Patients who left without being seen (LWBS) by a physician from a pediatric emergency department (ED)/urgent care (UC) center have become a serious challenge facing emergency medicine practitioners. The rate at which patients LWBS may serve as an indicator of patient dissatisfaction and sub-optimal healthcare quality. Numerous studies by Pham (2009), Polevoi (2005) and Hobbs (2000), have been published that describe factors associated with ED patients that LWBS. However, Burgeois (2008) mentioned that few of these studies have focused on pediatric patients. Studies thus far, have attempted to quantify waiting time, chief complaint acuity, health risks, hospital factors, medical-legal issues, and ways to keep patients from leaving. However, studies which analyze the costs and other financial implications of pediatric patients who LWBS from the ED/UC, including lost charges, are scarce.
The main objective of this study was to estimate the amount of lost billable charges as a result of pediatric patients who LWBS from the ED/UC. A retrospective study was designed to contact parents/caretakers of pediatric patients who LWBS over a one year period. We estimated the lost charges based on an analysis of hospital charges and physicians’ charges.
Methods
This population-based retrospective study was conducted in a single academic, tertiary care, urban children’s hospital’s ED/UC that treats approximately 65,000 patients annually. Patients are triaged according to acuity of symptoms. The ED sees approximately 37,000 patients, while the UC treats 28,000 patients. The majority of patients seen at this children’s hospital are of Hispanic/Latino decent. Each patient that arrived with a caretaker was assessed by the ED nurse screener, and was then triaged appropriately. None of the subjects who LWBS were encouraged to leave from triage, as the hospital policy is to have all presenting patients assessed by a physician before leaving. This research protocol was approved by the hospital’s Institutional Review Board (IRB) prior to its initiation. The study period began November 1, 2009 and ended October 31, 2010. During this period a total of 1,193 patients were recorded as LWBS, and contact was attempted in order to gather follow-up information from parents/caregivers. The inclusion criteria consisted of any parent/caretaker of a patient who LWBS from the ED/ UC during the study period. Patients were excluded if they could not be reached via telephone, or if they were examined by a physician before leaving the ED/UC.
Interview Process and Data Collection
Three trained interviewers made up to 3 attempts to contact each subject over a 1 week period. The follow up phone call was made over a time period of 3-12 months after the patient visit. Background information for the study was communicated to the subjects, and verbal consent was obtained for study enrollment according to IRB procedures. English speaking participants, or those with an English-speaking adult available to speak to the investigator at the time of the interview were surveyed. Spanish only speakers who did not have an adult available to translate were contacted again by an investigator who was a native Spanish speaker. No respondents were excluded due to language barriers.
The interview was then conducted by 1 member of the study team, either the Principal Investigator (PI) or 1 of 2 research assistants. During the telephone interviews, 19 questions were posed to study participants over a period of 10 to 15 minutes. The answers were recorded onto a data sheet designed for the study. Upon completion of the interview, the PI or research assistant gathered 3 more data points from the medical record; type of insurance, number of previous and subsequent visits to the study hospital, and past payment history.
The interview consisted of questions pertaining to the following items: whether the patient saw a doctor at the study hospital (to confirm the subject’s status as a patient who LWBS), chief complaint, area of the ED/UC from which the patient left, length of waiting time prior to LWBS, number of other children cared for by the respondent, whether the subject would or did return to the study hospital for care after the LWBS visit, whether the subject had a prior physician encounter elsewhere before coming to the study hospital, whether the subject sought care elsewhere after LWBS, availability of discharge papers from the other facility (if applicable), whether any tests were performed at the subsequent visit (x-rays, blood, or urine, if applicable), whether the subject received a bill from that visit, what the hospital could have done that would have prevented the patient to be LWBS, the child’s date of birth (DOB), whether the patient has a primary care physician (PCP), if the patient was well at the time of the survey, and if they were given a final diagnosis from another treatment facility.
Hospital Charges/Physician Charges
The projected lost charges for each visit were extrapolated in 1 of 2 ways. If the patient received subsequent care after they LWBS and was given a final diagnosis elsewhere, this was used to estimate the projected cost of the visit. If no care was sought after leaving the study hospital, then the chief complaint was used to estimate the cost of the visit. Projected lost charges were based on established codes, hospital charges, and physician fees. Based on these reported diagnoses, or chief complaints, the potential charges for each visit were calculated.
