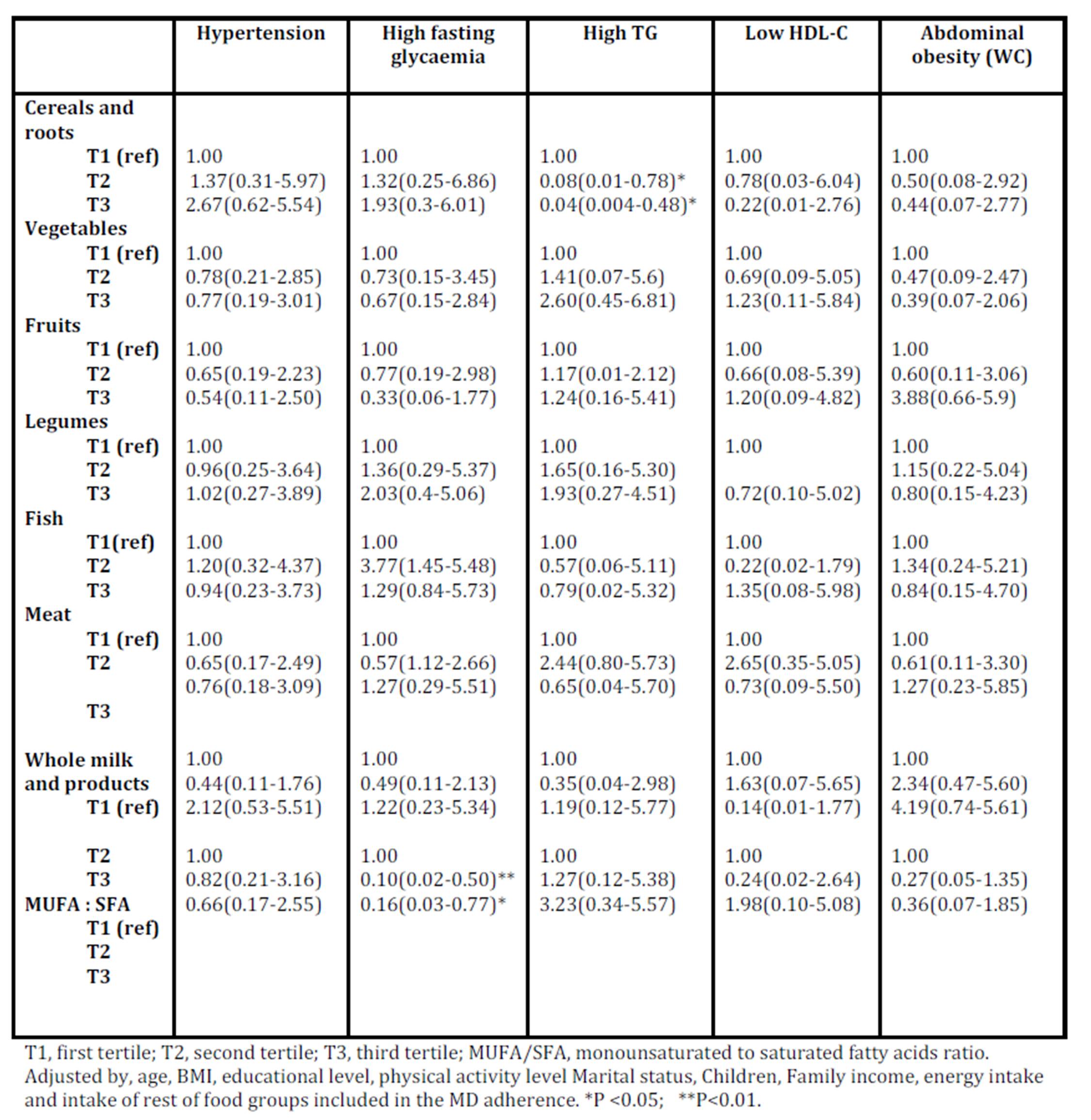
The association of the food items of the MD pattern with the five metabolic syndrome criteria prevalence was considered separately (table 7). Cereals intake and high mono-unsaturated to saturated fatty acids showed a protective effect on triglycerides criterion (p = 0.002) and on glycemia criterion (p = 0.02). No noticeable association was observed for the other metabolic syndrome criteria.
Discussion
The objective of the study was to assess the prevalence of MS in women population of Morocco, a Mediterranean country, in relationship with the adherence to Mediterranean diet. To the best of our knowledge, this study is the first one focusing on the possible relationship between the traditional Mediterranean diet (MD) and metabolic syndrome in the region. To better know the determinants of adherence of the women sample to the MD, the effect of the MD specific components is also discussed in this paper.
In Morocco, a developing country that is also experiencing demographic, health and nutrition transitions, few epidemiological studies have been conducted to characterize the magnitude of the prevalence of MS particularly in women; the importance of identifying women who are at risk of developing MS cannot be underestimated.
It is important to note that comparison of the prevalence of MS between studies is difficult, as different criteria are used and, most importantly, sex and age standardization is indispensable, that makes the comparison is not easy to make between published studies.
Although the prevalence of MS differs according to the criteria used to define it, it seems to affect around 25% of the population in developed countries (Alvarez Leon et al., 2003; Athyros et al., 2005). In this study, we used the National Cholesterol Education Program Adult Treatment Panel description of MS which is considered to be the most applicable tool for clinical and epidemiological practices (Isomaa et al., 2003).
