Introduction
It is widely known that information technologies will revolutionize patient care, medical research, medical education and the administration of health services. Information technology is increasingly recognized as important in clinical practice, but much remains to be done to implement its use. The term telemedicine encompasses a wide range of telecommunications and information technologies. The first telemedicine programs were established almost 40 years ago, but the technology has grown considerably in the past decade (Hu et al., 2000).
Telemedicine encompasses all medical activities: diagnosis, treatment, prevention, education, and research (Craig and Patterson, 2005). Telemedicine refers to the use of information and telecommunication technologies to develop information and/or expertise necessary for healthcare services provision, collaboration and/ or develop geographically separated participants, including physicians and patients (Bashshur, 2002).
Telemedicine has been recognized as a tool for exchange ideas and sharing knowledge among health professionals. Stanberry (2006) defined telemedicine using of telecommunications technology to provide clinical information and services.
Despite the fact that collaborative technologies used in telemedicine such as videoconference and internet is becoming very cheap, still the investment in these technologies by health organizations in Jordan is very little.
Many studies conclude that telemedicine has the requisite technology, but face uncertainties such as: lack of long-term sustainability plans; lack of nature programs that can be the basis of definitive cost-benefit analysis; and limited acceptance of telemedicine by health providers (Bashshur, 2002). It was also concluded that telemedicine has been slower to implement than originally envisioned or expected.
It has been difficult to move beyond single transmissions and limited projects into routine use. Generally speaking, it seems that the real telemedicine challenges are not of a technical nature, but relate to non technical factors such as individual or organizational considerations (Stanberry, 2006).
In general, telemedicine technology includes both store-and-forward-asynchronous, as well as live videoconferences-synchronous (Wootton, 2001). Several studies discussed the potential benefits of telemedicine for patients and healthcare providers hence, the results demonstrated the socio-economic impacts of telemedicine improving efficiency and quality care services (Craig and Patterson, 2005; Kifle et al., 2006). In this study, the researcher focused on the role of collaborative platform, governments, and organization to support health care services. The challenge is how can health care institutions can better communicate and collaborate within their employees, patients and stakeholders.
Creating knowledge suggests the need for improved knowledge flow internally within the organization and externally to the patient and stakeholders. Leveraging knowledge through the connection and collaboration of others may lead to critical success factor in whether a learning organization is successful (Chou and Brauer, 2005).
Collaborative learning refers to groups of professionals and practitioners, often from the same or related background, are coming together to share ideas and experience and to tackle common problems and issues. Further, the role of government and technology platform in facilitating communication and collaboration at health care institutions in Jordan are critical.
This study can help in building a community of health professionals and policy makers who collaborate in telemedicine development. In addition, this study will address the key factors that challenge the initiate telemedicine in health care services at Jordan.
Research Objectives
This study attempts to provide some viewpoints, and empirical results to understand the relevance requirements and constraints influence on telemedicine services in Jordan. Following are the main objectives of this study:
- To address the key factors that challenge telemedicine technology initiation in health care institutions.
- To identify the critical success factors of telemedicine transfer and performance in healthcare institutions.
- To develop a telemedicine framework model that can be used as a strategic adoption tool to support collaboration and knowledge sharing in healthcare institutions.
Theoretical Background
Telemedicine is one of the first innovative information systems to be integrated into healthcare services in the last fifty years (Wootton 2003; Stanberry, 2006; Struber, 2004). Telemedicine has witnessed rapid development in the last fifteen years; in recent years a number of studies have addressed the feasibility of clinical telemedicine applications (Kuntalp and Akar, 2004).
However, few studies discussed the social value of telemedicine applications in developing countries. According to Tan et al. (2005) telemedicine evolution can be analyzed through three historical periods, the first period focused on the improvement of clinical care in specialty areas including teleradiology, telecardiology, teledermatology, and telepsychiatry, the majority of studies in this stage were focused on proof-of-concept research in the form of technological feasibility studies.
The second historical period was characterized by the development of digital technology, in this stage computers became commonplace and digital communication methods merged quickly, They also founded that interactive video could be used over wide area surface networks at a much lower cost than the along television system of the first stage, studies in this stage started during of computer-based digital teleconferencing systems.
The third historical period focused on improving standards, use of wireless technologies, security, confidentiality and privacy issues, legal questions on jurisdiction and reimbursement for telemedicine services.
Many healthcares institutional adopt telemedicine technology for healthcare services improvement; enhance effectiveness & efficiency, and competitiveness enhancement as well. The readiness of healthcare institutions and the availability of the appropriate conditions are a motivation for the adoption of telemedicine (Hu et al., 2000).
Previous studies illustrated that a telemedicine initiative can be challenged by institutional culture and work processes (Robinson et al., 2003). When referring to collaboration, about what is one actually speaking? To put it simply, the term collaboration appears to refer to any activities that a pair of individuals or a group of people performs together.
Within learning sciences, common to the different definitions of collaboration is that they stress the idea of co construction of knowledge and mutual engagement of participants. In this sense, collaboration can be considered as a special form of interaction.
Rochelle and Pea (1999) for instance, stressed the role of shared understanding, and pointed that collaboration is a coordinated, synchronous activity that is the result of a continued attempt to construct and maintain a shared conception of a problem. Cooperation is working together to accomplish shared goalsw; within cooperative activities individuals seek outcomes that are beneficial to themselves and beneficial to all other group members.
