Conclusion
In conclusion, it is suggested that Social CRM is a sound business strategy for the Irish Health Insurance Industry mainly due to its appeal to the young generation. This is one market segment every insurer would like to retain and grow due to its profitability. The Literature Review has revealed that in the absence of risk spreading, the insurer can get into a “death spiral” type of situation. In a community rated market, the insurer needs to have a sufficient number of low risk (young policy holders) to spread the risk of insuring high risk older policy holders.
The Literature Review has also shown why adverse risk selection is generally absent in an employee sponsored group segment and how marketing and administrative efficiencies can contribute to higher profit in this segment. However, insurers are also limited by their ability to interact directly with the policy holders in this segment as their interaction typically would be with an authorised person appointed by the employer for maintaining employees’ policies. This confines the insurer’s ability to cross-sell and up-sell its products and generate a higher profit. Here, a non-conventional and innovative approach is required to engage the policy holders. The Literature Review has also highlighted the importance of creating multiple channels of communication with customers, which will help them in choosing the most comfortable channel for communicating with the organisation. Social CRM could be an effective channel in this segment for policy holders to engage with the insurer directly without involving their employers.
This research has also pointed out how Social CRM can promote a sense of community among users. It has highlighted the advantages of creating an accessible support structure possibly maintained by an ambassador customer for creating trust, loyalty and perhaps, additional sales and revenue. This model has a likely application in larger employee sponsored group segments whereby a suitable policy holder within each large group can be assigned the ambassador customer role.
Experts agree on how easy it is to form target clusters in a Social CRM space and there is tremendous scope for its application in the Health Insurance business. For instance, Social CRM can also be used to create a sense of prestige and status among policy holders who buy premium plans by creating a community of premium plan customers who would be eligible for a superior service and additional incentives.
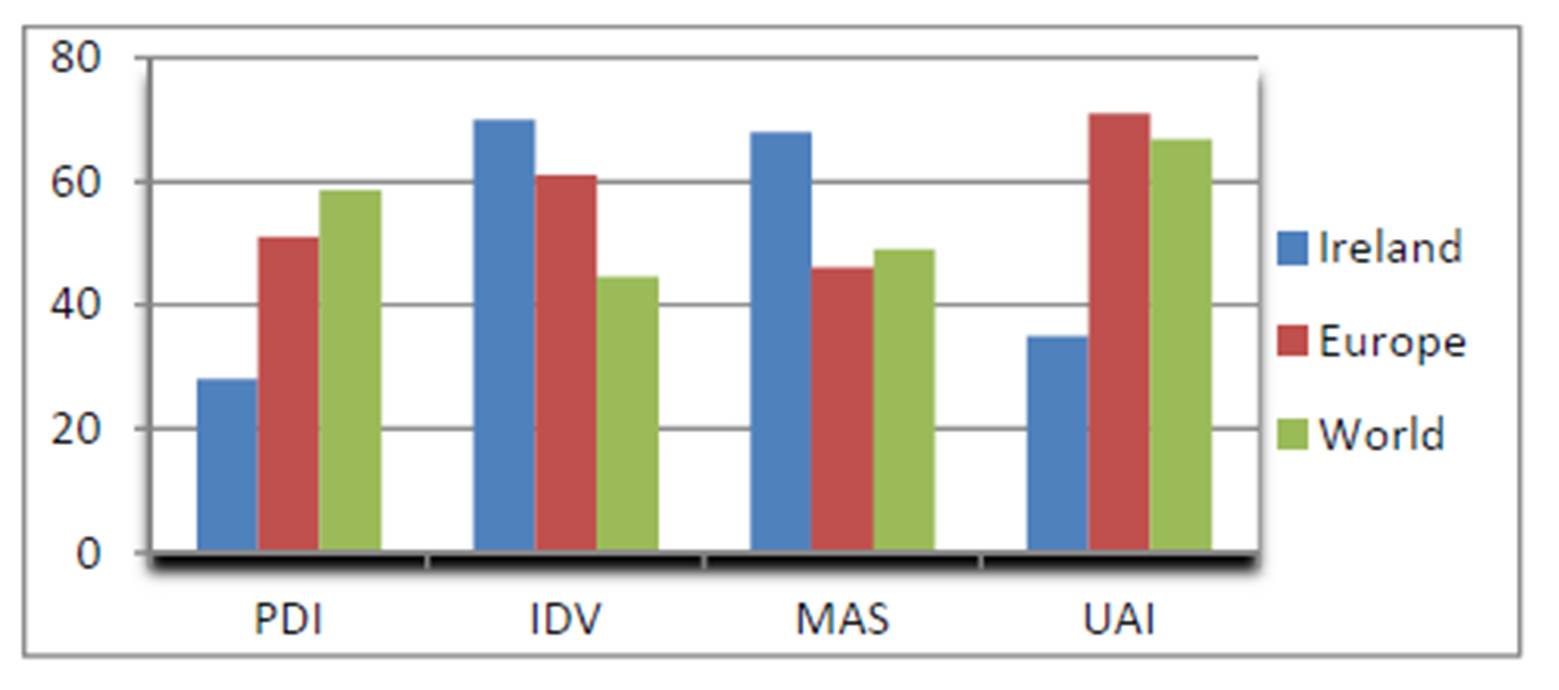
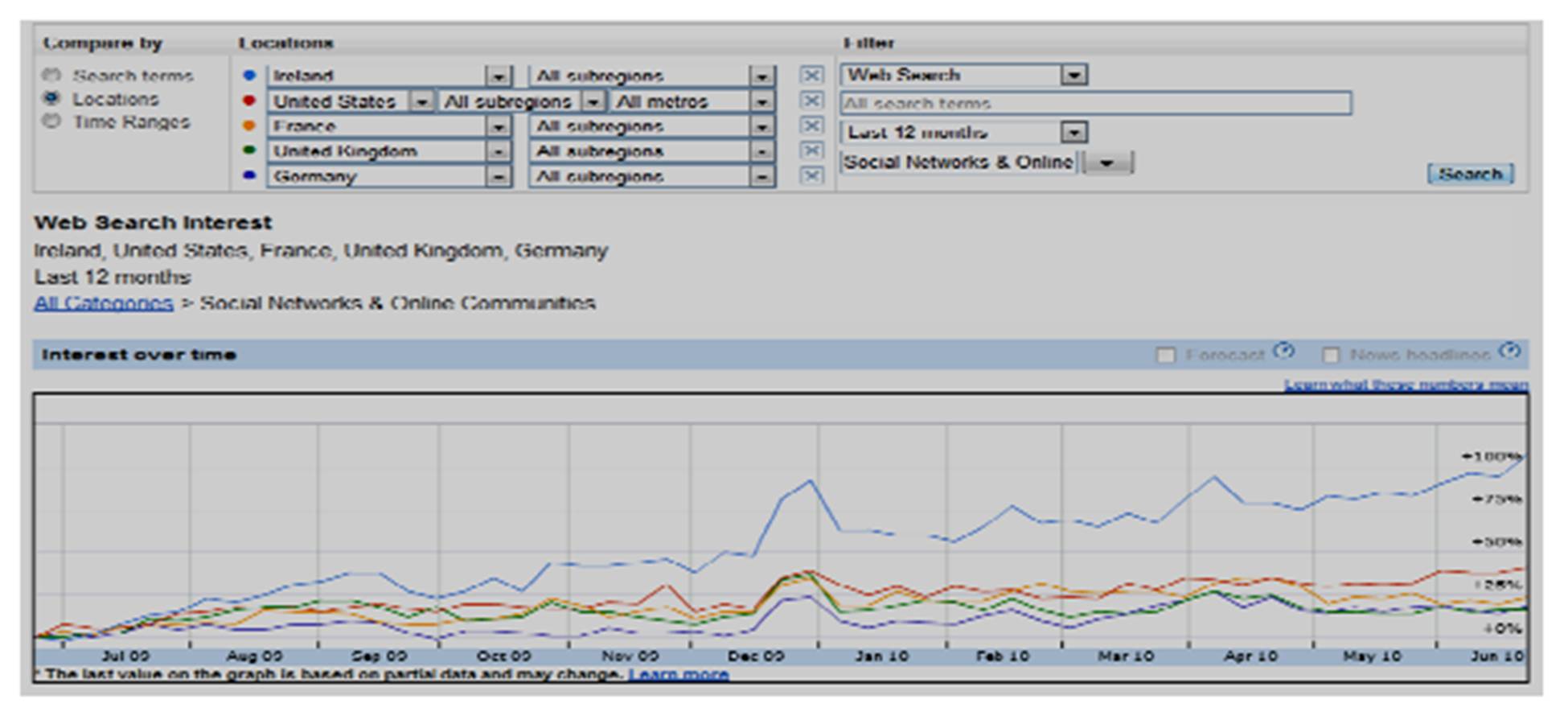
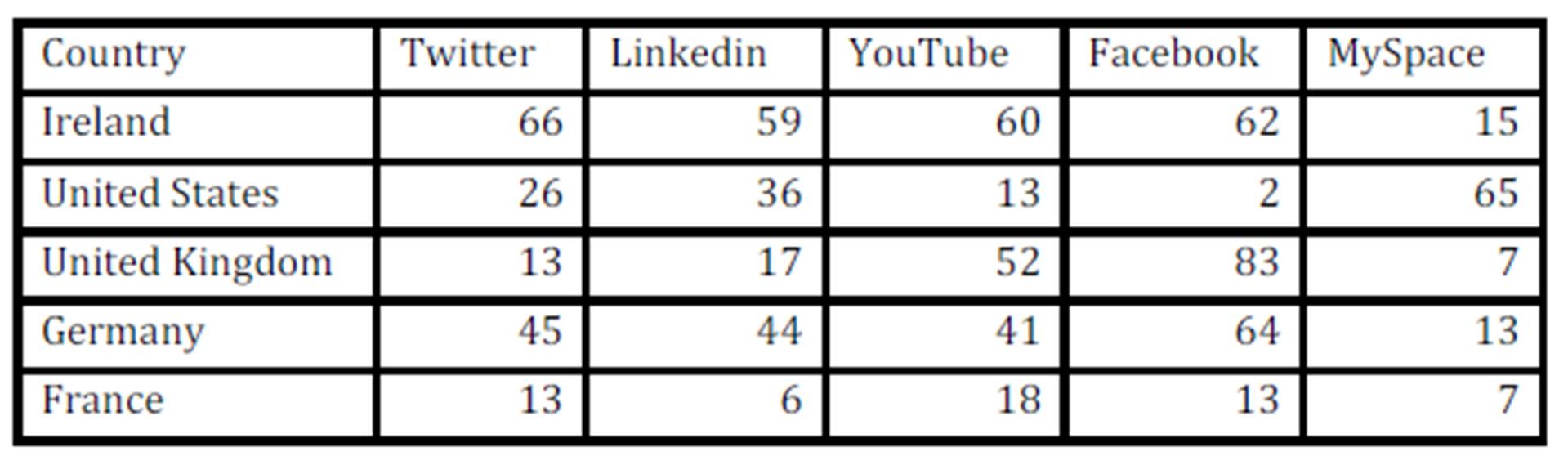
Hofstede’s cultural dimension studies have revealed that people in Ireland are very open to innovation and change and at the same time critical of irresponsible behaviour. This cultural aspect as well as the high social network usage in Ireland should encourage organisations to use Social CRM as an innovative channel for customer interaction as there is a higher probability that this initiative will find acceptance from its customers.
In recent times, a large number of insurance products were introduced by insurers in Ireland, targeting specific market segments. Competition alone cannot justify the number and frequency of these product launches. It is likely that the insurers are desperately looking for a winning formula to maximise the profit and as a result, tend to experiment by tinkering with the product and benefit design. The absence of an effective feedback loop from customer to insurer makes this process more time consuming and costly. This research has highlighted the possibility of improving this process by implementing Social CRM to facilitate receiving more timely feedback from online customer communities.
Organisations would like to receive timely market intelligence and there is a much higher expectation when Social CRM is implemented. However, experts have highlighted the need for creating the necessary structure and framework for processing this flow of information. It is likely that implementing Social CRM should activate this process within the organisation and improve an organisation’s overall capability in handling market intelligence and also strengthen their issue prevention/intervention mechanism.
