Helicobacter pylori infection is a high prevalence infection worldwide, and it is more common in developing countries than developed ones (Magalhães and Luzza, 2006). It is a major risk factor for chronic gastritis, peptic ulcer and gastric cancer (Fock and Ang, 2010). The ABO blood group system is the most important in human blood transfusion. The blood group antigens present on RBC are permanent, fixed and lifelong biological markers of any individual, they are almost as individual as fingerprints (Ravn and Dabelstein, 2000). The distribution of the ABO blood groups varies in populations throughout the world (Garratty et al., 2004). In addition to clinical significance for transfusion and transplantation, it is becoming increasingly apparent that ABO antigens are of biological significance and may be associated with predisposition to, or protection from many diseases (Reid and Bird, 1990).
Many authors reported an association between blood group O and H. pylori infection (Kanbay, et al., 2005). While, others failed to find such an association (Niv et al.,1996). The ABO phenotype has been linked with stomach ulcers, which are more common in group O individuals and gastric cancer, which is more common in group A individuals (Iodice et al., 2010).
The aim of this study was to report for the first time the incidence of H. pylori infection among patients with dyspepsia symptoms, and to determine the relationship between the ABO blood groups and H.pylori infection in patients with various gastrointestinal symptoms, from Basrah-Iraq.
Materials and Methods
Sample Collection
Two hundred (200) patients with various gastrointestinal symptoms attending endoscopy unit at Teaching Hospital in Basrah, during the period from March 2011 to October 2012, were studied after obtaining their consent. These consecutively chosen patients were 110 males and 90 females whose age ranged from 18-75 years. Patients were diagnosed as having gastritis, gastric ulcer, duodenal ulcer and gastric cancer using specimens from the antrum of the stomach of each patient. Diagnosis of gastric carcinoma was based on the WHO classification (Hamilton and Aaltouren, 2000) while, gastritis was characterized by chronic inflammatory cells infiltration with degeneration and detection of microrganisms. One of the specimens was used for the rapid urease test (RUT) immediately after collection. The other two gastric biopsy specimens were placed in transport medium, brain heart infusion broth for bacterial culture and PCR.
Three ml of venous blood sample was drawn from each patient, then 2ml of it transferred into plain tube and centrifuged at 5000 rpm for 5-10 minutes. The serum was used for rapid diagnostic test in screening for the detection of antibodies against H.pylori (IgG). The remaining 1 ml of the blood was emptied into disposable tube, and used for determination of ABO blood group antigens by a standard hemagglutination test.
Rapid Urease Test (RUT)
One-minute ultra-rapid urease test (URUT) was performed according to (Thillainayagam et al., 1991). A positive RUT result was noted immediately by a change in the color of the solution from yellow to deep pink within the first minute.
Rapid Diagnostic Test (RDT)
This one step test is used for qualitative detection of IgG antibodies of H. pylori in the serum by using Rapid Diagnostic Test Kit (ACON, USA) (Ansorg et al., 1991). All the 200 collected sera from patients were examined for the presence of antibodies against H.pylori.
Bacterial Culture
Gastric biopsy samples after homogenate were cultured on MCUA slant tubes under microaerophilic condition at 37°C for 1-2 days by using MDCS method (AL-Sulami et al., 2002). Colonies of primary isolates of H.pylori were subcultured on MCUA medium plates and incubated at 37ËšC under microaerophilic conditions for 3-5 days. Suspected colonies were identified as H. pylori on the basis of the color of the medium changing from yellow to pink indicating urease activity, and further confirmed for positivity of urease, oxidase and catalase traits.