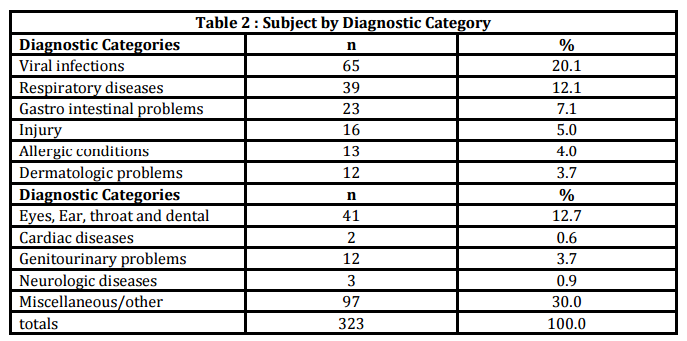
Each diagnosis or chief complaint was assigned a hospital charge by the international classification of diseases (ICD) code as listed by the hospital’s billing and coding personnel. Data from the 2010 fiscal year were used to calculate the hospital charges. The physician visit charges were assigned a current procedural terminology (CPT) billing code charge by the level of complexity of each diagnosis or chief complaint. The physician investigator assigned these codes based on figures for ED/UC visits for the 2010 fiscal year. Each diagnosis or chief complaint reported by the subjects during the phone interview was entered into 1 of 11 investigator-defined diagnostic categories. The chief complaint was used to estimate charges for patients who did not complete the telephone interview, but LWBS during the study time period. The total lost billable charges were then tabulated and analyzed.
Results
From November 1, 2009 to October 31, 2010 a total of 63,629 patients were registered to be seen in the ED/UC. Of these patients, there were 1,193 (1.87%) who LWBS. A total of 359 (30%) individuals were contacted successfully. Of those, 323 (90%) consented to participate in the interview and 36 subjects (10%) declined. The first attempt to contact the caretaker/parent was generally the most successful. There were 834 (70%) individuals that were unable to be contacted successfully. This was most commonly due to a disconnected phone number, or the number called belonged to someone other than the patient’s caretaker.
The patients who LWBS had a wide range of chief complaints. The most commonly reported chief complaint was fever (n =109) followed by vomiting (n =23), cough (n =22), abdominal pain (n =14) and earache (n= 14). The remainder of the patients had a chief complaint that was reported by less than 8 patients for each complaint. During the telephone interviews the respondents were asked several questions related to the medical visit as listed in Table 1.
Additionally, 248 (77%) respondents stated they left from the waiting room, while 51 (16%) said they left from a patient room. The median time reported that they waited without being seen was 2.79 hours, and the long wait time was the most common reason parents/caretakers decided to leave.
Our findings demonstrate that the lost charges for patients who LWBS were significant. When the data was extrapolated from our findings to include all LWBS patients for the study period, the total lost charges during the 1-year study period were quite substantial.
Patients who LWBS after presenting to the ED/UC and then LWBS represent a significant problem of lost charges for many pediatric EDs around the country. Pham (2009) reported that published estimates of LWBS rates from single site institutions vary widely. However, recently published national studies by Sun (2007) and Bourgeois (2008), suggest an average rate of patients who LWBS. This national LWBS rate was affected by the various patient, visit, and institutional characteristics. The study conducted by Bourgeois (2008), stated that on average nationally, 2.46% of pediatric patients presenting to pediatric EDs LWBS. While our hospital had a lower rate than the national average, an estimated loss of over $1 million dollars occurred. It should be noted, however, that the collection rate for the hospital during the study time period was 87%, so while we estimated the charges based on a 100% collection rate, in reality we may have collected less based upon our collection rate during this period.
During the survey, parents/caretakers were asked if they had seen a physician prior to coming to the hospital with the patient. A very small percentage of the respondents said they had been seen prior, however, most of the respondents also stated that they do have a PCP for their child. While it remains unclear why parents/caretakers brought the patient to the ED/UC instead of their PCP, this also contributed to the high volume of ED/UC patients. There is a possibility that obtaining appointments with their PCP could be difficult, or that patients perceive the ED/UC as a comprehensive care facility equipped with laboratory and x-ray capabilities. Ultimately, this more than likely contributed to the high volume of patients, which resulted in increased wait times and more patients who LWBS, and therefore more lost revenue. Only about two thirds of the respondents sought medical care elsewhere after they LWBS. Almost all the patients were doing well at the time of the interview. Very few had any diagnostic studies performed when they were subsequently seen by a provider. This indicates that the patients’ acuity was unlikely to be high at the time they LWBS. Previous studies by Goldman (2005), Rowe (2006) and Kronfol (2006) found that most patients who LWBS are low acuity and are not “sick enough to warrant admission elsewhere.” Therefore, the lost billable charges for those patients are likely to be at low levels of reimbursement.
Limitations
Our study consisted of a convenience sample of parents and caregivers. While our response rate was somewhat low, a previous study examining patients who LWBS conducted by Mohsin (2007) had a similar success rate of reaching patients.
Some of the data collected in our study may have been biased by the parent/caretaker. In some cases, if respondents were contacted successfully, they were resentful that their child had not been seen by a physician in what they considered a timely manner, and as a result either declined to participate in the interview or responded with hostility. Others cited customer service issues. Recent publications by Wiler (2010) and Arendt (2003) have also noted similar findings. These issues may have influenced respondents in providing the interviewer with inaccurate or biased data. In addition, due to the nature of this retrospective study, participants were subject to recall bias.