Our findings on the prevalence of MS are quite similar to those previously reported in developed countries, indeed, one in every fifth adults presented MS in this population. This prevalence confirms the results of a cross-sectional survey conducted in 1995 in the same population about the magnitude of the prevalence of MS and association of BMI and WC with risk factors for cardiovascular diseases (Belahsen et al., 2005). This prevalence was also greater than that encountered by another study conducted in another region, the south of Morocco (Rguibi et al., 2004). Compared to the North Africa, MS is less prevalent than that observed in Tunisian women (Allal-Elasmi et al., 2010) or Algerian women (Biad et al., 2010) with significantly higher prevalence in women (37.3% and 27,1%) than in men(23.9% and 14,9%) (Bouguerra et al., 2007). It is also the case of the countries in Middle East where MS is among the major health problems testified by the abundant published literature. In Turkey, for instance, the prevalence of MS was estimated as 33.9% more marked in among women [39.6%] than men 28% (Kozan et al., 2007). In Saudi Arabia a prevalence of 13.6% comparable to that found in the present study was reported in adult females (Motlagh et al., 2009). In Oman, another country of the same region, the MS prevalence was estimated as 21.0%. In the same way, the prevalence of MS using the ATP III definition was reported to be 36.3% in a population of the Northern Jordan with higher rates in women than in men.
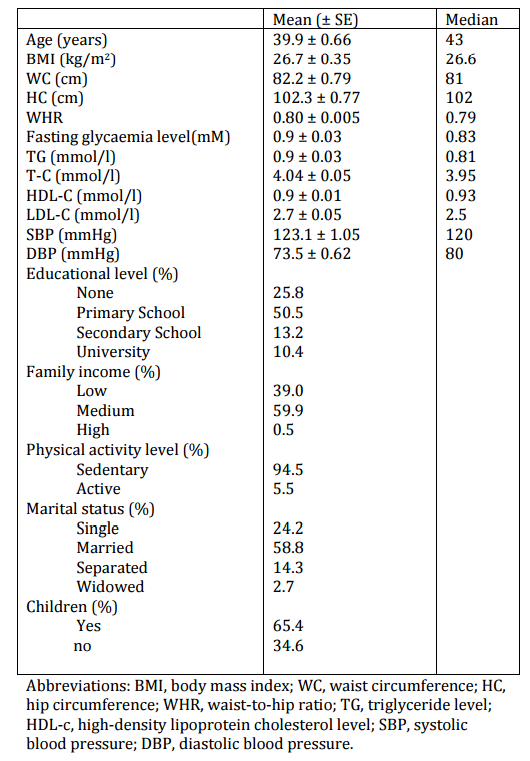
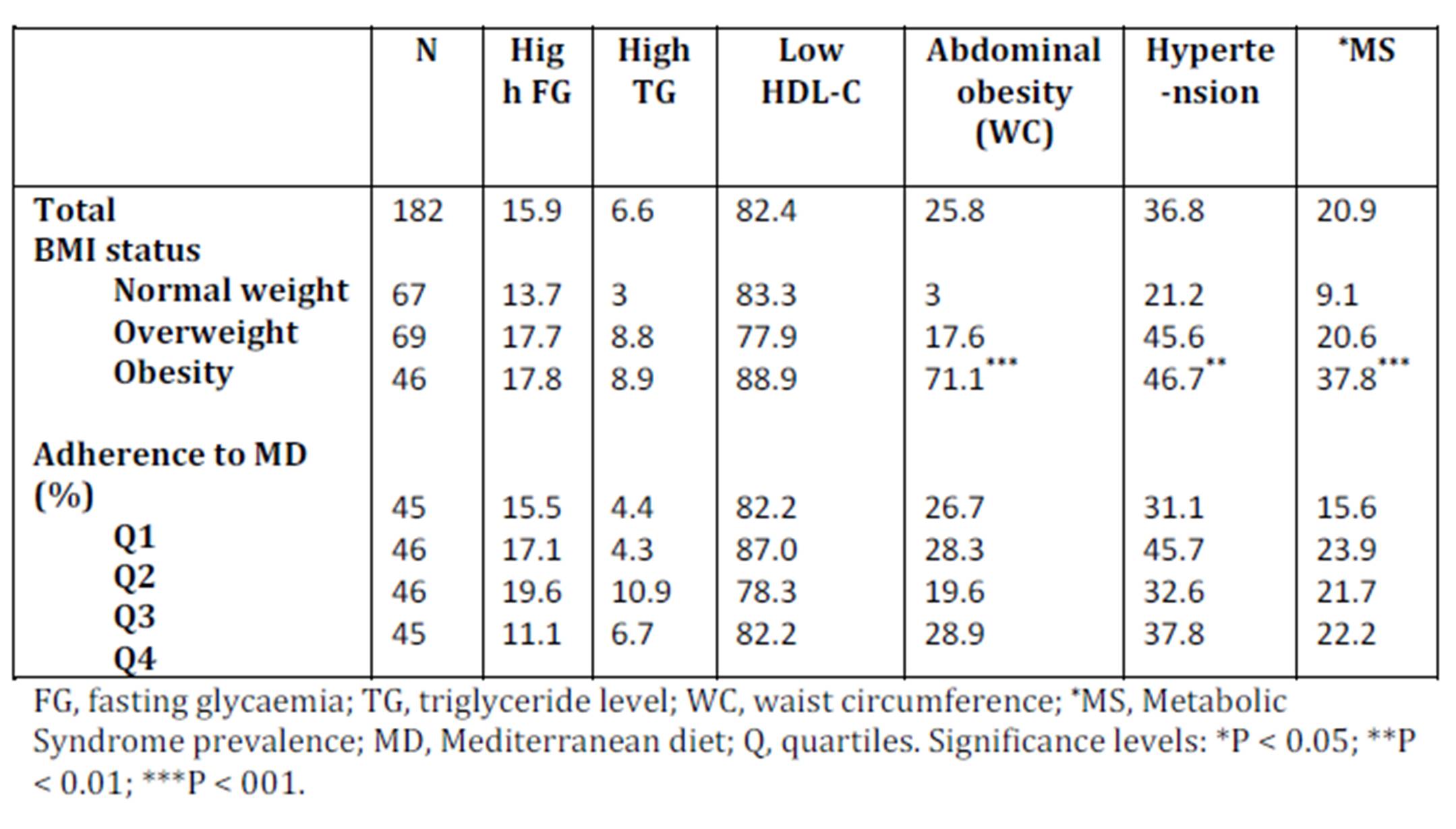
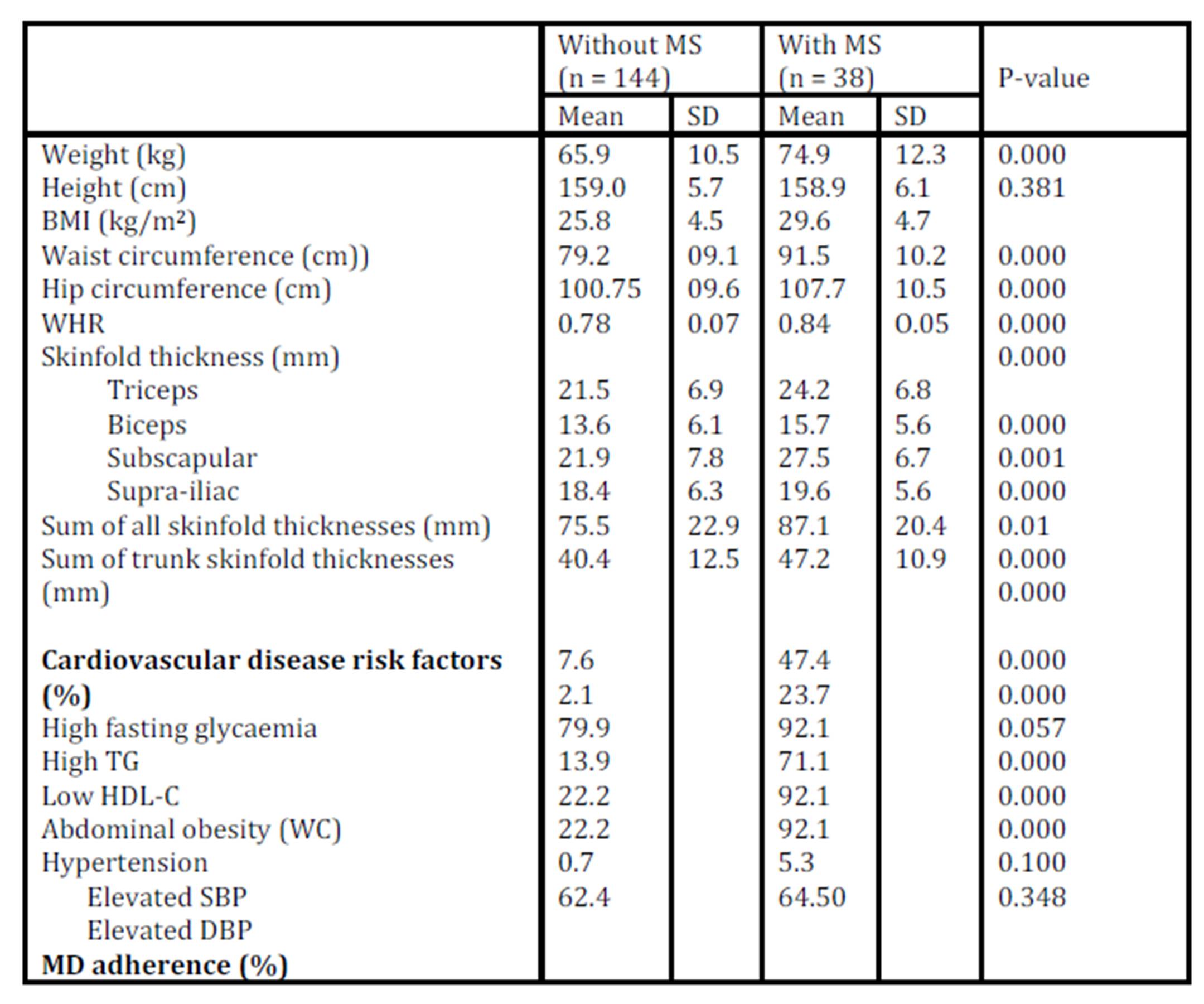