Systematically structuring those basic elements into group learning situations helps ensure cooperative efforts and enables the disciplined implementation of cooperative learning for long-term success (Kaplan, 2000).
The benefits of collaborative learning are that people bring divergent ideas in a collaborative environment and work towards the development of a shared understanding and building common knowledge (Tan at al., 2005).
At present, the current understanding appears to be that collaboration is a synonym for good learning and good educational technology; almost any web-based application is labeled as collaboration (Heinzelmann et al., 2003).
Increasing costs of health care and rapid knowledge growth have led to collaborate among health care professionals to share knowledge and skills. It is generally assumed that health care teams function in a collaborative manner can deliver health care efficiently & effectively. Collaborative learning process can exchange of ideas within small groups not only increases interest among the participants but also promotes critical thinking.
Collaboration in health care requires creating a platform, and governmental role to support sharing knowledge and experiences among employees. Sherry L. et al., (2004) argued that collaboration and health care teams are common in hospitals and long-term care facilities, but teams are often not available to providers in the community where most practitioners work independently.
A team environment could provide support for these community-based health care providers as well as allow for more efficient sharing of information. Collaboration makes group members more flexible and eventually replaceable as the group as a learning community shares knowledge and experiences (Struber, 2004).
Collaborative learning in health care services need to create the environment that support and encourage sharing knowledge such as: government policy, IT infrastructure, top management support, and business process management to provide employee the viability of discussion and reflection (Scott et al., 2005).
Form a pedagogical perspective; educators have long considered discussion as one of the most powerful techniques to promote learning. Wessner, M. et al, (2002) stated that collaborative learning has a great potential in facilitating active, constructive, and experiential learning. In a collaborative learning environment learners collaborate to perform educational tasks, activities, projects and other activities(W essner et al.,2002).
Effective communication is the central to functioning complex healthcare environments, providing optimal patient care requires the coordination of many different teams and services within the health system. Effective communication within and/or between teams is essential for achieving this coordination (Scott et al., 2005), effective communication can be characterized by being clear, complete, accurate, timely and requiring verification from the parties involved.
Verifying what has been communicated is important to the process, that is, the parties involved in the communication act need to ensure that the meaning of the sent message is understood and mutually agreed upon. Healthcare domain is a multidisciplinary setting where professionals from several disciplines, work together to provide care service to patients (Huston and Huston, 2000).
Previous studies(Wessner,2002;Craig and Patterson,2005) pay attention that cooperation in healthcare is important for two reasons, first: the division of skills within healthcare has become more pronounced as patient care has become more complex with the introduction of new technology, for example today nurses carry out actions that used to doctors responsibility and some tasks previously carried out by fully qualified nurses have been taken over by auxiliary nurses or administrative staff, e.g. washing and dressing of patients, feeding patients, serving meals, requesting medical notes from patients general practitioners (GPs) or hospitals etc.
The second reason is patient care is no longer solely medical care but involves input from healthcare professionals coming from several disciplines. The areas of healthcare that sees the greatest changes towards truly shared patient care are the ones where professionals from different disciplines have a large impact on the shared task of improving a patient’s state of health, for example cancer care is a highly cooperative area, where different needs of cancer patient can only be met by efficient cooperation of professionals from several disciplines (Rotvold, 2003).
The telemedicine performance dimensions deal with issue of uneven geographical distribution of healthcare resources and healthcare facilities (Han, 2005). The level of healthcare facilities and specialists skills are not the same in the develop countries.
Lack of accessibility o healthcare and rising health costs as a consequence of the high level of disease burden still consider an issue in the developing countries. Therefore, telemedicine considered as one of the methods to improve health status and reduce costs .More, potential of telemedicine systems can be expected to improve access to healthcare, and the efficiency with which it is delivered (Moore, 2002).
Even if the benefits of telemedicine are substantial, the practice of telemedicine is still not considered as part of healthcare practice in most of the hospitals in developing countries in general and Jordan in particular. International telemedicine link for medical education has been established between Jordan and the USA.
The king Husain medical centre and the Amman surgical hospital are linked to the Mayo Clinic. Interactive medical education programs are broadcast from the mayo clinic and received at the king Hussein medical centre auditorium. Moreover, heartbeat Jordan, a private company, and the ministry of health established a cardiac telemonitoring service within the country.
However, it is hoped that telemedicine can address four major concerns of researchers and practitioners: First, healthcare access is made possible for remote (isolated), confined patients, and improved by lowering geographical barriers hence totally affected on organization learning positively. Second, human resource development is promoted, and recruitment and retention of physicians in rural areas is encouraged also hence totally affected on organization learning positively.
Third, in terms of the issue of quality of care, telemedicine will provide clinicians’ better, timely information about the patient hence totally affected on the patient satisfaction positively.
Therefore, through the internet, the healthcare staff will receive information that may be vital to patient care. Also, telemedicine will reduce misdiagnoses of patients, and increase the local physicians’ professional experience. Fourth, from the economic perspective, telemedicine adoption may enhance efficiency&effectiveness (Struber, 2004).
Conceptual Model and Hypotheses Development
The literature review of telemedicine transfer and performance indicated that non-technical issues should be addressed. Thus, the theoretical model for this study is based on strategic level model. Figure 1 illustrated three independent variables that directly affect the telemedicine transfer.