Privacy and security are of utmost importance to the Health Insurance Industry. This was one of the concerns of experts while discussing the implementation of Social CRM in the Health Insurance Industry. It appears that this particular concern will limit the use of Social CRM as a Customer Support tool in the Health Insurance Industry. Insurers might want to provide this support on a one to one basis in a secure and confidential environment. However, there is a strong incentive to implement Social CRM in marketing, sales and market research activities. A Social CRM implementation is relatively less expensive than a number of other enterprise wide applications such as supply chain management, human resource management etc., as it would be usually built on top of an existing CRM module. It is unlikely that the cost will be a main concern in deciding whether or not to implement Social CRM; rather it would be the existence or absence of a justifiable business case. As such, in the case of the Health Insurance Industry, the business case is strong enough to consider its adoption in the current economic and regulatory environment.
In the social media space, the organisation and its customers coexist and the resultant vulnerability of the organisation could give rise to the fear of loss of control. It appears that this would be the nature of the game in the future and as pointed out by Howard Schultz, CEO of Starbucks, by facing up to this challenge, organisation can in fact benefit by gaining further trust from its customers.
References
1. American Academy Of Actuaries. 2001. Risk classification in voluntary individual disability income and long term care Insurance. Available: http://www.actuary.org/pdf/health/issue_genetic_021601.pdf [Accessed 17th March 2010].
2. Askool, S. S. & Nakata, K. Scoping study to identify factors influencing the acceptance of social CRM. Management of Innovation and Technology (ICMIT), 2010 IEEE International Conference on, 2-5 June 2010 2010. 1055-1060.
3. Band, W. & Petouhoff, N. L. 2010. Social CRM Goes Main Stream [Online]. Forrester Research Inc. Available: http://www.forrester.com/rb/Research/topic_overview_social_crm_goes_mainstream/q/id/55884/t/2 [Accessed 16 March 2010.
4. Barrett, S. D. 2000. The economics of competition in health insurance – The Irish case study, Trinity College, Dublin.
5. Bennet, J. T. 2008. Customer Relationship Management (CRM) Theory and Practice.
6. Bertiko, J,2008, Health Insurance Market Rating Practices, The RAND Corporation
7. Blinn, N., KUHNE, M. & NUTTGENS, M. Are Public and Private Health Insurance Companies Going Web 2.0? – A Complete Inventory Count in Germany. System Sciences (HICSS), 2010 43rd Hawaii International Conference on, 5-8 Jan. 2010 2010. 1-9.
8. Breaudun, D. D. & Donnellan, E. 2010. Sale of VHI will not keep prices down – FG. Irish Times, 29th May 2010.
9. Brian, B. N. N. 2006. The Interaction of Public and Private Health Insurance: Ireland as a Case Study. Geneva Papers on Risk & Insurance – Issues & Practice, 31, 633-649.
Publisher – Google Scholar
10. Brown, S. A. 2000. Customer relationship management : a strategic imperative in the world of e-business, New York ; Chichester, Wiley.
11. Buchmueller, T. & Dinardo, J. 2002. Did community rating induce an adverse selection death spiral? Evidence from New York, Pennsylvania, Connecticut. Available: http://www.jstor.org/pss/3083333 [Accessed 4th April 2010].
12. Buckley, D. 2010. Going Dutch: Fine Gael’s health plan. Irish Examiner, 27 Feb 2010.
13. Bundorf, M. 2010. The effects of offering Health Plan Choice within Employment based Purchasing Groups. Journal of Risk and Insurance, 77, 105.
Publisher – Google Scholar
14. C.K.Prahalad & Ramaswamy, V. 2000. Co-Opting Customer Competence. Customer Relationship Management. Hardward Business Review.
15. Candytech. 2010. Facebok Statistics Ireland [Online]. Candytech. Available: http://www.facebakers.com/countries-with-facebook/IE/ [Accessed 27th June 2010.
16. Canzer, B. 2006. E Business: Strategic thinking and practice. Houghton Mifflin Company.
17. Central Statistics Office Ireland. 2010. Consumer Price Index [Online]. Available: http://cso.ie/releasespublications/documents/prices/current/cpi.pdf [Accessed 20 June 2010.
18. Chollet, D. J. 1998. Understanding Individual Health Insurance Markets. Kaiser Family Foundation.
19. Claxton, G. 2002. How Private Insurance Works A Primer, Kaiser Family Foundation.
20. Collins, S. R. 2007. employer-based health insurance past, present, and future. hfm (Healthcare Financial Management), 61, 34-37.