In this study, all anthropometric indices (BMI, WHR, Skinfold thickness and WC) provided useful information on metabolic risks. Comparative findings about the mean values of anthropometric variables of groups with and without MS can be explained by the recognized association between weight excess and body fat, and metabolic alterations (Oliveira et al., 2009). The proportion of women with ≥ 1 MS abnormalities (91.2%) suggests that each MS component worsens with obesity among women, and is in accordance with previous studies (Mar Bibiloni et al., 2011; Hillier et al., 2006). Low HDL-cholesterol level was the most commonly observed component of MS (82.4%) followed by Hypertension (36.8%), while high triglyceridemia was the least common (6.6%). The prevalence of MS factors in our population follows in part the pattern in developed countries when we stratified by the presence or absence of metabolic syndrome. There are discrepancies in literature about the prevalence of MS components. In developed countries, low HDL-cholesterol levels, and high triglyceridaemia and hypertension were the most common MS factors, whereas high fasting glycaemia was the least common (Do Carmo et al., 2008). In developing countries, high fasting triglyceridaemia was the most common MS factor, whereas low HDL-cholesterol level was the least common (Ebrahimpour et al., 2006).
Diet may also be one of the most important factors determinants of MS. The average adherence to the MDP was 62.84 % (± 12.7). The present study shows a low variability of the percentage of adherence to Mediterranean diet as reflected by the SD values.