DNA Extraction and PCR
Genomic DNA was extracted directly from all biopsy specimens by using Wizard® Genomic DNA Purification Kit (Promega, USA) according to the manufacturer’s instructions. The extracted DNA was stored at -20°C until used. PCR was performed on extracted DNA from gastric biopsies directly using H. pylori 16SrRNA specific primers (Liu et al. 2008). The identification of the isolates have been confirmed by using the primer of the 229 pb of the 16S rRNA composed of forward 5´- TCG GAA TCA CTG GGC GTA A -3´and reverse 5´-TTC TAT GGT TAA GCC ATA GGA TTT CAC -3´. For the detection of H. pylori by PCR, amplification conditions were carried out in a 20”‰µl of reaction mixture containing 5 µl master mix, 1 µ”‰forward primer, 1 µl reverse primer, 5 µl DNA samples, 8 µl free deionized water. PCR conditions include: denaturation at 95°C for 5”‰min, followed by 30 cycles at 94°C for 30 sec, annealing at 52°C for 30 sec and extension at 72°C for45 sec, and an additional extension step at 72°C for 10”‰min. After completing PCR cycles, the amplified PCR products were electrophoresed in 2% agarose and 2000 bp ladder was used as DNA molecular weight standard. Then, the product was detected and examined under ultraviolet transilluminator, where a 229-bp band was considered a positive PCR result.
Determination of ABO Blood Group Antigens
The ABO blood group was determined for each patient by the conventional hemagglutination test using the anti- A, anti-B and anti-D sera. The ABO blood grouping procedure is based on the principle of agglutination or clumping as the patient’s blood is reacted with anti-A, anti-B and anti-Rh antibodies separately.
Statistical analysis
Statistical analysis was carried out by the use of the computer program, Statistical Package for Social Science (SPSS) version 21. The relationship between the parameters was determined using Chi- Square (X2) test. P value less than 0.05 was considered as statistically significant, and P- value less than 0.001 considered as highly significant.
Results
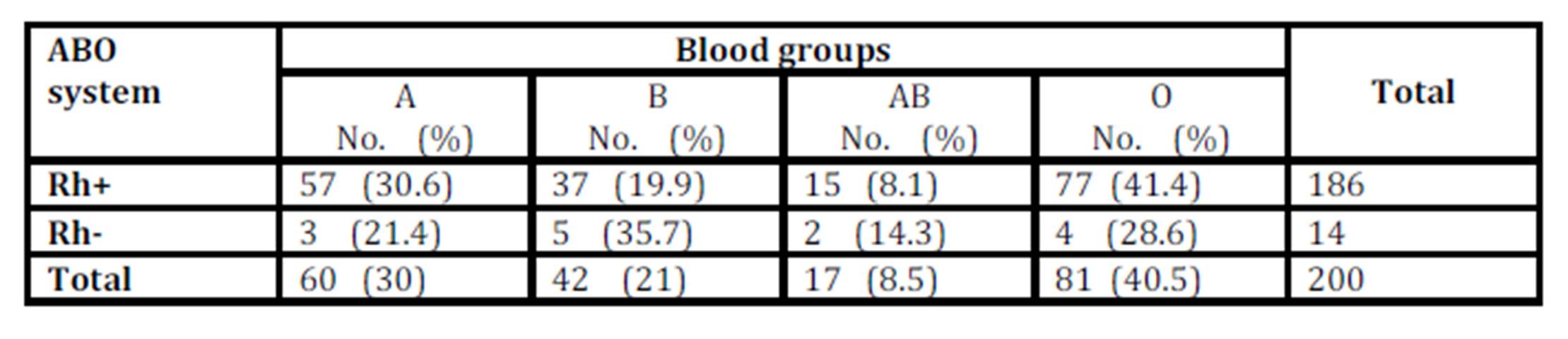
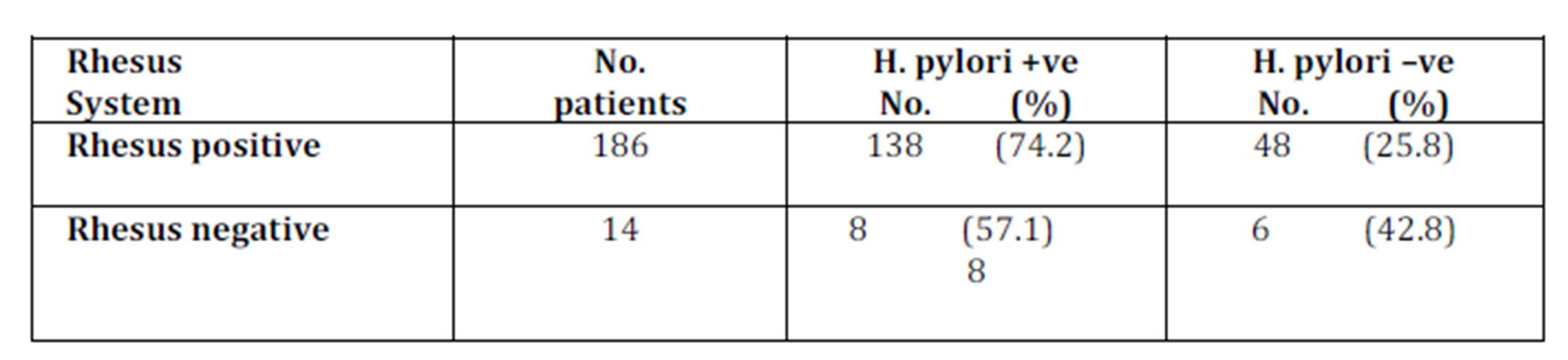