On the organizational level we have organizational support; organizational motivation; and organizational change, on the governmental level we have ICT infrastructure; ICT polices; security; and legal standards, on the collaboration level we have intranet; and wireless devices. Also Figure 1 illustrated three dependent variables related to telemedicine performance these variables are; effectiveness&efficiency, organizational learning, and patient satisfaction.
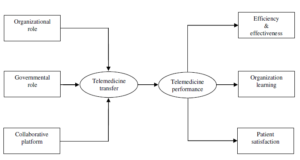
Fig1. The research model
Researcher hypothesize two sets of hypotheses will be tested in order to answer the research questions. The first set of hypotheses consider the effects of telemedicine transfer, while the second set hypotheses consider the effects of telemedicine transfer on the telemedicine performance and outcomes “efficiency&effectiveness, organizational learning, and patient satisfaction”. In general, proposed model attempts to answer two research questions:
1. What is the main factors influence on transferring of telemedicine in Jordan?
2. What aspects of telemedicine transferring influence on the telemedicine performance and the outcomes in Jordan?
In order to answer these two research questions with the background of a proper theoretical framework and to explain which factors are especially strongly related to telemedicine outcomes in Jordan. The framework of telemedicine developed based on various literature reviews on telemedicine with focusing on cost reduction, time saving, patient satisfaction, and organizational learning. The major hypotheses of this study are:
H1: Organizational role is positively associated with telemedicine transfer.
H2: Governmental role is positively associated with telemedicine transfer.
H3: Collaborative platform is positively associated with telemedicine transfer.
H4: Telemedicine performance is positively associated with efficiency&effectiveness.
H5: Telemedicine performance is positively associated with organizational learning.
H6: Telemedicine performance is positively associated with patient satisfaction.
H7: Telemedicine transfer is positively associated with telemedicine performance.
Methodology
Research methodology depicts the activities, tools, and methods that will be performed in order to achieve the intended objectives, accurate data collection, and apposite analysis. Alkhaldi (2007) has distinguished between the two terms that some researchers use interchangeably: ‘research design “methodology”‘ and ‘research technique “methods”‘.
The term research design or methodology refers to the overall strategy of the research. Thus, the research design should advise us on how the sample will be drawn, what groups andor subgroups it must include, what contrast should be made, what variables we need to consider and measure and how these measures are linked to external events.
The research design is concerned with making our problems accessible by directing our research in a way that generates precise answers to precise questions. Alkhaldi (2007) cited from Creswell (1994) two approaches that the research methodology can be derived from, these two approaches can be classified into two main categories: a positivistic and a phenomenological approach. These two categories are sometimes described by different terms.
The positivistic approach can sometimes be labeled as traditional, quantitative, or empiricist whilst, the phenomenological approach can be labeled as post-positivistic, subjective, or qualitative.
Alkhaldi (2007) summarized that the terms that are associated with each approach are not necessarily interchangeable and, in many cases, have emerged as a corollary of the author wanting to bestow a different approach. The positivistic approach seeks causes of social phenomena or objective knowledge (facts) that can be gained from experience or observation, while paying little attention to the subjective state of individuals, thus, employing a logical reasoning to attain objectivity when investigating a phenomenon and explaining causality.
The positivistic approach is largely based on quantitative data. Explaining causality requires the establishment of relationships between variables and linking them to a certain theory.
The benefits of positivistic approach are cost effective and speed in data collection, the ease of analysis, apposite for testing hypotheses and determining relations between variables and establishing the reliability and generalizability of data. Therefore, the researcher adopts positivistic approach to achieve the intended objectives.
To test the proposed model and the associated hypotheses and to evaluate the telemedicine outcomes, a questionnaire designed to cover all variables in the proposed models that influence on the transferring and performance of telemedicine.
A pilot test will be done to assess the reliability and construct validity of the instruments, people who’s participated in the pilot test excluded from the subsequent formal survey. Questionnaires were sent out to the senior administrator and to the medical director of each organization.
A self-administrated questionnaire survey was used, thus before distribute questionnaires, each organization’s management will be informed of researcher intent by means of an introductory letter that briefly states the study’s purpose and its significance.
Four hospitals was chosen purposively that cover all health care sectors in Jordan which are; King Hussein Cancer Center (Private Sector); King Hussein Medical City (Royal Medical Services); King Abdullah University Hospital (University); Prince Hamza Hospital (Ministry of Health).
Out of a total 240 responses to survey, 87.5% was retained (210 responses) and used in the study, the remainders 12.5% of the responses (30 responses) were dropped because of too many missing data points.
Data Analysis and Results
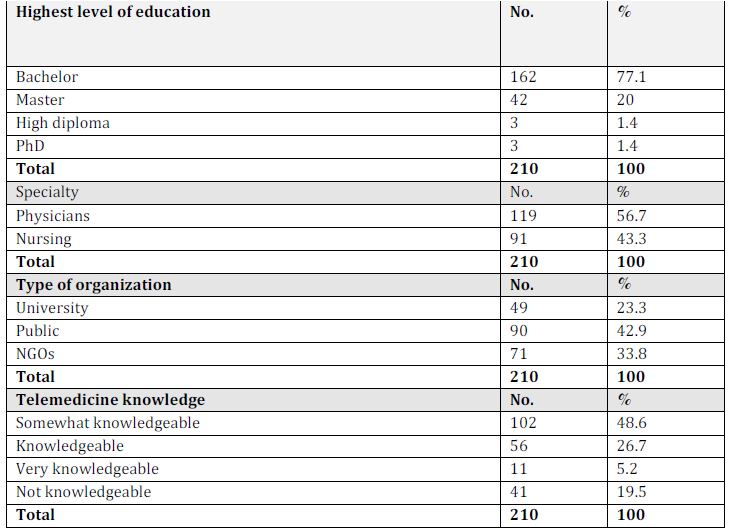
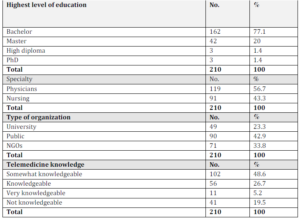
Demographic results
The backgrounds of respondents were studied in terms of the job title and educational background. Table 1 categorized demographic questions. Most of the respondents were employed at government hospitals. Most responses were physicians from persons between the ages of 35 and 45; most participants also have a Bachelor degree and they are to some extent knowledgeable about telemedicine.