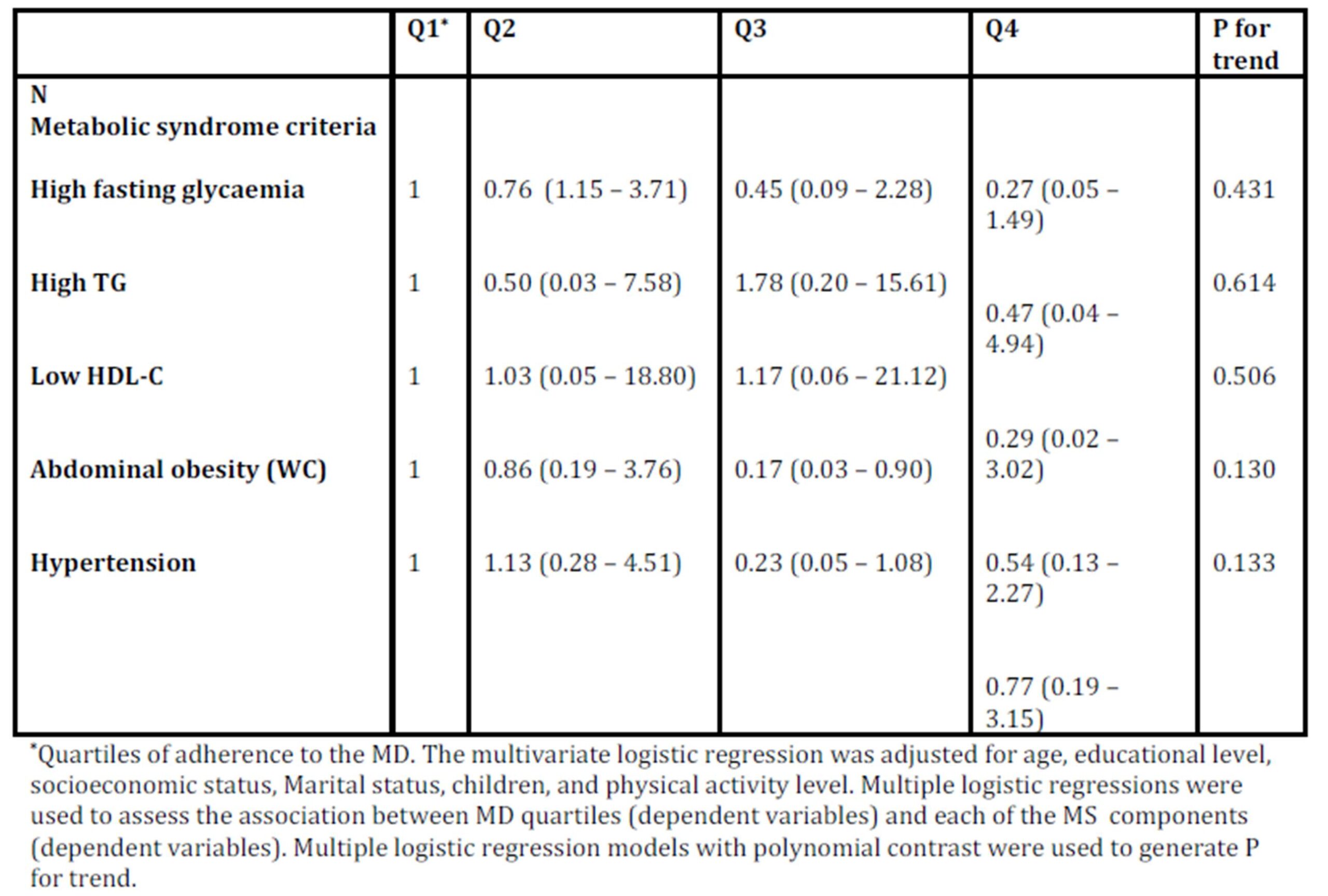
There was no association between the adherence to MD and the risk of metabolic syndrome, indicating that there is no protective effect of MD on the prevalence of MS in our study population. Several epidemiological studies have evaluated the role of the MD on the development or progression of the metabolic syndrome; and the association of the adherence to the MD with a beneficial effect on the MS was largely reported (Rumawas et al., 2009; Paletas et al., 2010), In the opposite, other studies in adults (Panagiotakos et al., 2004; Thanopoulou et al., 2006) found contradictory results or do not present a clear benefit of high adherence to MD in lowering prevalence of metabolic syndrome.
In the same way, this study shows that MS components were not significantly associated with adherence to the MDP, while several recent clinical trials demonstrated that adhering to MD has a beneficial effect on abdominal obesity (Romaguera et al., 2009), lipids levels (Tzima et al., 2007), glucose metabolism (Panagiotakos et al., 2007), and blood pressure levels (Estruch et al., 2006) and all the components of the MS, that are also risk factors for the development of cardiovascular disease, insulin resistance, and diabetes.
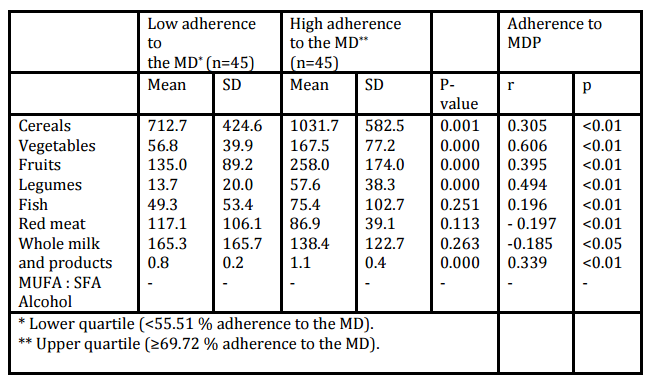
The multiple beneficial effects of the MD on the parameters of MS are also closely associated with its individual dietary components; in this context, the MS components risk was also evaluated by the MD pattern food groups. In our study, the food items associated with MD protective effect were higher MUFA /SFA for glycemia and higher cereals and roots for triglycerides.
