Daniel B Markeson, Olivier A Branford and Isam Al-Basri
Department of Plastic Surgery, Wexham Park Hospital, Slough, United Kingdom
Volume 2013 (2013),
Article ID 603862,
Plastic Surgery: An International Journal,
6 pages,
DOI: 10.5171/2013.603862
Received date: 28 November 2012; Accepted date: 10 February 2012; Published date: 27 February 2013
Academic Editor: UmarDaraz Khan
Cite this Article as:
Daniel B Markeson, Olivier A Branford and Isam Al-Basri, “The ‘Cleavage Imprinting’ Technique for Ensuring Mirror Image Medial Scar Symmetry in Reduction Mammoplasty,” Plastic Surgery: An International Journal, vol. 2013, Article ID 603862, 6 pages
DOI: 10.5171/2013.603862
A key step in the inverted T-scar pattern breast reduction technique is the preoperative marking of the medial skin incision which will ultimately become the medial aspect of the horizontal scar in the new inframammary fold. We describe the ‘cleavage imprinting’ technique that allows the surgeon to generate mirror-image medial imprint marks on the contralateral breast during preoperative marking. Using photographs from two clinical cases we demonstrate that this simple, inexpensive, easily learnt and reproducible method is a handy way of improving the symmetry of the medial incision borders in mammaplasty. Although it is not a novel technique, its widespread employment being a testament to its usefulness, to our knowledge it has not previously been described in the literature.
Keywords: Breast reduction, mastopexy, aesthetic breast surgery
Introduction
Reduction mammaplasty is one of the top five most commonly performed cosmetic surgical procedures for women and together with mastopexy accounts for 240000 cases per year (ASAPS, 2011). Although a number of skin excision patterns now exist, many plastic surgeons still use the classic inverted T-scar pattern (Wise, 1956). A key step in this technique is the preoperative marking of the medial skin incisions, which will ultimately become the medial aspect of the horizontal scar in the new inframammary fold. We describe a simple technique that allows the surgeon to generate mirror-image medial imprint marks on the contralateral breast. This maximises the likelihood of postoperative scar symmetry.
The Main Body of the Paper
Materials
A ruler or measuring tape; an indelible marker pen.
Technique
For the purposes of this report, preoperative photographs of a reduction mammaplasty are shown (Figures 1 to 4). It is worth noting that this patient had an earlier partial right mastectomy highlighting that this technique is applicable to create symmetry in preoperatively symmetrical and near symmetrical breasts. Preoperative skin markings were carried out by the senior author using his ‘cleavage imprinting’ technique as follows.
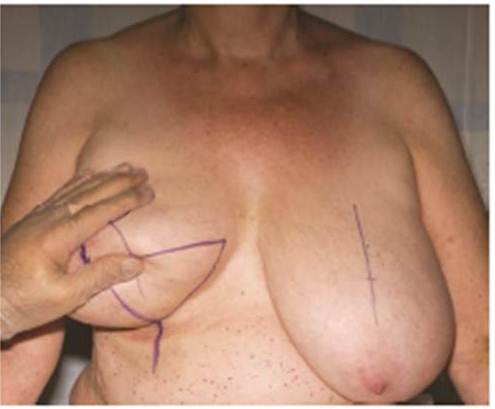
The patient was marked standing with an indelible marker pen. The breast meridians, the inframammary folds (in their central portion only), and the new nipple positions were marked bilaterally. Then the remaining skin markings for the inverted T-scar pattern were drawn onto one breast only, the right breast in the case shown (Figure 1).
Figure 1: Photograph of Preoperative Breast Reduction Markings with the Right Side Marked Medially
Once carefully drawn onto one breast, the marker pen was used to go over the medial skin markings once again (Figure 1). Then, with the ink still fresh, the breasts were pushed gently together (Figure 2).
Figure 2: Photograph of Both Breasts Pressed Gently Together by The Surgeon in the ‘Cleavage Imprinting’ Technique to Create a Mirror-Image Marking on the Contralateral Breast
After releasing the breasts a fainter mirror image imprint was produced on the contralateral breast (Figure 3).