Confirmatory Factor Analysis
Factor analysis is a method used to examine a number of measured variables; the main applications of a factor analysis technique are data reduction or structure detection (Maccallum et al., 1996). In general, both exploratory (EFA) and confirmatory factor analysis (CFA) are performed by examining the pattern of correlations between the observed measures.
EFA represents a procedure for the discovery of structure, while at the other extreme, CFA is a technique for testing hypothesized structure formed a prior basis in practice the EFA and CFA procedures tend to converge and represent differences in degree in this sense (Maccallum et al., 1996).
EFA is used to determine the number of common factors influencing a set of measures, and the strength of the relationships between each factor and each observed measure (Hair et al., 1998). CFA is used to determine the ability of a predefined factor model to fit an observed set of data. CFA ensures that, in a factor analysis of all the items in the instrument, each item is loaded on the construct to which it is theoretically assigned.
Hair et al., (1998) suggested that EFA analysis is most appropriate in the initial stages of model development, whereas CFA provides a more powerful tool in the second stage of research, when a model has been established. Confirmatory factor analysis was carried out to assess the measurement.
Factor analysis can be used for defining indicators of constructs, defining dimensions underlying existing measurement instruments, determining what items or scales should be included on and excluded from a measure.
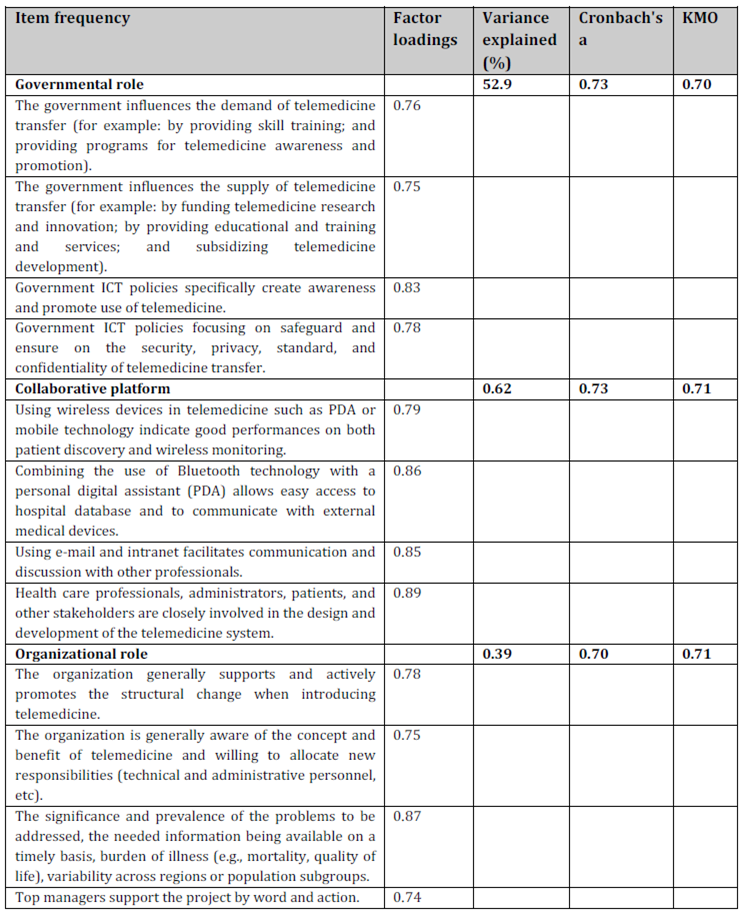
Factor analysis was conducted to analyze the scale items of the ten research constructs, and to check the construct validity of the measurement scale. To assess the suitability of data analysis, Bartlett’s Test of Sphericity suggests that the intercorrelation matrix contains sufficient common variance to make factor analysis worthwhile, Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy were used (Hair et al.,1998).
The KMO measure provides a means to assess the extent to which the indicators of a construct belong together (the homogeneity of variables). Maccallum et al. (1996) recommended accepting values greater than 0.5 as acceptable (values below this should lead to either collect more data or rethink which variables to include). Furthermore, values between 0.5 and 0.7 are mediocre, values between 0.7 and 0.8 are good, values between 0.8 and 0.9 are greater and values above 0.9 are superb factors with Eigenvalues greater than one were retained in the factor loading (Hair et al.,1998).
The principal components extraction in the unrotated factor solution with Eigenvalues over one, and Varimax as the rotation method, which is a matrix of factor loading for each variable onto each factor were utilized to identify the underlying subfactors of the critical factors for telemedicine transfer and telemedicine outcomes.