The primary source of MUFA is olive oil; it’s one of the most representative and central food of traditional MD. In the study subjects; this food represents 17.6 % of the fats and oils food group which explains the ratio MUFA/SFA of 1.02 ± 0.35. In Morocco; olive oil is used abundantly as a culinary fat. A recent review demonstrated its beneficial effects of MD on lowering blood pressure, reducing plasma glucose, and improving the cholesterol/HDL ratio and endothelial function (Lopez-Miranda et al., 2010). It is also to be noted that in our study, even not significant, high intakes of MUFA/SFA, Fruits, Vegetables and Fish were associated with lower risk of blood pressure criterion. Polyphenols and flavonoids present in fruits and vegetables, Intake of fish oil N-3 fatty acids have also been shown to decrease plasma triglycerides and blood pressure (Perez-Vizcaino et al., 2009; Duda et al., 2009).
The protective effect of the MD on triglycerides was mediated by higher cereals and roots food items and their known beneficial effect on lipid metabolism due to their water-soluble fiber content (Brown et al., 1999). In our study population, there’s a large intake of cereals and roots (696.4 g day-1); The effect of fiber on plasma triacylglycerol is mainly from such gel-forming fiber which influences the functional properties of the intestinal mucosa by slowing upper intestinal transit, as a result, the intestinal absorption of dietary lipids may impair (Topping et al., 1988).
The study reports also no protective effect of cereals intake on glycemia. Some studies have reported an association of high cereal intake with a lower prevalence of the glycaemic and even insulin resistance criterion. In this study, subjects with cereal intake >150 g day-1 presented half the risk of hyperinsulinemia than subjects with lower intakes. This effect could be explained in part by those foods fiber content, resulting in a lower rate of gastric emptying and an increased satiation (Delzenne et al., 2005).
The results of our analysis showed an association between some life-style characteristics and the adherence to a global MDP. Many studies have associated socioeconomic characteristics and life-styles with the adherence to several population dietary patterns (Sanchez-Villegas et al., 2002; Whichelow et al., 1996; Martinez et al., 2010) but to our knowledge this is the first time that the factors associated with the adherence to MDP have been analyzed in this population. Our subjects belong to a population stratum with a medium education level (half of the population has a primary school education level); there was a direct association between adherence to the MDP and women education level. The latter was reported to have marked effect on family lifestyles and dietary habits (Do Carmo et al., 2008). Nowadays, mothers are still in charge of the home dieting in the Moroccan population, and the mother education level is one of the best predictors of the family diet quality. The present results are also in agreement with previous studies carried out in Spanish adults (Moreno et al., 2002; Tur et al., 2004) suggesting a direct association between low education level and low fruits and vegetables’ consumption..
On average, higher socioeconomic level, defined by education level, has been associated with the adherence to a healthier dietary pattern (Fraser et al., 2000); however, Family income, another direct indicator of socioeconomic level, was not significantly linked to greater or lower adherence to the MD in the present study; this reinforces again the influence of education level especially in terms of food intake behaviour.
Contrary to other investigations, we have not been able to determine the number of women smokers because they do not want to respond to this issue probably for social and culture considerations. It was reported that smoking is positively associated with unhealthy dietary habits (lloveras et al., 2001) and negatively associated with high adherence to the traditional MDP (Martinez-Gonzalez et al., 1997).
We have also considered that Mediterranean lifestyle includes the regular practice of physical activity. In our study, despite a high rate of physical inactivity (94%), an inverse relation can be observed between physical activity during leisure-time and low adherence to the MD, although this difference is not statistically significant; the beneficial effect attributed to the MD against CHD and other related diseases could not be a result of diet only, but also in part to a more active life-style during leisure time of those who adhere to the traditional Mediterranean diet, this association has also been observed in previous studies (Sanchez-Villegas et al., 2002; Martinez et al., 2010; Mariscal-Arcas et al., 2007). Besides, epidemiological evidence supports a detrimental role of sedentary lifestyles on increasing obesity epidemic in Mediterranean countries (Martınez-Gonzalez et al., 2001).
Having children, marital status represents another social dimension, as dietary habits could be influenced by living arrangement. Women not living with spouse tend to have nutritional deficiency of iron, vitamin D and lower consumption of vegetables and fish. It is possible that they pay less attention to meal preparation. Other possible explanations are the low income, or lower education level in these women. Numerous studies have shown that married persons have lower risk of mortality, and enjoy better physical and mental health than their unmarried counterparts (Hu et al., 1990). Moreover, marital termination by death or divorce has been prospectively linked to decline in health and increased mortality risk, with more pronounced effects among men (Ebrahim et al., 1995; Stroebe et al., 1983).
To sum up, MS is prevalent among the study population, especially among obese women. These findings demonstrate an emerging health problem in Morocco because of the number of overweight and obese women that are likely to develop MS. Some components of the MD showed a protective effect on some MS components; however, no association was found between MS and adherence to MD. High education level, increased physical activity level and availability of family environment were also related to a better adherence to MD pattern.
Study Limitations
The key limitations of this study are the small sample size of this work. Furthermore, adherence to the MD was relatively uniform with low variability among the subjects, since the diets of the subjects are not largely different and remained relatively similar. Another concern is that adherence to the MD was determined only from dietary data collected over a few months (between September and December); it is possible that some subjects changed their diet over the many years required for MS to develop. It’s for this reason that we chose subjects who are not taking medication or recently changed their diet on the recommendation of their physician because of the detection of abnormalities (e.g., hypertension) linked to MS.
Conclusion
The present study demonstrates that despite the uniformity of the adhesion of the population to the MD that is the original Moroccan diet, there is an absence of its effect on the MS. The effect is still present in some components of MD, which shows an increasing abandonment of this diet that it is replaced by the nutrition transition that crosses Morocco. MD is often lost regardless of age and income, especially among people with low education and physical activity, living alone and having no children. These groups should be targeted for intervention strategies to deviate the development of detrimental mechanisms involved in the genesis of the synergistic effects of MS components, and to slow down the effects of nutrition transition that is the major source of alteration of the traditional MD pattern considered as the original diet in Morocco.
