Comment:
Patients with PJS may develop testicular neoplasms in a variable percentage of cases4. These belong to stromal tumors derived from Sertoli cells5. The large-cell calcifying Sertoli cell tumor was first described by Proppe and Scully6. In most cases it appears in phenotypically normal patients as a single, firm nodule but up to one third of cases5 are associated with genetic or endocrine syndromes as Carney Syndrome or PJS. In such cases neoplasms are commonly bilateral, multifocal, smaller and they appear earlier5,7, as in our patient. The testicular lesion specifically associated with PJS is called Intratubular large cell hyalinizing Sertoli Cell (LCHSC) neoplasia7 and is similar to the sex cord tumor with annular tubules of the ovary that appears in women with PJS8.
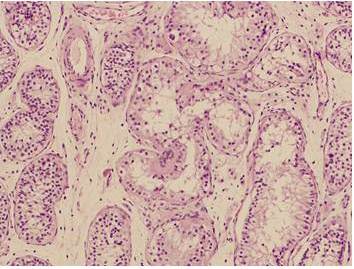
Histologically, the lesion shows a patchy distribution of enlarged tubules, which exceed several times the diameter of unaffected tubules. Sertoli tumor cells are large with vacuolated and eosinophilic cytoplasm. Tubules can be replaced by basement membrane deposits, giving a hyalinized appearance7. Another feature is the presence of calcifications, not always present in cases of PJS7,9, but seen in our patient. In some cases Intratubular Sertoli Cell Proliferations (ISCPs) have been described. They emerge from seminiferous tubules and gradually replace the cell population. There is controversy about whether ISCPs are non-neoplasic proliferative lesions with malignant potential or represent an intraepithelial stage of tumor development. Although in some patients ISCPs are the only pathological finding, they may appear nearby to large-cell calcifying Sertoli cell tumor10. Some authors argue that they are the testicular neoplasm specifically associated to PJS7,11.
Extratubular growth implies potentially malignant nature irrespective of local characteristics4. Malignancy is found in approximately 17% of patients with large-cell calcifying Sertoli cell tumor9, ussually in older patients with unilateral and unifocal mass8,9. In patients with PJS reviewing of published cases finds that local infiltration is very uncommon, so the process often remains confined to the tubules for long periods of time2. Anyway, it should be note that the follow-up period of these patients is limited since first cases date from the 80´s and progression to invasive tumor cannot be rule out12. Venara et al10 described a patient with a follow up of more than 30 years with no evidence of progression. Although histological malignancy index have been described (high mitotic rate, nuclear atypia, necrosis and vascular or lymphatic invasion)8,9, the question of which damage may progress is still unknown7.
Tumor cells have increase activity of aromatase enzyme10, which normally is produced by Leydig cells9. This determine a higher conversion of testosterone to estradiol. As a result, patients with LCHSC typically have clinical signs of estrogenic activity that lead to the suspicion of the tumor, such as acceleration of growth with avanced bone age9 and gynecomastia10. However, cases of incomplete penetrance have been already described 15 and peripubertal gynecomastia not necessarily related to the tumor was appreciated in our patient.
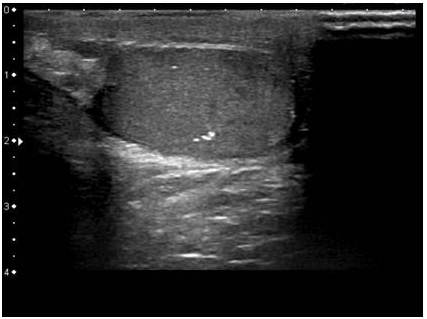
The course of evolution of this condition justifies its conservative management monitoring by ultrasounds. Surgery could be indicated in selected cases of unusual invasive tumors, pain or mass effect. Hormonal manifestations could be treated with aromatasa inhibitors13, like testolactone and anastrozol. These drugs can be effective in controlling the clinical features of the disease, like breast development, growth velocity and bone maduration16 but evidence is limited and further studies are required9. In our patient no hormonal abnormalities were found and bone age and growth was normal so it was decided to keep monitoring. Later ultrasound controls show no change compared to previous.
The case reported here represents an unusual presentation because it appears in an asymptomatic boy with almost no estrogenic manifestations unless mild gynecomastia. The lesion was diagnosed during a routine check, which should make us question the kind of monitoring strategies in these patients with increased risk of cancer. In case of testicular neoplasms surveillance strategies are based on expert opinion only. It is recommended to perform annual physical examination and ultrasound in case of detection abnormalities or signs of precocious puberty1. Anyway, it should be noted that average age of presentation of these tumors is earlier than in others cancers associated to PJS1,4,8. As in our case, diffuse and bilateral testicular involvement can overlook the presence of changes on physical examination13 and the development of secondary hormonal disturbances may not be present at an early stage. Hyperestrogenism cannot be detected in laboratory tests because the hormone excess is limited to testicular aromatase14, which may explain the findings in our patient.
Conclusions
Our case highlights the need to establish a high index of suspicion of testicular tumors in patients with PJS. Although LCHSC usually remains confined locally, can lead to endocrine disorders with impact on growth and pubertal development in children. It is necessary to establish preventive diagnostic strategies from an early age in these patients.
