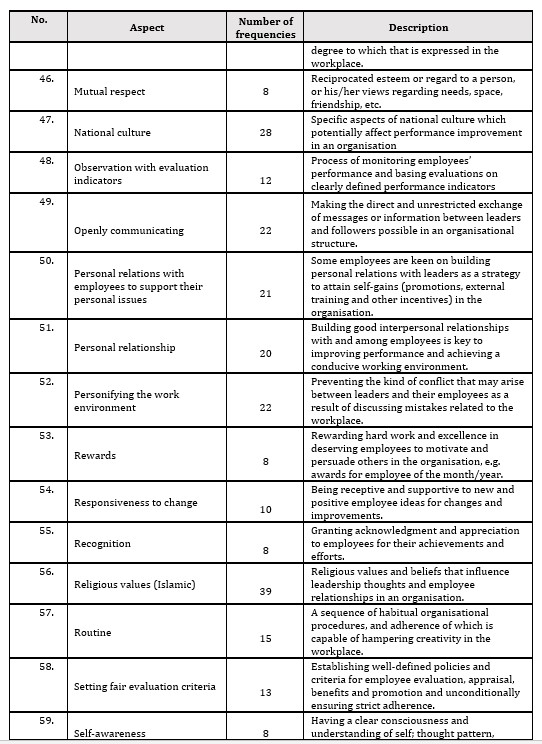
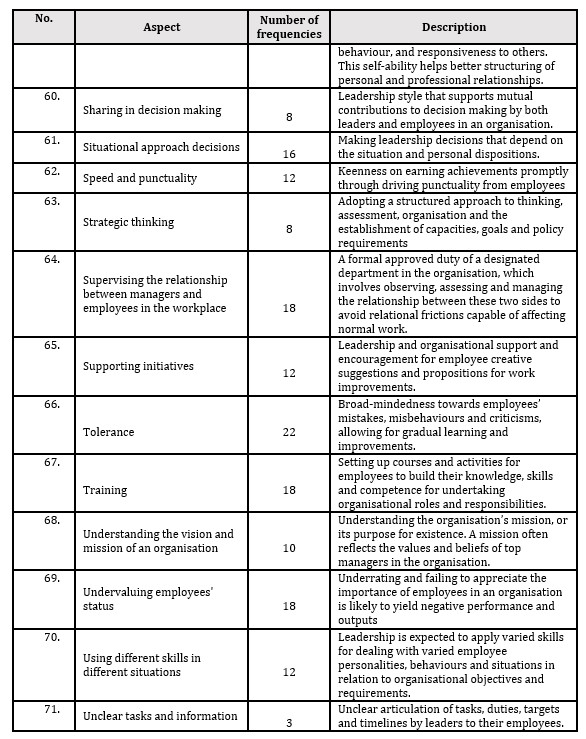
The results of this study revealed 71 aspects that promote and inhibit the performance improvement of leadership culture. These results show the aspects that influence the behaviour of leaders in the healthcare sector of the KSA, and play crucial roles in inhibiting or encouraging the development of leadership performance in this sector. Table 2 below displays the aspects that were obtained from the analysis and description of the data. It also illustrates the number of appearances of each aspect.
Table 1: Aspects with its frequencies and descriptions
The results of this exploratory study found that different factors influence the level of leadership performance in the healthcare sector in Saudi Arabia as illustrated above in Table 1. Particularly, culture-related factors seem to play a key role. The study also finds the heavy influence of organisational culture and structure on leadership performance. The dominance of these factors seems to be what mostly impact the decisions made by leaders. This also shapes the relationships between leaders and subordinates, and their commitment to the organisation.
The observed factors that mostly affect leadership performance in the Saudi healthcare sector incline towards the behavioural, cognitive or interpersonal qualities of the leaders. Other attributes emerged as important in shaping leadership performance developments, these include; fairness and equality, Islamic values, and the national culture. All these factors play a key role in a leader’s abilities to inhibit or encourage performance improvements.
Another interesting finding was the variation in the outcomes of assessment between male and female participants relative to the factors identified. Presumably, the difference may reflect the influence of culture and religion in the position of females in the KSA as presented by the study findings. For example, study results illustrate that a few women are allocated leadership positions in fieldwork-related areas. To support this finding one of the participants remarked,
“Particularly for the female here, if you achieved a leadership position and start to manage both genders (male and female), people around you will not be confident in your leadership as a female, this, as you know in general, is a result of the national culture aspects here”.