Acknowledgements
This study has been carried out with the financial support (Joint grant) of INSERM (Institut National de la Santé et de la Recherche Medicale, France) and CNCPRST (Centre National de Coopération et de Recherche Scientifique, Morocco).
References
1. Allain, C.C., Poon, L.S. , Chan, C.S., Richmond, W. and Fu, P.C. (1974) “ Enzymatic determination of total serum cholesterol” Clin. Chem, 20 (4) 470—475.
2. Allal-Elasmi, M., Haj Taieb, S., Hsairi, M., Zayani, Y., Omar, S. , Sanhaji, H., Jemaa, R., Feki, M., Elati, J., Mebazaa, A. and Kaabachi, N. (2010) “The metabolic syndrome: prevalence, main characteristics and association with socio-economic status in adults living in Great Tunis” Diabetes Metab, 36 (3) 204-8.
Publisher – Google Scholar
3. Alvarez Leon, E.E., Ribas Barba, L. and Serra Majem, L. (2003) “Prevalence of the metabolic syndrome in the population of Canary Islands, Spain” Med Clin (Barc), 120 (5) 172—174.
Google Scholar
4. ANAES (Agence Nationale d’Accréditation et d’Evaluation en Santé). (2000) Modalités de dépistage et diagnostic biologique des dyslipidémies en prévention primaire.
5. Athyros, V.G., Ganotakis, E.S., Elisaf, M. and Mikhailidis, D.P. (2005) “The prevalence of the metabolic syndrome using the National Cholesterol Educational Program and International Diabetes Federation definitions” Curr Med Res Opin, 21 (8) 1157—1159.
Publisher – Google Scholar
6. Bach-Faig, A. , Berry, E. M. , Lairon, D. , Reguant, J. , Trichopoulou, A. , Dernini, S., Medina, F. X., Battino, M., Belahsen, R., Miranda G. and Serra-Majem, L. (2011) ” on behalf of the Mediterranean Diet Foundation Expert GroupMediterranean. diet pyramid today. Science and cultural updates,” Public Health Nutrition, 14 (12A) 2274—2284.
Publisher – Google Scholar
7. Belahsen, R., Bermudez, O.I., Mziwira, M., Fertat, F., Newby, P.K. and Tucker, K.L. (2005) “Obesity and related metabolic disorders are prevalent in Moroccan women of child-bearing age,” International Journal of Diabetes & Metabolism, 13 (3) 159—66.
8. Biad, A., Chibane, A., Makhlouf, L., Atif, A., Lanasri, L. , Kessous, L. (2010) “The Prevalence of the Metabolic Syndrome in East of Algiers” Journal of Hypertension, 28, 133.
9. Bouguerra, R., Alberti, H. , Smida, H., Salem, L.B., Rayana, C.B., El Atti, J., Achour, A., Gaigi, S., Slama, C.B. , Zouari, B. and Alberti, K.G. (2007) “Waist circumference cut-off points for identification of abdominal obesity among the Tunisian adult population” Diabetes Obes Meta, 9 (6) 859—68.
Publisher – Google Scholar
10. Brown, L., Rosner, B., Willett, W.W.and Sack, F.M. (1999) “Cholesterol-lowering effects of dietary fiber: a meta-analysis” Am J Clin Nutr, 69 (1) 30—42.
11. Buckland, G., Salas-Salvado, j., Roure, E., Bullo, M. and Serra-Majem, L. (2008) ”Sociodemographic risk factors associated with metabolic syndrome in a Mediterranean population,” Public Health Nutr, 11 (12) 1372—1378.
Publisher – Google Scholar
12. Day, C. (2007) “Metabolic syndrome, or What you will: definitions and epidemiology,” Diab Vasc Dis Res, 4, (1) 32— 38.
Publisher – Google Scholar
13. Delzenne, N.M. and Cani, P.D. (2005) “A place for dietary fibre in the management of the metabolic syndrome”Current Opinion in Clinical Nutrition Metabolic Care, 8 (6) 636—40.
Publisher – Google Scholar
14. Do Carmo, I. , Dos Santos, O., Camolas, J., Vieira, J. , Carreira, M., Medina, L., Reis, L., Myatt , J. and Galvão-Teles, A. ( 2008) “Overweight and obesity in Portugal: national prevalence in 2003-2005” Obes Rev, 9 (1) 11—19.
15. Duda, M.K., O’Shea, K.M.and Stanley, W.C. (2009) “Omega-3 polyunsaturated fatty acid supplementation for the treatment of heart failure: mechanisms and clinical potential” Cardiovasc Res, 84 (1) 33-41.
Publisher – Google Scholar
16. Ebrahim, S., Wannamethee, G. and McCallum A. (1995) “Marital status, change in marital status, and mortality in middle-aged British men” Am J Epidemiol, 142 (8) 834—42.
17. Ebrahimpour, P., Fakhrzadeh, H., Pourebrahim, R. , Hamidi, A. and Larijani, B. (2006) ” Metabolic syndrome and related insulin levels in obese children” Metab Syndr Relat Disord, 4 (3) 172-8.
Publisher – Google Scholar
18. Estruch, R., Martinez-Gonzalez, M.A. and Corella D. (2006) “Effects of a Mediterranean-style diet on cardiovascular risk factors: a randomized Trial” Ann Intern Med, 145 (1) 1—11.
Publisher – Google Scholar
19. Fossati, P. and Prencipe, L. (1982) “Serum triglycerides determined colorimetrically with an enzyme that produces hydrogen peroxide” Clin. Chem, 28 (10) 2077—2080.
20. Fraser, G.E., Welch, A., Luben, R., Bingham, S.A. and Day N.E. (2000) “The effect of age, sex, and education on food consumption of a middle-aged English Cohort-EPIC in East Anglia” Prev Med, (30) 26—34.