Figure 3: Photograph of the Medial Markings of Both Breasts Showing a Faint Line on the Second (Left) Breast
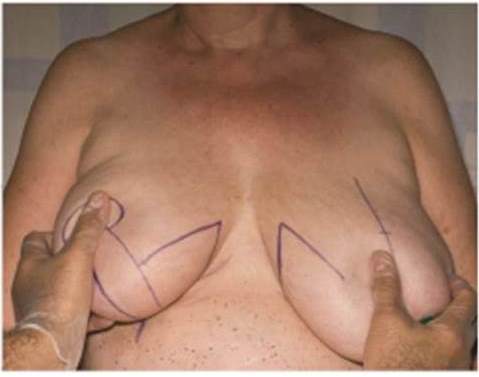
The marking pen was then used to trace over and emphasise the new and symmetrical marking (Figure 4).
Figure 4: Photograph with the Medial Markings on the Second (Left) Breast Having Been Emphasised, Demonstrating the Symmetry Created by the ‘Cleavage Imprinting’ Technique
With this medial marking now symmetrical on the left breast the remaining markings were then carried out to complete the preoperative skin markings.
Results
The postoperative result of the patient shown in Figures 1 to 4 is demonstrated in Figure 5.
These clinical photographs demonstrate the postoperative symmetry that can be achieved in the medial breast scars. The technique also works well for patients with very large breasts with minor asymmetry as demonstrated in Figure 6. It is worth noting that this technique may be usefully applied with very good results in both mastopexy and in therapeutic mammoplasty for larger breasts. The practicability of the technique does not only depend on volume, but rather the vertical length of the breast (suprasternal notch to nipple distance).
Figure 6: (A) Preoperative Photograph for Another Patient Undergoing a Bilateral Breast Reduction Using the ‘Cleavage Imprinting’ Technique. (B) Postoperative
Result
One limitation of the technique is that the surgeon needs to be consistent in their technique for pushing the breasts together as this may influence the medial marks on the other breast during preoperative marking. Further, as a precaution, the technique should not be used in cases where there is obvious preoperative asymmetry in breast shape, size or in the inframammary fold.
Discussion
Scarring is the most frequent cause of dissatisfaction for patients following reduction mammaplasty (Godwin, 1998; Migzala, 2000; Brown, 2000). The inverted T-scar technique has three component scars: periareolar, vertical and inframammary. A recent study which compared patient satisfaction regarding these three scar components after inferior pedicle breast reduction found that the inframammary scars were the least pleasing from a patients’ perspective (Çelebiler 2005). The surgeons’ evaluation of the three scars in the same study showed that there was no objective difference in the degree of hypertrophy and that the inframammary scars were less wide than both the periareolar and vertical scars. The authors found that the colour match in the inframammary scars was the poorest. This suggests that visibility and symmetry of the inframammary scar are the most important features in post reduction mammaplasty scarring that determine patient dissatisfaction. The most common postoperative complaint in another study on reduction mammaplasty was also related to the scar with approximately half of patients not being happy with the result (Fereirra, 2000). Other studies have also confirmed the fact that the horizontal scar from reduction mammaplasty is the component that most bothers patients and leads to greatest dissatisfaction (Sprole, 2007; Cruz-Korchin, 2003).
Various methods have been used in an attempt to ensure symmetry in breast surgery, ranging from tape measures (Spear, 2007), callipers (McKissock, 1991) or a goniometer (Lazarus, 1998) to a skin marker pen attached to a pendulum made from a silk suture in a midline structure (Raveendran, 2008). A study of 100 patients undergoing breast augmentation showed 88 percent of the women had some degree of asymmetry, with 65 percent having more than one parameter involved (e.g. inframammary fold and nipple-areola complex), emphasising the difficulties facing Plastic surgeons as they attempt to create symmetrical breasts in mammaplasty (Rohrich, 2006).
We have demonstrated a simple, inexpensive, easily learnt and reproducible handy method to obtain symmetry with the medial skin incisions and therefore the medial aspect of the postoperative inframammary fold scar. The senior author has used this technique routinely in hundreds of reduction mammaplasty cases and found that it provides good patient satisfaction. The technique has the advantage that the patient is aware of the mirror image imprint, as this is highlighted to the patient during marking, prior to undergoing surgery, emphasizing the surgeon’s attempts to achieve symmetry. Although it is not a novel technique, its widespread employment being a testament to its usefulness, to our knowledge it has not been previously described in the literature.
Spear, S. L. (2007). ‘Breast Reduction: Inverted T-Technique,’ In: Thorne TH. Grabb and Smith’s Plastic Surgery. 6th ed. Philadelphia: Wolters Kluwer Lippincott Williams and Wilkins, Philadelphia, PA, USA. 593-603. Google Scholar