Acknowledgments
The authors thank Dr. M. Nistal, Department of Pathology, La Paz University Hospital, for providing histopathological assistance.
References
1. Beggs, A. D., Latchford, A. R., Vasen, H. F. et al. (2010). “Peutz Jeghers Syndrome: A Systematic Review and Recommendations for Management,” Gut. 59(7):975-86.
Publisher – Google Scholar
2. Dreyer, L., Jacyk, W. K. & du Plessis, D. J. (1994). “Bilateral Large-Cell Calcifying Sertoli Cell Tumor of the Testes with Peutz Jeghers Syndrome: A Case Report,” Pediatric Dermatology. 11(4):335-7.
Publisher – Google Scholar
3. van Lier, M. G., Wagner, A., Mathus-Vliegen, E. M. et al. (2010). “High Cancer Risk in Peutz—Jeghers Syndrome:”¨ A Systematic Review and Surveillance Recommendations,” American Journal of Gastroenterology. 105(6):1258-64.
Publisher – Google Scholar
4. Ulbright, T. M., Amin, M. B. & Young, R. H. (2007). “Intratubular Large Cell Hyalinizing Sertoli Cell Neoplasia of the Testis: A Report of 8 Cases of a Distinctive Lesion of the Peutz-Jeghers Syndrome,” American Journal of Surgical Pathology. 31(6):827-35.
Publisher – Google Scholar
5. Ahmed, H. U., Arya, M., Muneer, A., Mushtaq, I. & Sebire, N. J. (2010). “Testicular and Paratesticular Tumours in the Prepubertal Population,” The Lancet Oncology. 11(5):476-83.
Publisher – Google Scholar
6. Proppe, K. H. & Scully, R. E. (1980). “Large-Cell Calcifying Sertoli Cell Tumor of the Testis,” American Journal of Clinical Pathology. 74(5):607-19.
Publisher – Google Scholar
7. Young, R. H. (2008). “Testicular Tumors – Some New and a Few Perennial Problems,” Archives of Pathology & Laboratory Medicine. 132(4):548-64.
Publisher – Google Scholar
8. Kratzer, S. S., Ulbright, T. M., Talerman, A. et al. (1997). “Large Cell Calcifying Sertoli Cell Tumor of the Testis: Contrasting Features of Six Malignant and Six Benign Tumors and a Review of the Literature,” American Journal of Surgical Pathology. 21(11):1271-80.
Publisher – Google Scholar
9. Gourgari, E., Saloustros, E. & Stratakis, C. A. (2012). “Large-Cell Calcifying Sertoli Cell Tumors of the Testes in Pediatrics,” Current Opinion in Pediatrics. 24(4):518-22.
Publisher – Google Scholar
10. Venara, M., Rey, R., Bergadá, I. et al. (2001) “Sertoli Cell Proliferations of the Infantile Testis: An Intratubular form of Sertoli Cell Tumor?,” American Journal of Surgical Pathology. 25(10):1237-44.
Publisher – Google Scholar
11. Amin, M. B., Young, R. H. & Scully, R. E. (2001). ‘Large Cell Hyalinizing Sertoli Cell Tumor of the Testis: A Distinctive Estrogenic Tumor of Boys with Peutz—Jeghers Syndrome (PJS). A Report of Six Cases,’ Modern Pathology. 14:100.
Google Scholar
12. Young, R. H. (2005). “Sex Cord-Stromal Tumors of the Ovary and Testis: Their Similarities and Differences with Consideration of Selected Problems,” Modern Pathology. 18 Suppl 2; S81-98.
Publisher – Google Scholar
13. Kara, C., Kutlu, A. O., Tosun, M. S. et al. (2005). “Sertoli Cell Tumor Causing Prepubertal Gynecomastia in a Boy with Peutz-Jeghers Syndrome: The Outcome of 1-Year Treatment with the Aromatase Inhibitor Testolactone,” Hormone Research in Paediatrics. 63(5):252-6.
Publisher – Google Scholar
14. Young, S., Gooneratne, S., Straus, F. H. 2nd. et al. (1995). “Feminizing Sertoli Cell Tumors in Boys with Peutz-Jeghers Syndrome,” American Journal of Surgical Pathology. 19(1): 50-8.
Publisher – Google Scholar
15. Lefevre, H., Bouvattier, C., Lahlou, N. et al. (2006). “Prepubertal Gynecomastia in Peutz-Jeghers Syndrome: Incomplete Penetrance in a Familial Case and Management with an Aromatase Inhibitor,” European Journal of Endocrinology. 154(2):221-7.
Publisher – Google Scholar
16. Grandone, A., del Giudice, E. M., Cirillo, G., Santarpia, M., Coppola, F. & Perrone, L. (2011). “Prepubertal Gynecomastia in Two Monozygotic Twins with Peutz-Jeghers Syndrome: Two Years’ Treatment with Anastrozole and Genetic Study,” Hormone Research in Paediatrics. 75(5):374-9.
Publisher – Google Scholar