Factor loading below 0.5, which is the cut-off limit for loading items, should be considered low and any low items should be eliminated from the analysis for the underlying factors that explain joint variation in the items measured. Factor analysis for each constructs of research model is presented as below.
Table 2: Results of factor analysis (independent variables)

Table 3: Results of factor analysis (dependent variables)

Statistic cronbachs alpha is important reliability measure of a psychometric instrument, cronbachs alpha generally increase when the correlations between the items increase (Maccallum et al., 1996), for this reason the coefficient is also called the internal consistency.
Reliability is the internal consistency of a scale, which assesses the degree to which items are homogeneous (Maccallum et al., 1996). Generally, reliability is concerned with the interrelationship among items in the scale for all who answer the item. Some professionals, as a rule of thumb, require a reliability of 0.70 or higher before they will use an instrument (Maccallum et al., 1996). Obviously, this rule should be applied with caution when alpha has been computed from items that systematically violate it assumptions.
Further, the appropriate degree of reliability depends upon the use of the instrument. Cronbach’s alpha was analyzed using SPSS version 17. As summarized in Table 2 and 3, all of the values were above acceptable range 0.70.
LISREL (Joreskog and Sorbom, 1989) and EQS (Bentler, 1989) are the two most popular SEM software packages used by researchers. Although the parameter estimates, standard errors and tests are essentially identical for both packages, EQS uses simpler terminology and notation(Brown, 1986). The goodness of fit test is carried out using Chi-squared goodness of fit test and other tests which are available in EQS.
The parameter estimates are derived using maximum likelihood estimation(MLE) or generalized least squares(GL) estimation methods. This study used EQS, and generalized least squares(GL) estimation method to test the conceptual model.
With an adequate measurement model and an acceptable level of significant. Using EQS V6.1 it is possible to specify, test, and modify the hypothesized measurement model. As a starting point, successive modifications were made to some of the scales until the parameters and the fit indices reached values within the recommended limits.
only three parameter was altered for each iteration to avoid over modifying the model. Hoyle (1995) draw attention that model-data fit evaluated based on multiple fit indexes.
The overall model fit indexes include goodness of fit index (GFI), and root mean square error of approximation (RMSEA). GFI indicates the relative amount of variance and covariance jointly explained by the model. Hoyle(1995) interpreted these index scores GFI in the range of .80-.89 as representing reasonable fit; scores of .90 or higher are considered as evidence of good fit.
The RMSEA takes into account the error of approximation and is expressed per degree of freedom, thus making the index sensitive to the number of estimated parameters in the model; values less than 0.05 indicate good fit. Values as high as 0.08 represent reasonable errors of approximation in the population, values ranging from 0.08 to 0.10 indicate mediocre fit, and those greater than 0.10 indicate poor fit.
The comparative fit index (CFI) is equal to the discrepancy function adjusted for sample size. CFI ranges from 0 to 1 with a larger value indicating better model fit. Acceptable model fit is indicated by a CFI value of 0.90 or greater (Hoyle, 1995).
But its indictor to model fit when value was reduced from 55.3 to 26.1. GFI is 0.95, AGFI is 0.92, CFI is .98, FIT is .97, IFI is .98 that’s mean all of index above to acceptable value 9.0 and RMSEA is .03 below to acceptable value0.05.
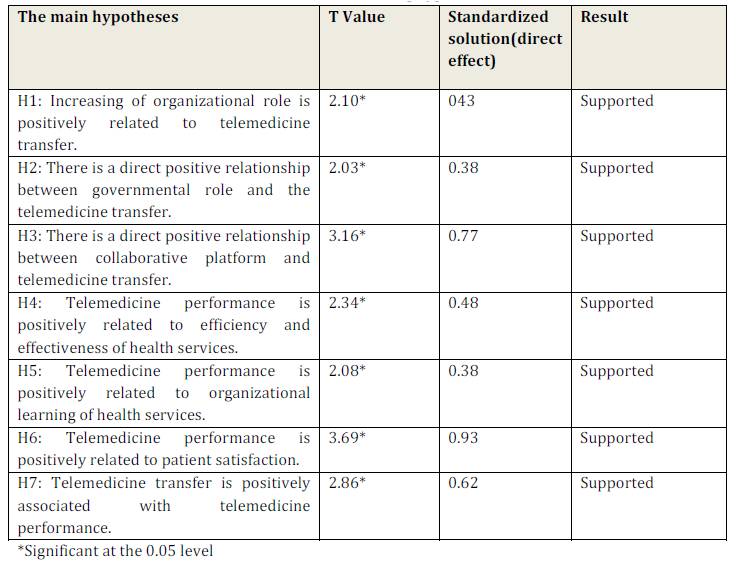
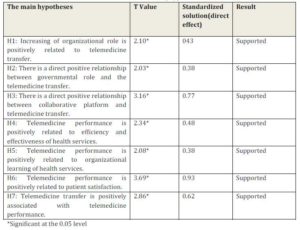
Thus, overall the data indicate a favorable fit for our conceptual model. Hypotheses test using a T value-squared- standardized solution, the result of EQS analysis has shown in table 4 that a significant and positive relationship between all constructs. All indicators point to a good fit except the Chi-square has an inherent problem with sample size,

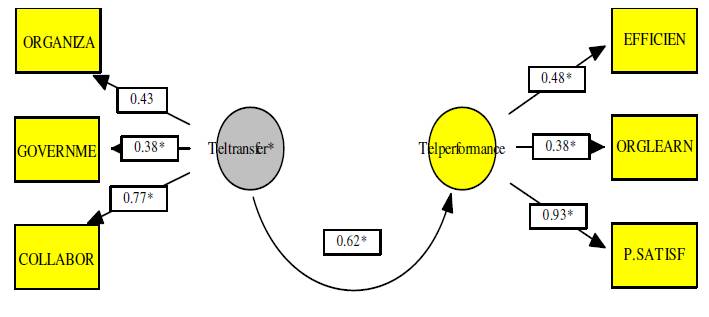
Fig 2. Testing the research model
All indicators point to a good fit except the Chi-square has an inherent problem with sample size, but its indictor to model fit when value was reduced from 55.3 to 26.1. GFI is 0.95, AGFI is 0.92, CFI is .98, FIT is .97, IFI is .98 that’s mean all of index above to acceptable value 9.0 and RMSEA is .03 below to acceptable value0.05. Thus, overall the data indicate a favorable fit for our conceptual model. Hypotheses test using a T value-squared- standardized solution, the result of EQS analysis has shown in table 4 that a significant and positive relationship between all constructs.