Of the two hundred patients with various gastrointestinal symptoms, 110 were males and 90 were females. The age range of patients was 18-75 years with the highest percentage >50 years old (29 %). The distribution of the ABO blood groups of the patients was O (40.5 %) followed by A (30 %), B (21 %) and AB (8.5 %), while 186 (93%) of patients were Rh-positive and only14 (7%) of patients are Rh-negative. The Rh+ distribution among blood groups was as follow: 57 (30.6%), 37 (19.9%), 15 (8.1%) and 77 (41.4%) for blood groups A, B, AB, and O respectively. While, Rh- distribution among blood groups was 3 (21.4%), 5 (35.7%), 2 (14.3%) and 4 (28.6%) for blood groups A, B, AB, and O respectively as shown in (Table. 1)
Discussion
The ABO blood group system is the most important in human blood transfusion. This system is used as a genetic marker in studies of associations with infectious and non-infectious diseases (Mattos et al., 2002). The ABO blood group antigens confers advantage of resistance against certain infectious disease (Reid and Bird, 1990). The risk of gastric cancer was found higher among those with the blood group A, while the gastric ulcer was more common in blood group O persons (Alkout et al., 2000 and Nakao et al., 2011).
Various diagnostic tests for H. pylori infection may have false negative results, and the use of multiple tests may help to provide a more accurate diagnosis of H. pylori infection (Akbar and El Tahawy, 2005 and Laheij et al., 2000). However, this study showed that H. pylori detection rate by RUT, RDT, culture and PCR were 66.5%, 69.5%, 71% and 67.5% respectively with no significant difference. Thus, a patient may be negative by culturing, but positive by PCR or other methods making the total positivity 73%. . The culture method was the most sensitive one; to detect this bacterium is ascribed to culturing on MCUA medium and applying the MDCS (Al-Sulami et al., 2002). Results on gender agree with some studies that indicated the males were associated with a higher risk of acquiring H. pylori infection than females (Ndip et al., 2004 and Ndip et al., 2009) while, disagree with other studies as males and females are infected at the same rate (Nwodo et al., 2009 and Rasmi et al., 2009).