21. Cone. 2008. 2008 Business in Social Media Study [Online]. Cone. Available: http://www.coneinc.com/content1183 [Accessed 7th July 2010.
22. Connelly, L. B. & Brown, I. I. I. H. S. 2010. Private Health Insurance in Australia: Community Rating, but at What Price(s)? Journal of Health Care Finance, 36, 80-92.
23. Coyle, R. G. 2004. Practical strategy : structured tools and techniques, Harlow, Financial Times Prentice Hall.
24. Davis, J. R. 2005. Right-Time Business Intelligence Optimizing the Business Decision Cycle [Online]. Beye Research. Available: http://www.beyeresearch.com/study/2149 [Accessed 18th July 2010.
25. De Mooij, M. & Hofstede, G. 2010. The Hofstede model. International Journal of Advertising, 29, 85-110.
26. Dealtry, T. R. 1992. Dynamic SWOT analysis : developer’s guide : when looking to the future look for the opportunities and threats and consider your strengths and weaknesses, Birmingham (Prince’s Corner, Harborne Park Road, Harborne, Birmingham. B17 0DE), Dynamic SWOT Associates.
27. Deloitte. 2009. Tribalization of Business Study. Available: http://www.deloitte.com/assets/Dcom-UnitedStates/Local%20Assets/Documents/TMT_us_tmt/us_tmt_TribofBusFlipBook_100609.pdf [Accessed 16 June 2010].
28. Department Of Health And Children 1999. White Paper – Private Health Insurance. Stationery Office.
29. Department Of Health And Children. 2010. Health Insurance Market Reforms – Qustion and Answers [Online]. Available: http://www.dohc.ie/issues/health_insurance/health_insuranceqanda.pdf?direct=1 [Accessed 5th July 2010.
30. Dones, J. 2010. Harney plans new risk equalisation measures. Sunday Tribune, 21st Feb 2010.
31. Dormont, B., Grignon, M. & Huber, H. 2006. Health expenditure growth : reassessing the threat of ageing. Available: http://hal.inria.fr/docs/00/18/16/05/PDF/Dormont-Grignon-Huber-HE.pdf [Accessed 23 April 2010].
32. Eggleston, K. 2000. Risk Selection And Optimal Health Insurance-Provider Payment Systems. Journal Of Risk & Insurance, 67, 173-196.
Publisher – Google Sholar
33. Etemad, H. & Chu, H. 2004. The dynamic impact of regional clusters on international growth and competition: some grounded proposition. International entrepreneurship in small and medium size enterprise. Edward Elgar Publishing Limited.
34. Feldman, R. & Dowd, B. 2000. Risk segmentation: goal or problem? Journal of Health Economics, 19, 499-512.
Publisher – Google Scholar
35. Fiona, R. 2009. Try to keep covered, if you can. The Irish Times (1921-Current File).
36. Foubister, T., S. Thomson, et al. (2006). Private medical insurance in the United Kingdom. Copenhagen, World Health Organization.
37. Fürhaupter, R. & Brechtmann, C. 2003. A survey of the Private Health Insurance in Germany. Available: http://www.actuaries.org/EVENTS/Congresses/Cancun/health_subject/health_28_furhaupter.pdf [Accessed 9th May 2010].
38. Gartner. 2010. Gartner Reveals Five Social Software Predictions for 2010 and Beyond [Online]. Available: http://www.gartner.com/it/page.jsp?id=1293114 [Accessed 8th July 2010.
39. Greenberg, P. 2009a. Managing Social Customers for Profit. CRM Magazine, 13, 48-48.
40. Greenberg, P. 2009b. Social CRM Comes of Age [Online]. Oracle. Available: http://www.oracle.com/us/products/applications/siebel/036062.pdf [Accessed 15th July 2010.
41. Greenberg, P. 2010. CRM at the speed of light : social CRM strategies, tools, and techniques for engaging your customers, New York, McGraw-Hill.
42. Grootaert, C. & Bastelaer, T. V. 2002. Social Capital from Definition to Measurement. Understanding And Measuring Social Capital. The World Bank.