Surprisingly, only a minority of respondents mentioned factors such as strategic thinking and shared decision-making are valuable within a workplace environment, as shown in Table 1. Neglecting these important factors may lead to failure of healthcare organisations’ plans to change or improve their services.
However, most respondents agreed that other factors also play key roles in leadership performance level. These include; a combination of human-factor and regulation, use of fair evaluation criteria, difficulties introduced by the national culture, open communications, personal relationships, personalising the work environment, and tolerance. These factors yielded varied frequencies between 21 and 37.
Significantly, this study finds ‘Islamic values’ with a high frequency of 39 as the most influencing factor in the performance of leaders and employees in the organisations surveyed, as shown in Table 1. In this regard, one interviewee remarked,
“A lot of things [happen] in the work environment. If we apply the teachings of Islam in our work, we will find ourselves the greatest nation on earth, but sadly, we don’t. If you think of it right, Islam says: “Allah will be pleased with those who do their work perfectly”.
The second most influencing factor that appeared in these data was ‘fairness and equality’, with a frequency of 37. A notion of this perception as remarked by one interviewee goes thus:
“For me, the features of leadership are fairness and equality…along with brotherly treatment. Such things—I believe—are essential for leadership”. He added, “Of course the most significant thing I wish all leaders would have is … fairness. [It] is very important…it is the basis of judgment, once it is applied and handled in the best way between leaders and their followers…I find this crucial point to be essential with a very positive effect on the leader’s role, work, and responsibilities”.
Putting it in another way, one of the participants mentioned that:
“the major inhibitor is the lack of justice”.
Study findings also suggest a high influence of ‘national culture’ on; the practices of leaders, the job satisfaction of employees, and the general commitment towards an organisational goal. This factor had a frequency of 28, as shown in Table 1.
Furthermore, the study suggests a general view from participants highlighting the importance of emotional intelligence. Attributes like; being human and honest, showing initiative, having cognitive skills and an eagerness to develop capacity were noted to crucially contribute to the performance of organisations. Talking about this issue an interviewee remarked:
“I try to make the employees feel the importance of their decisions and ideas because that will make them closer. Also, I give them my guidance and advice to get benefit, follow the instruction and achieve my goals, too. It is not acceptable to deal with my staff in a complete formal way like: “hello, you have to do this and this…” certainly, they will do the task, but I do not prefer it that way”.
Some participants expressed the belief that creating a suitable culture and work environment can support daily more comfortable work. Supporting this view, an interviewee remarked:
‘The most important thing that a manager should be occupied with is how to create a suitable work environment, for the employee to feel that his manager or director is supporting him and not to feel that his manager is always a threat to him or taking actions against him’. One of the participants commented, “I totally believe that you can change the culture in a department, in the environment. You can put the objectives for it and don’t make these objectives requirements from the department but a nature of the department, a culture for that department to work in this way”.
From the perspective of the workforce requirements, this study emphasises the need to give real attention to the important factors to improve performance. These include; encouraging education and supporting skills and personal development – offering on-the-job training for employees during their regular working hours in the same work setting. For example, one interviewee said:
‘So, in the way you manage, you have to be up-to-date with the development that takes place in the health sector worldwide which is very dynamic and changeable. So, to be on top of this, you have to know what has changed and what has developed and what are the new things that came up in this field. Another thing is that a leader in the health sector should be knowledgeable. Not like any…I mean knowledgeable on daily basis. Currently, we always attend conferences, attend courses because the health sector is dynamic’.
To facilitate the improvement and change process in a workplace, the results of this study emphasise the important role of engaging all staff in change plans and development processes. On this, an interviewee remarked:
“This could help to engage all staff in any plans for change and development and thus facilitate change implementation in the workplace, avoid resistance, and enhance commitment and loyalty”.
Another participant also added:
“I found that when the person is convinced and feels that he is part of that change and that he wants it, he will be more productive and there will be success”.
Interestingly, one of the most noticeable findings that emerge from this study is the influence of several factors affecting leadership performance in the healthcare sector of KSA. For example, aiding employees who have personal issues, individualising employees’ motivation, having moral criteria for employment, using evaluation indicators to assess employees, supervising the relationship between managers and employees in the workplace and evaluating employees’ mindsets.