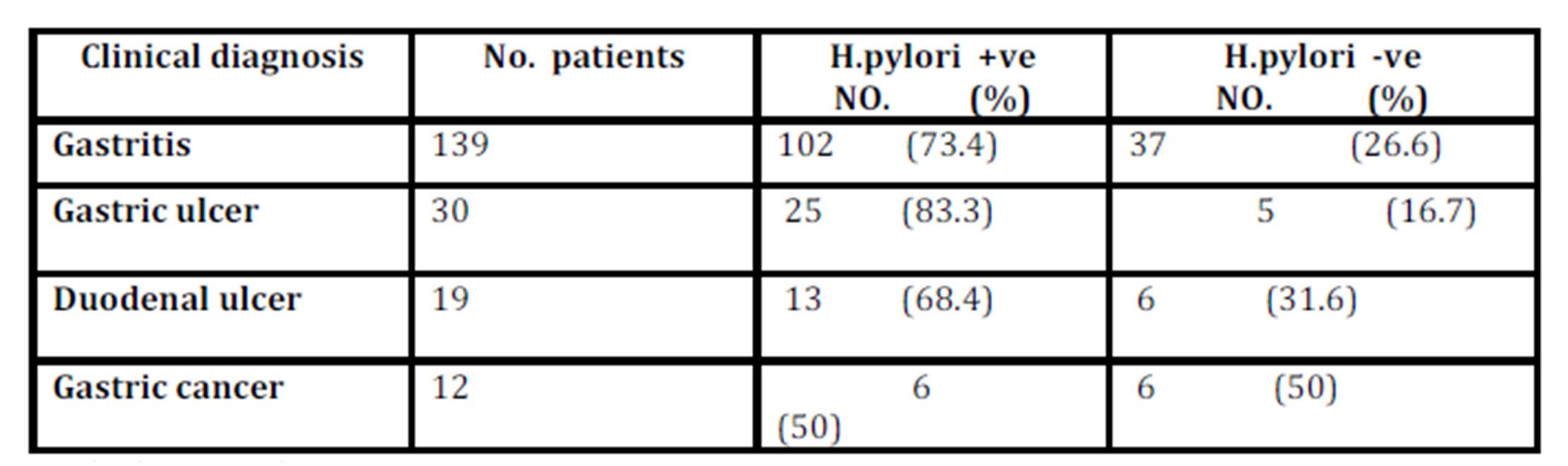
Studying the distribution of H. pylori infection and their clinical diagnosis among patients reveal that H.pylori positivity among patients with gastritis, gastric ulcer, duodenal ulcer, and gastric cancer were 73.4%, 83.3%, 68.6% and 50%, respectively. These results showed that the difference was statistically not significant (P>0.05) between H. pylori infection and the degree of clinical status of these patients.
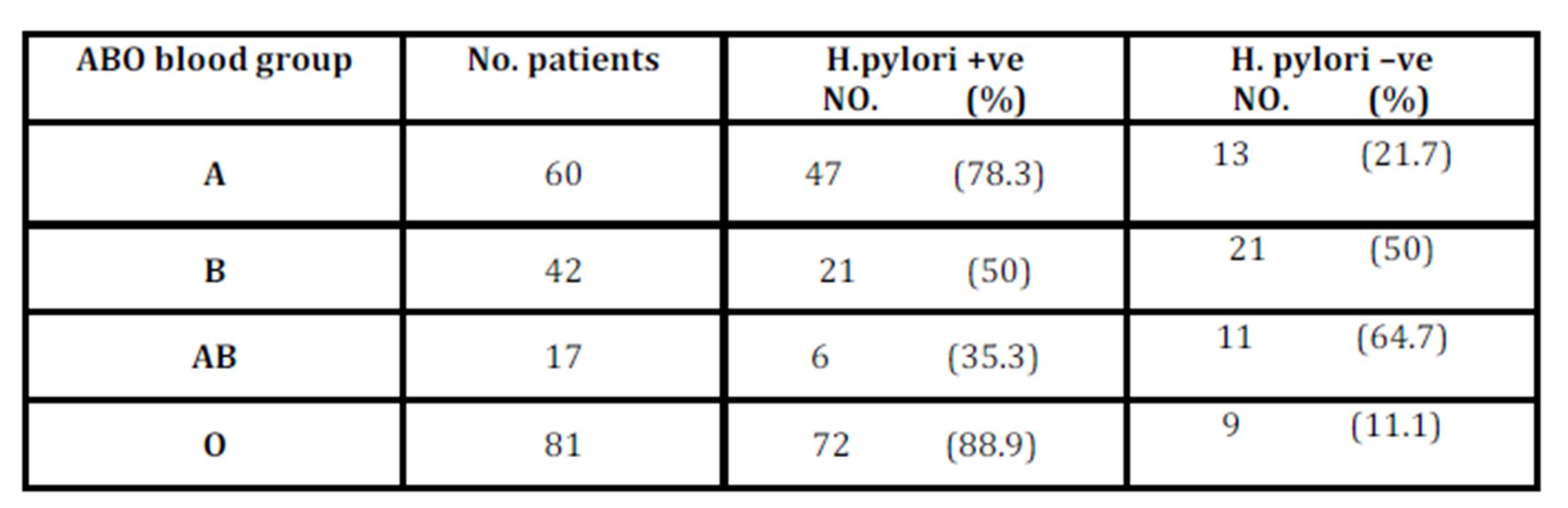
The results of this study showed that there was a significant association between ABO blood groups and H. pylori infection, in which type O has a greater tendency towards infection and type AB to non-infection. These results are reinforced by the data obtained from other researchers showing the greater susceptibility of blood group O to H. pylori infection (Kanbay et al., 2005and Mattos et al., 2002). While, the results disagree with some previous studies which demonstrated that the O blood group did not represent a risk factor for H. pylori infection (Seyda et al., 2007 and Sharara et al., 2006).
The H type 2, Lewis (a) can act as receptors for H. pylori on the gastric mucosa (Alkout et al., 2000). Additionally, it is demonstrated that epithelial cells of persons of group O bound signiï¬cantly more H. pylori than did cells of persons of other blood groups (Alkout et al., 1997 and Kanbay et al., 2005). H. pylori express lipopolysaccharides on its outer membrane including blood group antigen-binding adhesion A (BabA adhesin) which causes adhesion of bacteria to gastric epithelium and allow persistent colonization (Linde ‘N et al., 2002).
The present study demonstrated higher incidence of H. pylori among patients of blood group O with gastric ulcer ( 46.7%) as compared with A (20%), B (13.3%) and AB (3.3%) blood groups where that differs significantly (P0.05).These findings indicate that people of blood group O with gastric ulcer are more susceptible to infection with H.pylori as compared with other blood groups.