43. Hall, M. A. 1994. Reforming Private Health Insurance The AEI Press
44. Health Insurance Authority. 2010a. Consultation Paper on Risk Equalisation in the Irish Private Health Insurance Market.Available:http://www.hia.ie/assets/files/publications/Risk_Equalisation/Consultation%20Paper%20on%20Risk%20
Equalisation%20June%202010.pdf [Accessed 10th July 2010].
45. Health Insurance Authority. 2010b. Health Insurance Comparison [Online]. Health Insurance Authority, Ireland. Available: http://www.hia.ie/ci/health-insurance-comparison/search-form/compare-against/ [Accessed 22nd July 2010.
46. Hitt, M. A., Ireland, R. D., Hoskisson, R. E. & Hitt, M. A. S. M. C. A. G. 2007. Management of strategy : concepts and cases, Australia ; United Kingdom, Thomson South-Western.
47. Hofstede, G. 2010. Greet Hofstede Cultural Dimensions [Online]. itim International. Available: http://www.geert-hofstede.com/index.shtml [Accessed 6th June 2010.
48. Hoppe, M. H. 2004. An interview with Geert Hofstede. Academy of Management.
49. Ignatius, A. 2010. “We Had to Own the Mistakes”. Harvard Business School Publication Corp.
50. Independent, I. 2008. Supreme Court Strikes Down Risk Equalisation Scheme. Irish Independent, July 16 2008.
51. Insight Statistical Consulting. 2008. The Private Health Insurance Market in Ireland.
52. Intel. 2010. Intel Social Media Guidelines [Online]. Intel Corpration. Available: http://www.intel.com/sites/sitewide/en_us/social-media.htm [Accessed 18th July 2010.
53. ISACA. 2010. Social Media: Business Benefits and Security, Governance and Assurance Perspectives [Online]. ISACA, USA. Available: http://www.isaca.org/Knowledge-Center/Research/Documents/Social-Media-Wh-Paper-26-May10-Research.pdf [Accessed 16th July 2010.
54. John, C., Michael, C., David, H., Tony, J. & Jimmy, J. 2002. Report of Working Group on Risk Equalisation [Online]. Society of Actuaries in Ireland. Available: http://web.actuaries.ie/Events%20and%20Papers/Events%202002/2002-05-01_Risk%20Equalisation/Risk%20Equalisation
%20Report%20-%202002.pdf [Accessed 15 Mar 2010.
55. Joseph Pine, Don Peppers & Rogers, M. 1995. Do you want to Keep your customers forever? Hardward Business Review, 103-115.
56. Kennedy, A. 1996. Private Health Insurance in Ireland. European Journal of Health Law, 3, 345-357.
Publisher – Google Scholar
57. Khushman, S., Todman, A. & Amin, S. The Relationship between Culture and E-business Acceptance in Arab Countries. Developments in eSystems Engineering (DESE), 2009 Second International Conference on, 14-16 Dec. 2009 2009. 454-459.
58. Kifmann, M. 2002. Insuring premium risk in competitive health insurance markets J.C.B.Mohr (Paul Siebeck) Tubingen.
59. Kumar, V., Petersen, J. A. & Leone, R. P. 2007. How Valuable Is Word of Mouth? Harvard Business Review, 85, 139-146.
60. Kwon, W. J. & Skipper, H. D. 2007. Risk management and insurance : perspectives in a global economy, Oxford, Blackwell.
61. Lancaster, G. & Reynolds, P. 2002. Marketing made simple. Elsevier Science.
62. Li, C. & Bernoff, J. 2008. Groundswell: Winning in a world transformed by social technologies, Harvard Business Press.
63. Mark, J. B. 1992. Evidence of Adverse Selection in the Individual Health Insurance Market. Journal of Risk and Insurance (1986-1998), 59, 13.
64. Marquis, M. S. & Buntin, M. B. 2006. How Much Risk Pooling Is There in the Individual Insurance Market? Health Services Research, 41, 1782-1800.
Publisher – Google Scholar
65. Marse, 2011. Dutchhealthcare reformatthe crossroads [Online]. Available: http://healthcarecostmonitor.thehastingscenter.org/files/2011/06/Maarse-Dutch-health-care-reform-at-the-crossroads-long-version1.pdf [Accessed 26th Feb 2014.