Strategic thinking, which seems to be currently lacking, is a key driver to improved performance in the Saudi healthcare system. As emphasised by one interviewee:
“Without a clear strategy…when I say strategy, some understand it as just a plan! It’s a plan that includes everything. It should have a financial aspect, a strategic aspect…it should include all departments, the manpower aspect. All these things must be put in an achievable plan and you have to have objectives”.
Monitoring and evaluation are also crucial in the process of improving performance development culture. Regarding this, one of the interviewees remarked,”
“I see the evaluation as a person’s mirror from where he knows his weaknesses and his strengths. The second thing is that evaluation is a chance for developing the employee. I stand with the management that says: I have that employee who has low communication skills; as an organisation, I have to provide a training course for him to correct this weakness. I shouldn’t just look at it as a point of weakness that he has without trying as an organisation to develop the employee”.
The study has also revealed one of the challenges in the Saudi healthcare system as “unclear tasks and information”. This relates to daily assignments from the top levels to subordinates as outlined in Table 1. About this issue, an interviewee remarked,
“When you give unclear guidelines to an employee, that will be disappointing for him/her. Some of them will ask you what you meant, whilst others may feel shy or afraid to ask. Your responsibility, as a leader, is to communicate clearly’’.
Furthermore, this paper underscores the importance of a clear and agreed-upon vision and mission statements, which provide a direction guide to staff as illustrated in Table 1.
In investigating the nature of the relationship between leaders and their followers within the workplace, most participants significantly believed in the importance of building a strong relationship through clear and dynamic communication channels. Hence, the study findings suggest a clear connection between designing flexible communication channels and successful change implementation in the workplace. To support this result, one of the participants remarked:
“communication with the staff is the main factor. One of the international patient safety goals is effective communication among employees, between the employee and the patient, and between the manager and employee. Communication helps to promote problem-solving”.
The findings of this study also suggest that an assessment period for employing a new candidate can enable organizations in this sector to elect the most competent staff and leaders. Talking about this, one interviewee pointed out that:
“leadership skills, problem solving, control and communication skills are essential things to follow when choosing the manager. Also, three-month experimental period is useful.It may be an evaluation after the experimental period. This method may help to reduce the problems that happen because of unsuccessful leadership”.
Discussion
Taken together, these results suggest that there is an association between the findings of this study and the existing research on leader efficiency, typically; Avolio and Gardner (2005) and Frankel et al., (2007). Both studies discuss the role of organisational context and climate on leadership practices. They also argue that a well-designed organisational context can moderate the style of leadership behaviours. They also suggest that organisations should provide open access to information, resources, and equal opportunity for all employees. This in line with Smith and Vecchio (2007) who stress that culture can determine whether or not the organization is able to survive under changing conditions.
However, this study produced similar findings to those of Sanghi (2016) who claims that successful organisations need to adopt a flexible organisational structure and improve communication to implement change effectively. Similarly, Yukl (2012) also finds that attention should be paid to delegating authority to staff and improving communication channels between managers and staff.
This is consistent with Franco et al. (2002) who argued that cultural characteristics can influence the organisational structure decision-making processes within organisations. Similarly, it is argued that cultural aspects pose a particular challenge to performance improvement in Saudi Arabia (Idris, 2007; Hodges, 2017). Moreover, Al-Bosaily et al. (2017) indicated that healthcare organisations face challenges to promote a culture that continuously improves the quality of services, patient safety and compassion in healthcare. This result overlaps with the thought from Sanghi (2016) stating that organisations need to establish and foster a suitable culture that can enable them to build strong working relationships in the workplace. This can be achieved through aspects such as working closely with the team, ensuring that needs are considered, issues are addressed and situations are managed in a collaborative, consultative, creative, and flexible manner (Sanghi, 2016; Willcocks and Wibberley, 2015).