Previous studies demonstrated that individuals with blood group O have a higher risk of developing duodenal ulcers and also a higher incidence of gastric ulcers (Dhillon, B.S. and Shergill, 2004 and Martins et al., 2006). The increased susceptibility to peptic ulceration among persons with blood group O was duo to density of colonization of epithelial cells and higher inflammatory responses to H. pylori (Alkout et al., 2000).
Regarding Rh status, 74.2% Rh+ patients and 57.1% Rh- patients were positive for H.pylori. The present study showed no significant differences between the positive patients and negative patients, indicating that the presence of H.pylori did not relate to the Rh factor, which is in an agreement with previous study by Petrovic et al (2011).
References
1. Akbar, D.H. and El Tahawy, A.T. (2005) ʻʻHelicobacter pylori infection at a university hospital in Saudi Arabia, prevalence, comparison of diagnostic modalities and endoscopic findings,ʼʼ Indian Journal of Pathology and Microbiology, 48 (2) 181-185.
Publisher – Google Scholar
2. Alkout, A. M. Blackwell, C.C. and Weir, D.M. (2000) ʻʻ Increased inflammatory responses of persons of blood group O to Helicobacter pylori, Journal of Infectious Disease, ʼʼ 181( April )1364—1369.
Publisher – Google Scholar
3. Alkout, A.M. Blackwell, C.C. Weir, D.M. Poxton, I.R. Elton, R.A. Luman, W. and Palmer, K. (1997) ʻʻIsolation of a cell surface component of Helicobacter pylori that binds H type 2, Lewis a and Lewis b antigens,ʼʼ Gastroenterology, 112 (4) 1179-1187.
Google Scholar
4. AL-Sulami, A.A. Hammadi, S.S. and AL-Ghazawi, G.J. (2002) ʻʻA single step method for rapid isolation and identification of Mycoplasma pneumoniae from clinical specimens,ʼʼ Journal of Eastern Mediterranean Health, 8: 1-7.