66. Mcdonnell, O. & O’donovan, O. 2009. Private health insurance as a technology of solidarity? The myth of ‘community’ in Irish healthcare policy. Irish Journal of Sociology, 17, 6-23.
Publisher – Google Scholar
67. Mechanic, D., LYNN B, R., C.CLOBY, D. & R.KNICKMAN, J. 2005. Policy Challenges in Modern Health Care. Rutgers University Press.
68. Microsoft. 2010. CRM and Social Networking: Engaging the Social Customer [Online]. Microsoft Dynamics. Available: http://crm.dynamics.com/docs/CRM_and_Social_Networks.pdf [Accessed 25th July 2010.
69. Morgan, R. M. & Hunt, S. D. 1994. The Commitment-Trust Theory of Relationship Marketing. Journal of Marketing, 58, 20.
Publisher – Google Scholar
70. Mossialos E, et al. (2002). Funding health care options for Europe, European Observatory on Health Care System Series, Open University Press
71. Moseley, G. B. 2009. Managing Health Care Business Strategy. Jones and Barrlett Publishers, LLC.
72. Nonnecke, B. & PREECE, J. 1999. Shedding Light on Lurkers in Online Communities.
73. Neuhaus, W, 1995, Community rating and equalisation, University of Copenhagen and MIRA Consultants Ltd (Sydney)
74. O’toole, A. 2010. State of the Net [Online]. Irish Internet Association in Collaboration with amas. Available: http://www.iia.ie/resources/resource/1/state-of-the-net/ [Accessed 27th June 2010.
75. Ofcom. 2008. Social Networking A quantitative and qualitative research report intoattitudes, behaviours and use [Online]. Office of Communcations, UK. Available: http://www.ofcom.org.uk/advice/media_literacy/medlitpub/medlitpubrss/socialnetworking/report.pdf [Accessed 03 Feb 2010 2010].
76. Office Of The Technology Assessment 1984. Medical Technology and cost of the Medicare program. Washington DC. US Congress.
77. Peppers, D. & Rogers, M. 2004. Managing customer relationships : a strategic framework, New Jersey ; [Chichester], Wiley.
78. Percival, G. 2010. Bid to allay concerns after Quinn Insurance administration. Irish Examiner, 31st March 2010.
79. Percy, A. M. 2000. Community rating and regulatory reform in health insurance markets. Ph.D. 9989636, University of Pennsylvania.
80. Petouhoff, N. L., Gliedman, C., Band, W. & Magarie, A. 2009. The ROI of Online Customer Service Communities [Online]. Forrester. Available: http://www.forrester.com/rb/Research/roi_of_online_customer_service_communities/q/id/48002/t/2 [Accessed 28th May 2010.
81. Postman, J. 2009. SocialCorp : social media goes corporate, Berkeley, CA, New Riders.
82. Prahalad, C. K. 2010. Best Practices Get You Only So Far. Harvard Business Review, 88, 32-32.
83. Preece, J. & Shneiderman, B. 2009 Transaction on Human-Computer Interaction: Motivating Technology-Mediated Social Participation.
84. Pricewaterhousecoopers. 2006. Healthy Choice 2006 – The Changing Role of Health Insurer [Online]. [Accessed 17th July 2010.
85. Quenqua, D. 2010. Starbucks’ Own Good Idea. Marketing News, 44, 23-25.
86. Reichheld, F. F. 1996. The quest for loyalty : creating value through partnership, Boston, MA, Harvard Business School Press.
87. Rosenau, P. V. & Lako, C. J. 2008. An Experiment with Regulated Competition and Individual Mandates for Universal Health Care: The New Dutch Health Insurance System. Journal of Health Politics, Policy & Law, 33, 1031-1055.
Publisher – Google Scholar
88. Ross, J. M. 2009. Abandon stocks, embrace flows – a conversation. O’Reilly radar.
89. Rubel, S. 2009. How to build social capital: Innovate early and often. Advertising Age, 80, 14-14.
90. Santerre, R.E. & Neun, S.P., 2012. Health Economics : Theories, Insights, and Industry Studies. Cengage Learning.
91. Sarner, A., Thompson, E., Mann, J., Dunne, M., Davles, J., Fletcher, C., Alvarez, G. & Maoz, M. 2010. Magic Quadrant for Social CRM [Online]. Gartner Inc. Available: http://www.lithium.com/pdfs/whitepapers/Gartner-MQ-Social-CRM-t4OR7RhY.pdf [Accessed 18 July 2010.