Thus, this study emphasises that strategic thinking needs to receive real attention within the future plans of performance development. Moreover, the results of this study also overlap with others that emphasise direct communications across all levels. Mentoring and constantly evaluating outcomes can positively enhance the organisation’s position and improve its productivity (Armit et al. 2015; Bratton and Gold, 2017; A. West et al., 2014b). One of the most interesting findings is that there is a small number of female leaders in this sector in Saudi Arabia. A recent study that investigated the obstacles to women’s development in the KSA, (Hodges, 2017) revealed similar findings. Social, religious, cultural, and organisational challenges are the main obstacles faced by professional women in the KSA. This is also consistent with Al-Rasheed (2013) who stated that cultural and social factors do indeed play a role in the position of women. Religion has also been identified as a very dominant factor in seeking to preserve women’s status and confirm their position as subordinate members of society.
conclusion
Generally, the study offers some important insights into factors that particularly affect leadership performance in the healthcare sector of KSA. These include; maintaining personal relationships with employees as a form of personal support, individualising employees’ motivations, having moral criteria for employment, using evaluation indicators to observe and assess employees, supervising the relationship between managers and employees in the workplace, evaluating employees’ mind-set, and combining a human- aspects with regulations. This study is one of the first investigations to assess the impact of leadership practices and culture factors on organisational performance of Saudis’ healthcare. However, an in-depth study on the effectiveness of these factors in isolation can help in addressing the issue of leadership performance improvement in healthcare organisations.
West, M., Lyubovnikova, J., Eckert, R. and Denis, J.-L. (2014a) ‘Collective leadership for cultures of high quality health care’, Journal of Organizational Effectiveness: People and Performance, 1(3), pp. 240–260.
West, M., Lyubovnikova, J., Eckert, R. and Denis, J.-L. (2014b) ‘Collective leadership for cultures of high quality health care’, Journal of Organizational Effectiveness: People and Performance, 1(3), pp. 240–260. doi: 10.1108/JOEPP-07-2014-0039.
Abdulaziz Al-Bosaily, Glenn Lovell, Alain Sfeir, Ben Cowling, Joycia Young, Dino Wilkinson, Sara Khoja, Susie Abdel-Nabi and Niall O’Toole (2017) Growth opportunities in Saudi Arabia. Riyadh.
Al-Rabeeah, A. (2003) ‘The history of health care in the Kingdom of Saudi Arabia with emphasis on pediatric surgery.’, Saudi medical journal, 24 Suppl, pp. S9-10.
Al-Rasheed, M. (2013) A most masculine state : gender, politics and religion in Saudi Arabia. London: Cambridge University Press.
Aldraehim, M. S., Edwards, S. L., Watson, J. A. and Chan, T. (2012) ‘Cultural impact on e-service use in Saudi Arabia: the role of nepotism’, International Journal for Infonomics (IJI). Infonomics Society, 5(3/4), pp. 655–662.
Almgren, G. R. (2017) Health care politics, policy, and services: a social justice analysis. London: Springer Publishing Company.
AM Idris (2007) ‘Cultural barriers to improved organizational performance in Saudi Arabia’, A.M. Advanced Management Journal, 72(2), p. 36.
Aseri, M. (2015) LEADERSHIP A Study of Global and Cultural Context In Saudi Arabian Organisations. The University of Manchester.
Avolio, B. J. and Gardner, W. L. (2005) ‘Authentic leadership development: Getting to the root of positive forms of leadership’, The Leadership Quarterly, 16, pp. 315–338.
Bass, B. M. and Riggio, R. E. (2006) Transformational leadership. New York: L. Erlbaum Associates.
Berwick, D. M., Nolan, T. W. and Whittington, J. (2008) ‘The Triple Aim: Care, Health, And Cost’, Health Affairs, 27(3), pp. 759–769.
Bilimoria, D., Godwin, L., Sims, R. R. and Quatro, S. A. (2005) ‘Engaging people’s passion’, Leadership: Succeeding in the Private, Public, and Not-for-Profit Sectors.
Binder, M. and Edwards, J. S. (2010) ‘Using grounded theory method for theory building in operations management research: a study on inter-firm relationship governance’, International Journal of Operations & Production Management. Emerald Group Publishing Limited, 30(3), pp. 232–259.
Bratton, J. and Gold, J. (2017) Human resource management : theory and practice. 6th edn. London: Macmillan Education UK.
Broad, C. D. (2014) Religion, Philosophy and Psychical Research : Selected Essays. London: Routledge.
Bhaduri, R.M. (2019), “Leveraging culture and leadership in crisis management”, European Journal of Training and Development, Vol. 43 No. 5/6, pp. 554-569.