Discussion of Results
This study provides the inferences made from an instrument that is valid and reliable for the current study’s context. The measurement instruments include six constructs: 1. Organizational role, 2. Governmental role, 3.Collaboration, 4. 5. organizational learning 6. Patient satisfaction 7. efficiency. All the scales have been tested through rigorous statistical methodologies including KMO, convergent analysis, discriminant analysis, and confirmatory factor analysis.
All the scales meet reliability and validity requirements ,the development of these scales will greatly stimulate and facilitate theory development in this field. The supportive results enable the researcher to accept the main hypotheses accordingly; the conclusion will be drawn as can be seen from table 4.
Table 4 Results of testing hypotheses
Impact of Organizational Role on Telemedicine Transfer
The result shown that there is a positive relationship between the organizational role among healthcare organizations and telemedicine transfer (T value=2.10, direct effect = 0.43).
This result was consistent by Moore (2002) results which certain degree that organizational top management support, change management, and the nature of business process management can improve telemedicine transfer. Healthcare organization strategy intends to adopt telemedicine technology for sharing experiences and exchange ideas for certain cases to confirm diagnosis.
Impact of Governmental Role on Telemedicine Transfer
Governmental role is positively related to telemedicine transfer, the result of the statistical analysis indicates that there is a positive relationship between governmental role and telemedicine transfer (T value=2.03, direct effect = 0.38).
This result was consistent by Datta and Mbarika (2004) which concluded that governmental policy, security standards, and technology infrastructure are critical to telemedicine transfer. This is particularly important in this study, because telemedicine can be used to deliver healthcare to rural and underserved areas in Jordan.
Most respondents believe that unless basic infrastructure services such as power (electricity) access and costs have been addressed, the future of telemedicine in Jordan will still hang in the balance. Furthermore, most physicians believe that the digital divide between urban and rural areas is a major factor influencing the transfer of telemedicine in Jordan. Furthermore, the result reveals that a simple and economically affordable low-cost telemedicine system is an important factor for successful telemedicine transfer outcomes.
A possible reason for this explanation is that in rural areas in Jordan as in other developing countries, telephone networks, bandwidth and computers are scarce, in addition to low income levels and other conditions. This indicates how these various government regulations can affect on the way of delivering healthcare in the region.
The study also establishes that ICT infrastructural capabilities provide useful guidance to enhance telemedicine capabilities. General ICT policies are positively related to telemedicine transfer. This implies that public policy, including administrative reforms such as e-government and demographic factors such as health status indicators (Mortality rate and epidemiology dominated by infectious disease) are more important in the adoption of re-distributive polices that influence decision making in various public domains, whereas economic development policy is more important for development policies.
Thus, considering socioeconomic and demographic situations in ICT policies potentially influences changing the healthcare system for the better. The study findings show that data security policies are a significant positive influence on telemedicine implementation.
It is understandable that issues like privacy, confidentiality, availability and standards have emerged as significant factors with a great impact upon transferring and integrating telemedicine services into the traditional health system. This shows that telemedicine technologies begin working with more than one healthcare organization, since security and standards become a major risk issue.
This means that it is necessary for any telemedicine transaction (data, image, text) to have procedures established for security and standards when a telemedicine program gets into routine delivery of health care services.
Therefore, data security policies which should be addressed are those identified by the research community as pertinent issues for telemedicine transfer, such as privacy, confidentiality, availability, licensure, technology and standards and liability at both national and international levels. Furthermore, prior research shows that standardization of telemedicine is very important, and consequently increases the quality of transmitted data (image, data and text), and also reduces the total costs of transmission.
Therefore, for telemedicine to be transferred, security and standards are a major part of physicians’ concern. Even though the importance and necessity of these standards have been well received by the physicians, there is concern about their full implementation within the existing ICT infrastructure.
Impact of Collaborative Platform on Telemedicine Transfer
The hypothesized relationship between collaboration and telemedicine transfer was supported. The results shown a positive relationship between collaboration and telemedicine transfer (T value=3.16, direct effect = 0.77).
This was supported by Chen and Hirschheim (2002) study which founded that collaboration across professions, specialties, hospitals, hospital department and level of care with collaboration value is added, and clinical results are improved for many groups of patients. ICT leads to improved communication and collaboration.