21. Friedewald, W.T., Levy, RI. and Fredrickson, DS. (1972) ” Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge” Clin. Chem, 18 (6) 499—502.
22. Giugliano, D. and Esposito, K. (2008) “Mediterranean diet and metabolic diseases,” Curr Opin Lipidol, 19 (1) 63-68.
23. Harris, N., Galpchian V. and Rifai, N. (1996) ” Three routine methods for measuring high-density lipoprotein cholesterol compared with the reference method” Clin. Chem, 42 (5) 738—743.
24. Hillier, T.A., Fagot-Campagna, A., Eschwege, E., Vol, S., Cailleau, M. and Balkau, B. (2006) “Weight change and changes in the metabolic syndrome as the French population moves towards overweight: The DESIR cohort” Int J Epidemiol, 35 (1) 190—196.
Publisher – Google Scholar
25. Hu, Y. and Goldman, N. (1990) “Mortality differentials by marital status: an international comparison” Demography, 27 (2) 233—50.
Publisher – Google Scholar
26. Isomaa, B. (2003) “A major health hazards: the metabolic syndrome” Life Sciences, 73 (19) 2395—411.
Publisher – Google Scholar
27. Kastorini, C.M., Milionis, H.J., Esposito, K., Giugliano, D. , Goudevenos, J.A. and Panagiotakos, D.B. (2011)
“The effect of Mediterranean diet on metabolic syndrome and its components” J Am Coll Cardiol, 57 (1) 1299-313.
Publisher – Google Scholar
28. Katsimabros, N. (2006) “Epidemiological evidence for the non-random clustering of the components of the metabolic syndrome: multicentre study of the Mediterranean group for the study of diabetes“ Eur J. Clin Nutr, 60 (12) 1376-1383.
Publisher – Google Scholar
29. Kouris-Blazos, A., Gnardellis, C., Wahlqvist, M.L., Trichopoulos, D., Lukito, W. and Trichopoulou, A. (1999) “Are the advantages of the Mediterranean diet transferable to other populations? A cohort study in Melbourne, Australia” BJN, 82 (1) 57—61.
30. Kozan, O., Oguz, A., Abaci, A., Erol, C., Ongen, Z., Temizhan, A. and Celik, S. (2007) “ Prevalence of the metabolic syndrome among Turkish adults” Eur J Clin Nutr, 61 (4) 548—53.
31. Lasheras, C., Fernandez, S. and Patterson, A.M. (2000) “Mediterranean diet and age with respect to overall survival in institutionalized, nonsmoking elderly people” Am J Clin Nutr, 71 (4) 987—992.
32. Lloveras, G., Ribas-Barba, L. and Ramon, J.M. (2001) “Relacion del consumo de alimentos y nutrientes con el habito tabaquico (Food consumption and nutrient intake in relation to smoking)” Med Clin (Barc) 116 (4) 129—132.
Publisher – Google Scholar
33. Lopez-Miranda, J., Perez-Jimenez, F., Ros, E. and De Caterina, R. (2010) “Olive oil and heatlh: Summary of the II international conference on olive oil and health consensus report, Jaen and Cordova (Spain) 2008” Review Nutr Met Cardiovasc Dis, 20 (4) 284-294.
Publisher – Google Scholar
34. Mar Bibiloni, M., Martínez, E., Llull, R., Maffiotte, E., Riesco, M., Llompart, I., Pons, A. and Tur, J.A (2011)
“ Metabolic syndrome in adolescents in the Balearic Islands, a Mediterranean region” Nutr Metab Cardiovasc Dis, 21 (6) 446-54.
Publisher – Google Scholar
35. Mariscal-Arcas, M., Romaguera, D. and Rivas, A. (2007) “Diet quality of young people in southern Spain evaluated by a Mediterranean adaption of the diet quality index-international (DQI-I)” Brit J Nutr, 98 (6) 1267—1273.
36. Martinez, E., Llull, R., Del Mar Bibiloni, M., Pons, A. and Tur, J.A. (2010) “Adherence to the Mediterranean dietary pattern among Balearic Islands adolescents” Br J Nutr, 103 (11) 1657-64.
37. Martinez-Gonz alez, M.A., Perez-Gutierrez, R., Martinez-Gonzalez, J., Garcia- Martin, M. and Bueno-Cabanillas, A. (1997) “Dietary intake of some food items in smokers and non-smokers in a Mediterranean population” Eur J Public Health, 7 (1) 40—44.
38. Martınez-Gonzalez, M.A., Varo, J.J., Santos, J.L., De Irala-Este´vez, J., Gibney, M. and Kearney, J. (2001) “Prevalence of physical activity during leisure time in the European Union” Med Sci Sports Exerc, 33 (7) 1142—1146.
39. Mirmiran, p., Noori, N. and Azizi, F. (2008) “ A prospective study of determinants of the metabolic syndrome in adults,” Nutr Metab Cardiovasc Dis, 18 (8) 567—573.
40. Moreno, L.A., Sarrıa, A. and Popkin, B.M. (2002) “The nutrition transition in Spain: a European Mediterranean country” Eur J Clin Nutr, 56 (10) 992—1003.
41. Motlagh, B. , O’Donnell, M., Yusuf, S. (2009) “Prevalence of cardiovascular risk factors in the Middle East: A systematic review” Eur J Cardiovasc Prev Rehabil, 16 (3) 268—80.
Publisher – Google Scholar
42. National Cholesterol Education Program. (2001) Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA, 285, 2486—2497.
43. National Institute of Health. (2002) Third Report of the National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). National Institute of Health. NIH publication No. 02-5215. Available at: http://www.nhlbi.nih.gov/guidelines/cholesterol/ atp3full.pdf.
44. Olinto, M.T., Nacul, L.C., Gigante, D.P., Costa, J.S., Menezes, A.M. and Macedo, S. (2003) “Waist circumference as a determinant of hypertension and diabetes in Brazilian women: a population-based study,” Public Health Nutrition, 7 (5) 629—635.