Collins, H. (2017) Creative research : the theory and practice of research for the creative industries. London: Bloomsbury Publishing.
D Denham, J Bratton – Organizational Leadership, 2020
Fottler, M. D. (1981) ‘Is management really generic?’, Academy of Management Review. Academy of Management, 6(1), pp. 1–12.
Francis report (2013) ‘Francis in brief: key nursing recommendations’, Nursing Times, 109(7), pp. 1–20.
Frankel, A., Gardner, R., Maynard, L. and Kelly, A. (2007) ‘Using the communication and teamwork skills (CATS) assessment to measure health care team performance’, The Joint Commission Journal, 33(9).
Garrido-Franco, M., Ehlert, S., Messerschmidt, A., Marinkovic’, S., Huber, R., Laber, B., Bourenkov, G. P. and Clausen, T. (2002) ‘Structure and function of threonine synthase from yeast.’, The Journal of biological chemistry, 277(14), pp. 12396–405.
Gary Yukl (2012) Leadership in Organizations (8th Edition): Amazon.co.uk: Gary Yukl: 8601404994968: Books. New York: Pearson Education.
Golafshani, N. (2003) ‘The Qualitative Report Understanding Reliability and Validity in Qualitative Research Understanding Reliability and Validity in Qualitative Research’, The Qualitative Report, 8(4), pp. 597–606.
Golafshani, N. (2003) ‘Understanding reliability and validity in qualitative research’, The qualitative report.
Hamdan, A. (2005) ‘Women and Education in Saudi Arabia: Challenges and Achievements.’, International Education Journal. ERIC, 6(1), pp. 42–64.
Hodges, J. (2017) ‘Cracking the walls of leadership: women in Saudi Arabia’, Gender in Management: An International Journal, 32(1), pp. 34–46.
Holden, K., Akintobi, T., Hopkins, J., Belton, A., McGregor, B., Blanks, S. and Wrenn, G. (2015) ‘Community Engaged Leadership to Advance Health Equity and Build Healthier Communities’, Social Sciences, 5(1), p. 2.
House, R. J. (1996) ‘Path-goal theory of leadership: Lessons, legacy, and a reformulated theory’, The Leadership Quarterly, 7(3), pp. 323–352. doi: http://dx.doi.org/10.1016/S1048-9843(96)90024-7.
Khan, S. A. and Varshney, D. (2013) ‘Transformational Leadership in the Saudi Arabian Cultural Context: Prospects and Challenges’, in Culture and Gender in Leadership. London: Palgrave Macmillan UK, pp. 200–227.
Khoja, T., Rawaf, S., Qidwai, W., Rawaf, D., Nanji, K. and Hamad, A. (2017) ‘Health Care in Gulf Cooperation Council Countries: A Review of Challenges and Opportunities.’, Cureus. Cureus Inc., 9(8), p. e1586.
King, T., Commission on Leadership, F. and in the NHS, M. (2011) the future of leadership and management in the nhs No more heroes Report from The King’s Fund Commission on Leadership and Management in the NHS. London.
Kirsten Armit, Dr Lola Loewenthal, Dr Regina Eckert, Thomas West, A. L. (2015) Leadership and leadership development in health care, TheKing’sFund.
Kitson, A. L., Rycroft-Malone, J., Harvey, G., McCormack, B., Seers, K. and Titchen, A. (2008) ‘Evaluating the successful implementation of evidence into practice using the PARiHS framework: theoretical and practical challenges’, Implementation Science, 3(1), p. 1.
Klein, A.S., Wallis, J. and Cooke, R.A. (2013), “The impact of leadership styles on organizational culture and firm effectiveness: an empirical study”, Journal of Management & Organization, Vol. 19 No. 3, pp. 241-254.
Lincoln, Y. S. and Guba, E. G. (1989) Fourth generation evaluation. Sage.
Mcdonald, R. (2014) ‘Leadership and leadership development in healthcare settings – a simplistic solution to complex problems? Citation: McDonald R. Leadership and leadership development in healthcare settings – a simplistic solution to complex problems?’, Int J Health Policy Manag, 3(35), pp. 227–229.
McLaughlin, P., Bessant, J. and Smart, P. (2005) Developing an organizational culture that facilitates radical innovation in a mature small to medium sized company: emergent findings. 1826/858.