Google Scholar
6. Ansorg, R. Von Recklinghausen, G. Pomarius, R. and Schmid, E.N. (1991) ʻʻEvaluation of techniques for isolation, subcultivation and preservation of Helicobacter pylori,ʼʼ Journal of Clinical Microbiology, 29 (1) 51-53.
Google Scholar
7. Dhillon, B.S. and Shergill, S.S. (2004) ʻʻ Prevalence of ABO and Rh blood groups in color vision defective Punjabi population,ʼʼ North Zone Ophthalmological Society Journal,1: 2-4.
8. Fock, K.M. and Ang, T.L. (2010) ʻʻ Epidemiology of Helicobacter pylori infection and gastric cancer in Asia,ʼʼ Journal of Gastroenterology and Hepatology, 25( 3) 479-86.
Publisher – Google Scholar
9. Garratty, G. Glynn, S.A and McEntire, R. (2004) ʻʻ ABO and Rh(D) phenotype frequencies of different racial/ethnic groups in the United States,ʼʼ Transfusion, 44 (5)703-706.
Publisher – Google Scholar
10. Iodice ,S. Maisonneuve, P. Botteri , E. Sandri, M.T. and Lowenfels, A.B. (2010) ʻʻABO blood group and cancer,ʼʼ Eur J Cancer, 46(18) 3345-3350.
Publisher – Google Scholar
11. Jackson, L. Britton, J. Lewis, S.A. McKeever, T.M. Atherton, J. Fullerton, D. et al. (2009) ʻʻA population-based epidemiologic study of Helicobacter pylori infection and its association with systemic inflammation, ʼʼ Helicobacter, 14(5) 108-113.
Publisher – Google Scholar
12. Kanbay, M. Gur, G. Arslan, H. Yilmaz, U. and Boyacioglu ,S. (2005) ʻʻThe relationship of ABO blood group, age, gender, smoking and Helicobacter pylori infection,ʼʼ Dig. Dis. Sci, 50 (7) 1214-1217.
Publisher – Google Scholar
13. Laheij, R.J. de Boer, W.A. Jansen, J.B. van Lier, H.J. Sneeberger, P.M. and Verbeek, A.L. (2000) ʻʻ Diagnostic performance of biopsy-based methods for determination of Helicobacter pylori infection without a reference standard,ʼʼ J. Clin .Epidemiol, 53(7) 742- 746.
Publisher – Google Scholar
14. Linde ‘N, S. Nordman, H. Hedenbro, J. Hurtig, M. BoreORE ‘N,T. and Carlstedt, I. (2002) ʻʻ Strain- and blood group—dependent binding of Helicobacter pylori to human gastric MUC5AC glycoforms,ʼʼ Gastroenterology, 123( 6) 1923—1930.
Google Scholar
15. Liu, H. Rahman, A. Semino-Mora, C. Doi, S. Q. and Dubois, A. (2008) ʻʻSpecific and sensitive detection of H. pylori in biological
Google Scholar
16. specimens by real-time RT-PCR and In situ hybridization,ʼʼ PLoS ONE, 3(7) 1-7.
17. Magalhães, Q.D. and Luzza, F. (2006) ʻʻ Epidemiology of Helicobacter pylori infection,ʼʼ Helicobacter, 1(11)1-5.
Publisher – Google Scholar
18. Martins, L.C. Corvelo, T.C.O. Oti, H.T. Loiola, R.S.P. Aguiar, D. C. F.; Barile, K.A.S. Amaral, R.K.C. Barbosa, H.P.M. Fecury, A.A. and de Souza, J.T. (2006) ʻʻABH and Lewis antigen distributions in blood, saliva and gastric mucosa and H. pylori infection in gastric ulcer patients,ʼʼ World J. Gastroenterol, 12 (7)1120-1124.