45. Oliveira, R.M. , Franceschini Sdo, C., Rosado, G.P. , Priore, S.E. (2009) “Influence of prior nutritional status on the development of the metabolic syndrome in adults” Arq Bras Cardiol, 92 (2) 101-12.
46. Paletas, K., Athanasiadou, E., Sarigianni, M. , Paschos, P., Kalogirou, A., Hassapidou, M. and Tsapas, A. (2010) “The protective role of the Mediterranean diet on the prevalence of metabolic syndrome in a population of Greek obese subjects” J Am Coll Nutr, 29 (1) 41-45.
47. Panagiotakos, D.B., Tzima, N. and Pitsavos C. (2007) ”The association between adherence to the Mediterranean diet and fasting indices of glucose homoeostasis: the ATTICA study” J Am Coll Nutr, 26 (1)32— 8.
48. Panagiotakos, D.B., Pitsavos, C., Chrysohoou, C., Skoumas, J., Tousoulis, D., Toutouza, M., Toutouzas, P. and Stefanadis, C. (2004) ”Impact of lifestyle habits on the prevalence of the metabolic syndrome among Greek adults from the ATTICA study” Am Heart J, 147 (1) 106-12.
49. Perez-Vizcaino, F. , Duarte, J., Jimenez, R., Santos-Buelga, C. and Osuna, A. (2009) “Antihypertensive effects of the flavonoid quercetin” Pharmacol Rep, vol. 61 (1) 67-75.
50. Rguibi, M., Belahsen, R. (2004) “Metabolic syndrome among Moroccan Sahraoui adult women” Am J Human Biol, 16 (5) 598—601.
51. Romaguera, D., Norat, T. and Mouw, T. (2009) “Adherence to the Mediterranean diet is associated with lower abdominal adiposity in European men and women” J Nutr, 139 (9) 1728 —37.
52. Rumawas, M.E., Meigs, J.B., Dwyer, J.T., McKeown, N.M. and Jacques, P.F. (2009) “Mediterranean-style dietary pattern, reduced risk of metabolic syndrome traits and incidence in the Framingham Offspring Cohort” Am J. Clin Nutr, 90 (6) 1608-1614.
53. Sanchez-Villegas, A., Martinez, J.A., De Irala, J. and Martinez-Gonzalez, M.A. (2002) “Determinants of the adherence to an a priori defined Mediterranean dietary pattern” Eur J Nutr, 41 (6) 249—257.
54. Sofi, F., Cesari, F., Abbate, R., Gensini, G. F. and Casini, A. (2008) “ Adherence to Mediterranean diet and health status: meta-analysis,” BMJ, 337, 1344.
55. Stroebe, M.S. and Stroebe, W. (1983) “Who suffers more? Sex differences in health risks of the widowed” Psychol Bull, 93 (2) 279—301.
56. Sugiuchi, H., Uji, Y., Okabe, H., Irie, T., Uekama, K., Kayahara, N. and Miyauchi, K. (1995) ”Direct measurement of high-density lipoprotein cholesterol in serum with polyethylene glycol-modified enzymes and sulfated alpha-cyclodextrin” Clin. Chem, 41 (5) 717—723.
57. Takahashi, M. M., De Oliveira, E. P., de Carvalho, A. L., Dantas, LA., Burini, F. H., Portero-McLellan, K. C. and Burini, R. C. (2011) “Metabolic Syndrome and dietary components are associated with coronary artery disease risk score in free-living adults: a cross-sectional study,” Diabetol Metab Syndr, 3-7.
58. Thanopoulou, A., Karmananos, B., Angelico, F., Assaad-Kahalil, S., Djordjevic, P. and Topping, D.L. , Oakenfull, D., Trimble, R.P. and Illman, R.J. (1988) “A viscous fibre (methylcellulose) lowers blood glucose and plasma triacylglycerols and increases liver glycogen independently of volatile fatty acid production in the rat” Br J Nutr, 59 (1) 21-30.
59. Trichopoulou, A., Kouris-Blazos, A. , Wahlqvist, M.L., Gnardellis, C., Lagiou, P., Polychronopoulos, E., Vassilakou, T., Lipworth, L. and Trichopoulos, D. (1995) “Diet and overall survival in elderly people” BMJ, 311, 1457—1460.
60. Trichopoulou, A., Lagiou, P. and Trichopoulos, D. (1994) “Traditional Greek diet and coronary heart disease” J Cardiovascular Risk, 1, 9-15.
61. Tur, J.A., Romaguera, D. and Pons, A. (2004) “Adherence to the Mediterranean dietary pattern among the population of the Balearic Islands” Brit J Nutr, 92 (3)341—346.
62. Tzima, N., Pitsavos, C. and Panagiotakos, D.B. (2007) “Mediterranean diet and insulin sensitivity, lipid profile and blood pressure levels, in overweight and obese people; the Attica study” Lipids Health Dis, 19, 6-22.
63. Whichelow, M.J. and Prevost, A.T. (1996) ”Dietary patterns and their associations with demographic, lifestyle and health variables in a random sample of British adults” Br J Nutr, 76 (1) 17—30.
64. Willett, WC. (1994) “Diet and health: What should we eat?” Science, 264 (5158) 532 —537.
65. Wood, D. (2001) “Established and emerging cardiovascular risk factors,” Am Heart J, 141 (2) 49-57.
66. World Health Organization. (1998) Obesity: Preventing and managing the Global Epidemic – Report of a WHO Consultation on Obesity, 3-5 June 1997; Geneva, WHO/NUT/NCD/98.1.
67. World Health Organization. (2003) Diet, Nutrition and the Prevention of Chronic Disease. Report of a Joint WHO/Food and Agriculture Organization Expert Consultation, WHO Technical Report Series No. 916. Geneva