Mohammed Al-Borie, H. and Tanweer Abdullah, M. (2013) ‘A “DIRE” needs orientation to Saudi health services leadership’, Leadership in Health Services, 26(1), pp. 50–62.
Nguyen, H.N. and Mohamed, S. (2011), “Leadership behaviors, organizational culture and knowledge management practices: an empirical investigation”, Journal of Management Development, Vol. 30 No. 2, pp. 206-221.
Novak, Andrej, Breznik, Kristijan, and Natek, Srečko. ‘How Leaders Can Initiate Knowledge Management in Organizations: Role of Leadership Style in Building Knowledge Infrastructure’. 1 Jan. 2020 : 37 – 50.
Sackmann, S. A. (1991) ‘Uncovering culture in organizations’, The Journal of applied behavioral science, 27(3), pp. 295–317.
Saleh, A. and Otaibi, A. (2017) ‘An Overview of Health Care System in Saudi Arabia’, International Journal of Management and Administrative Sciences International Journal of Management and Administrative Sciences (IJMAS), 4(12), pp. 1–12.
Sanghi, S. (2016) The Handbook of Competency Mapping : Understanding, Designing and Implementing Competency Models in Organizations. London: SAGE Publications.
Sashkin, M. (1988) The visionary leader. Jossey-Bass.
Sarros, J.C., Gray, J.H. and Densten, I.L. (2002), “Leadership and its impact on organizational culture”, Journal of International Business Studies, Vol. 10 No. 2, pp. 1-26.
Saudi Embassy in the USA (2017) SAUDI ARABIA: POLITICAL, ECONOMIC & SOCIAL DEVELOPMENT. WASHNGTON. doi: MAY 2017 REPORT.
Schein, E. H. (2010) Organizational culture and leadership. San Francisco: Jossey-Bass.
Schein, E. H. (2016) Organizational culture and leadership. New York: John Wiley & Sons.
Smith, C.G. and Vecchio, R.P. (2007), Organizational Culture and Strategic Leadership: Issues in the
S, E., Ramly, M., & Alam, R. (2020). Leadership style, organizational culture and job satisfaction at employee performance. Point Of View Research Management, 1(3), 09-18.
Taylor, M. J., McNicholas, C., Nicolay, C., Darzi, A., Bell, D. and Reed, J. E. (2014) ‘Systematic review of the application of the plan-do-study-act method to improve quality in healthcare.’, BMJ quality & safety. BMJ Publishing Group Ltd, 23(4), pp. 290–8.
Thach, E. and Thompson, K. J. (2007) ‘Trading places: Examining leadership competencies between for-profit vs. public and non-profit leaders’, Leadership & Organization Development Journal. Emerald Group Publishing Limited, 28(4), pp. 356–375.
The Saudi General Authority For Statistics (2017) Surveys Demographic Survey 2016. Riaydh.
Tønnessen, L. (2016) Women’s Activism in Saudi Arabia: Male Guardianship and Sexual Violence. Bergen, Norway.
Turner, P. (2017) Talent management in healthcare : exploring how the world’s health service organisations attract, manage and develop talent. London: Palgrave Macmillan.
Washington, P. K., Li, Y., Durzinsky, D. S., Duffy, J., Shim, V., Barnett, N. M., Warren, N. and Stodd, K. (2016) ‘Implementation of survivorship care plans: Lessons learned at the Kaiser Permanente Oakland Medical Center.’, Journal of Clinical Oncology, 34(3_suppl), pp. 75–75.
Weber, V. and Joshi, M. S. (2000) ‘Effecting and Leading Change in Health Care Organizations’, The Joint Commission Journal on Quality Improvement, 26(7), pp. 388–399.
Willcocks, S. G. and Wibberley, G. (2015) ‘Exploring a shared leadership perspective for NHS doctors’, Leadership in Health Services. Emerald Group Publishing Limited, 28(4), pp. 345–355. doi: 10.1108/LHS-08-2014-0060.
World Health Organization (2016) WHO | Saudi Arabia, WHO. World Health Organization.
Yin, R. K. (2013) Case study research : design and methods. London: SAGE Publications.
Xie, L. (2019), “Leadership and organizational learning culture: a systematic literature review”, European Journal of Training and Development, Vol. 43 No. 1/2, pp. 76-104