The results also indicate that when physicians are exposed to technology from advanced nations, and they conduct their practice well, the desired outcomes are more likely to be success. However, physicians do not believe that exposure to advanced technology alone, especially by simply participating in conferences or workshops; will have much influence on telemedicine capabilities.
Most physicians in contrast believe that technology culturation has negative impacts on telemedicine capabilities, because of the “brain drain” and poor socioeconomic conditions of Jordan, especially when this is not conducive for them to return home. Another reason could be that physician exposure to a relatively technology-intense culture itself cannot be a solution for purposes of clinical care.
Even in the presence of correct diagnosis, treatment facilities and drugs are still an issue to improve the current situation. Moreover, the telemedicine technology readiness of all stakeholders, and proper implementation of telemedicine projects, is more important than a few physicians being exposed to the technology of industrial countries.
Impact of Telemedicine Performance on Efficiency and Effectiveness
The results shown a significant telemedicine outcomes on improving efficiency&effectiveness of health services (T value=2.34, direct effect = 048). This result indicates that telemedicine outcomes will improve the quality of care provided by achieving better performance timely and reducing the operational cost. This was harmonized by Rotvold (2003) study which founded that specialists can get initial views of the patients and they can make early decisions about the need for full office visits.
Impact of Telemedicine Performance on Organizational Learning
The result shown that there is a positive relationship between telemedicine performance and organizational learning (T value=2.08, direct effect = 0.38). Nonaka and Takeuchi(1985) stated that organizations learn not only from the competitors in their own industry, but also from firms in related and supporting industries. Both vertical and horizontal network learning is highly dependent on physical proximity (Porter, 1990). Overall, the rapid increase in the number of joint-ventures, R&D consortia, and strategic alliances in technology intensive industries is a clear sign of the growing importance of network learning for organizational competitiveness (Teece, 1992).
Impact of Telemedicine Performance on Patient Satisfaction
The hypothesized relationship between telemedicine performance and patient satisfaction was supported (T value=3.69, direct effect = 0.93). This result indicated that patient satisfaction for both the users and patients is important as an outcome of telemedicine implementation. Further, the results illustrated that using telemedicine technology in healthcare can improve the patient satisfaction and healthcare providers as well. In addition, using telemedicine technology in underserved areas can facilitate the accessibility of healthcare services.
Conclusions and Implications
This study constructs the affect of telemedicine transfer on telemedicine performance in healthcare services in Jordan through an empirical investigation study. It provides a strategic insights into telemedicine transfer in the healthcare sector.
As a result, study concluded that general organizational role, governmental role& ICT policy, and collaborative platform are significant factors affecting on telemedicine transfer. Also, the results concluded that organizational learning, patient satisfaction, and efficiency &effectiveness as an outcomes of telemedicine transfer are significant.
This study provides an illustration of the use of structural equation modeling technique for testing the validity of conceptual models as building blocks to theory development. One of the advantages of using SEM is its inherent capability to simultaneously test the measurement and structural models, which are derived from the conceptual model.
Finally, with respect to the study conclusions there are many other strategic issues that influence on telemedicine adoption in Jordan such as:
- Telemedicine must address the majority of the rural areas and especially at primary care level where most of the problems can be easily solved by getting a second opinion, such as radiology, dermatology, pathology, and ophthalmology.
- Telemedicine systems require a real commitment of all the involved parties, especially support from governments.
- Telemedicine services depend on the acceptance of physicians who must own the system; therefore their involvement is important in the development and implementation of the telemedicine project.
- Telemedicine technology should be user-friendly, and users must be well trained and supported to function effectively.
- Education in medical schools and arrangements of seminars and workshops for specialists in the use of technology is necessary.
Acknowledgements
Author is grateful to Dr. Ahmad Alkhateeb from King Hussein Center for the collecting data and suggestions on earlier drafts of this paper.
References
Alkhaldi, F.M.K. (2007). ‘Issues in research design,’ ALmanahjyah Journal, 6(1), 4-8, retrieved January 28, 2008, from www.aabfs.org
Bashshur, R. (2002). ‘Telemedicine and healthcare,’ Telemedicine Journal and e- Health, 8(3), 5-12.
Publisher – Google Scholar – PubMed
Bentler, P.M. (1989). ‘EQS: Structural Equations Program Manual, ‘ version 3.0. Los Angeles: BMDP Statistical Software.
Brown, R.L. (1986). ‘A comparison of the LISREL and EQS programs for obtaining parameter estimates in confirmatory factor analysis studies, ‘ Behav. Res. Methods Instr. Comput. 18 (4), 382—388.
Chen, W. and Hirschheim R. (2002).’A Paradigmatic and mythological examination of information systems research from 1991 to 2001, ‘Information System Journal, 14(3), 197-235.
Publisher – Google Scholar – British Library Direct
Chou, C, and Brauer, D. (2005). ‘Temperament and satisfaction with health status among Persons with rheumatoid arthritis, ‘ Clinical Nurse Speciaist, 19(5), 94-100.
PubMed
Craig, J. and Patterson, V. (2005). ‘Introduction to the Practice of Telemedicine, ‘ Journal of Telemedicine and Telecare, 11(1), 3-9.
PubMed
Datta, p., and Mbarika, V. (2004). ‘Are we there yet? An exploratory relationship between national information infrastructure expenditures, infrastructure development, and service-sector productivity, ‘Proceeding of the 37th Annual Hawaii International Conference on system Sciences (HICSS 04)-Track 8, Joreskog, K.G., Sorbom, D. (1989). ‘LISREL VII: A Guide to the Program and Applications, ‘ Joreskog and SorbomrSPSS, Chicago, IL.