Google Scholar
19. Mattos, L.C. Cintra, J.R. Sanches, F.E. Alves, R.C. Ruiz, M.A. and Moreira, H.W.(2002) ʻʻ ABO, Lewis, secretor and non-secretor phenotypes in patients infected or uninfected by the Helicobacter pylori bacillus,ʼʼ Sao. Paulo. Med. J., 120 (2) 55-58.
Publisher – Google Scholar
20. Nakao, M. Matsuo, K. Ito, H.; Shitara, K. Hosono, S. Watanabe, M. Ito, S. Sawaki, A. Iida, S. Sato, S. Yatabe, Y. Yamao, K. Ueda, R. Tajima,K. Hamajima, N. and Tanaka, H. (2011) ʻʻABO genotype and the risk of gastric ancer, atrophic gastritis, and Helicobacter pylori nfection,ʼʼ Cancer Epidemiology, Biomarkers and Prevention, 20 (8) 1665-1672.
Publisher – Google Scholar
21. Ndip, R.N. Malange, E.A. Akoachere, T.K. MacKay, G.W. Titanji, K.P. and Weaver, T.L. (2004) ʻʻ Helicobacter pylori antigens in the faeces of asymptomatic children in the Buea and Limbe health districts of Cameroon: A pilot study,ʼʼ Trop. Med. Int. Health., 9 (9)1036-1040.
Publisher – Google Scholar
22. Niv, Y. Fraser, G. Delpre, G. and Neeman, A. (1996) ʻʻ Helicobacter pylori infection and blood groups,ʼʼ Am. J. Gastroenterol., 91(1) 101-104.
Google Scholar
23. Nwodo, E.N. Yakubu, S.E. Jatau ,E.D. and Yabaya , A. (2009) ʻʻSeroprevalence of Helicobacter pylori infection in patients with gastritis and peptic ulcer disease in Kaduna, Kaduna State, Nigeria,ʼʼ African Journal of Basic & Applied Sciences, 1(5-6) 123-128.
24. Petrovic, M. Artiko, V. Novosel, S. and Ille, T. (2011) ʻʻRelationship between Helicobacter pylori infection estimated by 14C-urea breath test and gender, blood groups and Rhesus factor,ʼʼ Hell. J. Nucl. Med.,14(1) 21-24.
25. Rasmi,Y. Sadreddini, M. Peirovi, T. Jamali, M. Khosravifar, F. Dadkhah, A. Fatemi, F. Rahmati, M. Zargari, M. and Sharifi, R.(2009) ʻʻ Frequency of ABO blood group in peptic ulcer disease in Iranian subjects,ʼʼ Pakistan J. Biol. Scien.,12 (13) 991-993.
Google Scholar
26. Ravn, V and Dabelstein, E. (2000) ʻʻThe ABO blood group system: historical background,ʼʼ Trans. Med.,11: 243-262.
27. Reid, M.E. and Bird, G.W. (1990) ʻʻ Associations between human red cell blood group antigens and disease,ʼʼTransfusion Med. Rev., 4(1) 47-55.
Publisher – Google Scholar
28. Seyda, T. Derya, C. Fusun, A. and Meliha, K.(2007) ʻʻThe relationship of Helicobacter pylori positivity with age, sex, and ABO/Rhesus blood groups in patients with gasterointestinal complaints in Turkey,ʼʼ Helicobacter, 12(3) 244-250.
Publisher – Google Scholar
29. Sharara, A. Abdul-Baki, H. El Hajj, L. Kreidielh, N.and Kfoury Baz, E.M.(2006) ʻʻAssociation of gasterodudenal disease phenotype with ABO blood group and Helicobacter pylori virulence specific serotypes,ʼʼ Dig. Liver Dis, 38: 829-833.
Publisher – Google Scholar
30. Thillainayagam, A.V. Arvind, A.S. Cook RS, Harrison, I.G.Tabaqchali, S. and Farthing, M.J. (1991) ʻʻDiagnostic efficacy of an ultra-rapid endoscopy room test for Helicobacter pylori,ʼʼ Gut, 32 (5) 467—469.
Publisher – Google Scholar