The diagnostic categories of the LWBS patients covered a wide range. A large number of subjects could not remember the diagnosis that was given subsequently, therefore the chief complaints and diagnoses specifically may be broader than our data suggest.
The reliability of the final diagnoses as stated by the respondents is also somewhat unreliable since there is no corroborating data for those diagnoses from medical personnel. Studies by Mohsin (2007) and Monzon (2005), suggest that influences such as culture, environment, socioeconomic status, and true relationship of the respondent with the patient may have influenced their responses to the interviewer. The interviewers had no prior relationship with the respondent, thus, a lack of trust was sometimes noted as a barrier to transmission of information.
Lastly, we were unable to obtain physician revenue data from the hospital or the physician group based on hospital/medical group policy which does not allow this information to be released. Only billable charges and fee information were made available to the principal investigator. This limited our ability to calculate revenue loss.
Conclusions
Parents/caregivers of pediatric patients may LWBS. We have attempted to quantify the loss of billable charges from those patient visits.
Only a small portion of study patients who left without being seen had diagnostic studies (imaging, and laboratory studies) performed elsewhere. These billable charges were therefore not a significant portion of the lost charges from patients who LWBS.
Patients who LWBS ultimately result in lost billable charges. Thus, examining inefficiencies and addressing the problems associated with long waits may result in increased patient satisfaction and ultimately increased patient revenues.
References
Arendt, K. W., Sadosty, A. T., Weaver, A. L., Brent, C. R. & Boie, E. T. (2003). “The Left Without Being Seen Patients – What Would Keep Them From Leaving?” Annals of Emergency Medicine, 42 317-23.
Publisher
Bourgeois, F. T., Shannon, M. W. & Stack, A. M. (2008). “‘Left Without Being Seen’: A national profile of children who leave the emergency department before evaluation,” Annals of Emergency Medicine, 52 599-605.
Publisher
Pham, C. J., Ho G. K., Hill, P. M., McCarthy, M. L. & Pronovost, P. J. (2009). “National Study of Patient, Visit, and Hospital Characteristics Associated with Leaving an ED Without Being Seen: Predicting LWBS,” Academic Emergency Medicine, 16 949-55.
Publisher – Google Scholar
Goldman, R. D., Macpherson, A., Schuh, S., Mulligan, C. & Pirie, J. (2005). “Patients Who Leave the Pediatric Emergency Department Without Being Seen: a Case-Control Study,” Canadian Medical Association Journal, 172 39-43.
Publisher – Google Scholar
Hobbs D., Kunzman S. C., Tandberg D. & Sklar, D. (2000). “Hospital Factors Associated with Emergency Center Patients Leaving Without Being Seen,” American Journal Emergency Medicine, 18 767-72.
Publisher
Kronfol R. N., Childers K. & Caviness, A. C. (2006). “Patients who leave our emergency department without being seen: the Texas Children’s Hospital experience,” Pediatric Emergency Care, 22 550-54.
Publisher
Mohsin M., Forero R., Leraci, S., Bauman, A. E., Young, L. & Santiano, N. (2007). “A Population Follow-Up Study of Patients Who Left an Emergency Department Without Being Seen by a Medical Officer,” Emergency Medicine Journal, 24 175-9.
Publisher – Google Scholar
Monzon J., Friedman, S. M., Clarke, C. & Arenovich, T. (2005). “Patients Who Leave the Emergency Department Without Being Seen by a Physician: a Control-Matched Study,” Canadian Journal of Emergency Medicine, 7 107-13.
Polevoi S. K., Quinn, J. V. & Kramer, N. R. (2005). “Factors Associated with Patients Who Leave Without Being Seen,”Academic Emergency Medicine, 12 232-6.
Publisher – Google Scholar
Rowe, B. H., Channan, P., Bullard, M., Blitz, S., Saunders, L. D., Rosychuk, R. J., Lari, H., Craig, W. R. & Holroyd, B. R. (2006). “Characteristics of Patients who Leave Emergency Departments Without Being Seen,” Academic Emergency Medicine, 13 848-852.
Publisher – Google Scholar
Sun, B. C., Binstadt, E. S., Pelletier, A. & Camargo, C. A. (2007). “Characteristics and Temporal Trends of ‘Left Before Being Seen’ Visits in US Emergency Departments, 1995-2002,” Journal of Emergency Medicine, 32 211-5.
Publisher
Wiler, J. L., Gentle, C., Halfpenny, J. M., Heins, A., Mehrotra, A., Mikhail, M. G. & Fite, D. (2010). “Optimizing Emergency Department Front-End Operations,” Annals of Emergency Medicine, 55 142-60.
Publisher – Google Scholar