Hair, J.F., Anderson, R.E., Tatham, R.L., and Black, W.C. (1998). ‘Multivariate data analysis, ‘ Fifth Edition, Macmillan Publishing Company, New York, NY.
Han, S. (2005). ‘Understanding user adoption of mobile technology: focusing on physicians in Finland, ‘ Doctoral dissertation.
Heinzelmann, P.J., Hapgood, J.E., Fleeger, E., and Lam, E. (2003). ‘Indian e-health initiative: technoconsultation service, ‘Harvard-MIT division of health sciences and technology. Cambridge, MA, p.7.
Hoyle, R. H. (1995). ‘The structural equation modeling approach: Basic concepts and fundamental issues, ‘ In Structural equation modeling: Concepts, issues, and applications, R. H. Hoyle (editor). Thousand Oaks, CA: Sage Publications, Inc., 1-15.
Hu, P.J.H., chau, P.Y.K., and Sheng, O.R.L. (2000). ‘Investigation of factors affecting healthcare organization adoption of telemedicine technology, ‘ Proceedings of the 33th Hawaii International Conference on System Sciences.
Huston, T.L. and Huston J.L (2000). ‘Is telemedicine a practical reality? ‘ Communications of the ACM, Vol. 43,pp. 91-95.
Publisher – Google Scholar – British Library Direct
Kaplan, B. (2000).’Culture counts: how institutional values affect computer use,’MD Computing, 17(1), 23-26.
PMid:10710929
Kifle, M., Mbarika, V., and Datta, P. (2006). ‘Interplay of cost and adoption of telemedicine in sub-Saharan Africa: the case of telecardiology in Ethiopia, ‘Information System Frontires, 8(3), 211-223.
Publisher – Google Scholar – British Library Direct
Kuntalp, M., and Akar, O.A. (2004). ‘Simple and low-cost internet-based teleconsultation system, ‘ Health Care Access and programs in Biomedicine Journal, 75(2), 117-126.
MacCallum, R.C., Browne, M.W., and Sugawara, H.M. (1996).’Power analysis and determination of sample size for covariance structure modeling, ‘ Psychological Methods, 1(5), 130-149.
Publisher – Google Scholar – British Library Direct – PubMed
doi:10.1037/1082-989X.1.2.130
Moore, S.K. (2002). ‘Extending healthcare reach: telemedicine can help spread medical Expertise around the globe, ‘IEEE Spectrum, 39(1), 66-71.
Publisher – Google Scholar
Nonaka, I. and Takeuchi, H. (1985). ‘Managing the new product development process: how the Japanese companies learn and unlearn, ‘ in: Clark, K. B., Hayes, R. H. and Lorenz, C. (Eds.), The Uneasy Alliance, Cambridge, MA: Harvard Business School Press.
Porter, M. E. (1990). ‘Competitive advantage of nations, ‘New York: Free Press.
Robinson, D.F., Savage, G. T., and Campbell, K.S. (2003). ‘Organizational learning, diffusion of innovation, and international collaboration in telemedicine, ‘Health Care Management Review, 28 (1), 68-78.
PMid:12638374
Rochelle, J., and Pea, R. (1999). ‘Trajectories from today www to a powerful educational infrastructure, ‘ Educational Researcher, 43(4), 22-25.
Publisher – Google Scholar – British Library Direct
Roothold G. (2003). ‘Telemedicine screening for diabetic retinopathy: staff and patient satisfaction, ‘ Journal of Telemed Telecare, 2(9), 109-13.
Publisher – Google Scholar – British Library Direct – PubMed
Scott, R.E., Ndumbe, P., and Wootton, R. (2005). ‘An e-health needs assessment of medical resident in Cameroon, ‘Journal of Telemedicine and Telecare, 11(1), 78-80.
Publisher – Google Scholar – PubMed
Sherry, L. Dieleman, and Karen B. (2004). ‘Primary health care teams: team members perception of the collaborative process, ‘ Journal of Interprofessional Care, 18(1), 105-114.
Stanberry, B., (2006). ‘Legal and ethical aspects of telemedicine, ‘ Journal of Telemedicine and Telecare, 12(4), 166-175.
Publisher – Google Scholar – British Library Direct – PubMed
Struber, J. (2004). ‘An introduction to telemedicine and email consultation, ‘ The Internet Journal of Allied Health Sciences and Practic.Retrieved October 22, 2004, from http://ijahsp.nova.edu/articieS/Vol2number3/telemedicine.html
Tan, J., Kifle Mbarika, V., and Okoli, C. (2005). ‘E-medicine diffusion: e-medicine in developed and developing countries, ‘ New York: Jossy-Bass press.
Teece, D. (1992). ‘Competition, cooperation and innovation,’ Journal of Economic Behavior and Organization, 3(1), 1-25.
Publisher
Wessner, M.Haake, and J.M., Titeze, D. (2002). ‘AN infrastructure for collaborative lifelong learning, ‘ Proceedings of the 3rd Hawaii International Conference on System Science.
Wootton, R. (2001). ‘Recent advance in telemedicine, ‘ British Medical Journal, 32(3), 557-560.
Wootton, R. (2003). ‘Success and failure in telehealth, ‘ 3rd International Conference on Successes and Failures in Telehealth. Queensland Australia.