92. Schleifer, D. 2012, Expanding the definition of Social CRM [Online]. Available: http://www.destinationcrm.com/Articles/Web-Exclusives/Viewpoints/Extending-the-Definition-of-Social-CRM-84164.aspx [Accessed 23 Feb 2013.
93. Schneider, E. 2011, The Main Features of German Private Health Insurance [Online]. Available: http://www.actuaries.org/EVENTS/Congresses/Cancun/health_subject/health_16_schneider.pdf [Accessed 26 Feb 2013.
94. Shi, L. & SINGH, D. A. 2008. Delivering health care in America: a systems approach. Jones and Bartlett’s publications, Inc.
95. Simon, C. 2009. Underwriting profits in Irish insurance fall 83%. The Irish Times (1921-Current File).
96. Soat, J. 2010. 7 Questions Key To Social Networking Success. InformationWeek, 18.
97. Steinman, M. L. & Hawkins, M. 2010. When Marketing Through Social Media, Legal Risks Can Go Viral. Intellectual Property & Technology Law Journal, 22, 1-9.
98. Stickel, D., Mayer, R. C. & Sitkin, S. B. 2009. Understanding social capital: in whom do we trust? In: BARTKUS, V. O. & DAVIS, J. H. (eds.) Social capital: reaching out, reaching in. Edward Elgar Publishing Ltd.
99. Svendsen, G. T. & Svendsen, G. L. H. 2009. Handbook of social capital : the troika of sociology, political science and economics, Cheltenham, Edward Elgar.
100. Takahashi, M., Fujimoto, M. & Yamasaki, N. 2007. Active Lurking: Enhancing the value of inhouse online communities through the related practices around the online communities. Available: http://cci.mit.edu/publications/CCIwp2007-06.pdf [Accessed 25th May 2010].
101. The Health Insurance Authority. 2009. Submission of the Health Insurance Authority to the Oireachtas Joint Committee on Health and Children [Online]. Available: http://www.hia.ie/publication/other-advisory-reports.htm [Accessed 18 Feb 2010.
102. The Oecd Health Project 2004. Private health insurance in OECD countries, Paris, OECD.
103. Thompson, J. L. & Martin, F. 2010. Strategic management : awareness & change, Andover, South-Western Cengage Learning.
104. Thomson S & Mossialos E, 2010, Health Systems Governance in Europe, Cambridge University Press
105. Thomson, S. & Mossialos, E. 2009. Private health insurance in the EuropeanUnion. London School of Economics and Political Science.
106. Walsh, B. 2002. McEneaney judgement. Available: http://www.actuaries.ie/Events%20and%20Papers/Events%202002/2002-03-26_McEneaney%20Judgement/020326_
Brendan_Walsh.pdf [Accessed 25th April 2010].
107. Warfield, B. 2009. A Social CRM Manifesto: How to succeed with Social CRM Virtuous Cycle. helpstream.
108. Warshawsky, M. J. 1994. Projects of Health Care Expenditures as a Share of the GDP: Actuarial and Macroeconomic Approaches. Available: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1070007/pdf/hsresearch00053-0040.pdf [Accessed 23rd April 2010].
109. Williams, G. & Zinkin, J. 2008. The effect of culture on consumers’ willingness to punish irresponsible corporate behaviour: applying Hofstede’s typology to the punishment aspect of corporate social responsibility. Business Ethics: A European Review, 17, 210-226.
110. Witter, L. & Chen, L. 2008. The she spot : why women are the market for changing the world–and how to reach them, San Francisco, Calif., Berrett-Koehler ; London : McGraw-Hill [distributor].
111. Worthington, I. & Britton, C. 2009. The business environment, Harlow, Financial Times Prentice Hall.
112. York, E. B. 2010. Starbucks gets its Business Brewing again with Social Media. Advertising Age, 81, 34-34.
113. Zeisser, M. 2010. Unlocking the Elusive Potential of Social Networks [Online]. Mckinsey Quarterly. Available: https://www.mckinseyquarterly.com/Unlocking_the_elusive_potential_of_social_networks_2623 15 July 2010].