The thoracic skeleton is an osteocartilaginous frame which creates space for the principal organs of respiration and circulation. Intra-thoracic space is narrow above and broad below, flattened anteroposteriorly and longer behind (Datta, 1994). It is bound anteriorly by sternum, the rib cage forming the lateral wall and the vertebral column forming the posterior boundary (Williams, 2000). These three key components together form the frame work, giving oval contour to the thoracic wall in adults and rounded shape in infants (Openshaw, 1984). The primary function of the key components is to protect the vital organs like the lungs and the heart; they also contribute in the respiratory movements like bucket handle and pump handle movement where in rib and the sternum play an important role.
Intra-thoracic space has a limited area to accommodate numerous structures including heart, lungs and mediastinal structures. Openshaw (1984) and Haller (1987) explained about the alteration in the intra-thoracic space and its dimensions may be seen due to positional change of sternum in the front, ribs on the either side or vertebral column behind, as seen normally in the aging process from early infancy to adulthood or in the cases of anterior chest wall and spine deformities. According to Wachtel et al. (1956), compromise in the intra-thoracic space beyond a particular limit may compress upon the cardiac and lungs there by reducing the cardiac output and the lungs’ volume especially during exercises. Chest wall deformities may be a disease in which different morphological types can be distinguished following morphological alterations of the sternum, the sterno-costal segments and the ribs (Willtal et al., 2011).
However, there are very limited data in the literature on the influence of the sternal position on thoracic shape. The present article would be the first of its kind in an attempt to include the sternum as a key component in framing the thoracic shape and dimension. The aim was on the measurement of the internal thoracic dimensions in normal subjects with focus on manubriosternal joint angulation in individuals of different age groups so as to understand and differentiate the normal aging changes of the skeletal components with chest wall deformities; and finally an attempt to provide a baseline value for internationally accepted vertebral and Haller’s index in Indian population so as to objectively categorise the chest wall as normal or deformed based on the findings.
Materials and Methods
The present study was conducted from September 2011 to August 2013 in two hospitals; K S Hegde medical academy, Mangalore and K V G Medical College and Hospital, Sullia. The study protocol was approved by the ethical committee of NITTE University in September 2011. Informed consent was obtained for the particular study. 80 subjects with a chest considered to be morphologically normal on physical examination were studied. Subjects were again divided into two groups:
Group 1: 36 subjects with age ranging from 1- 18 years with median age of 10 years (pre-pubertal group)
Group 2: 44 subjects with age ranging from 19- 40 years with median age of 25 years (post-pubertal group)
The criteria for inclusion of normal subjects were as follows:
a- absence of depression or protrusion of the central portion of the anterior thoracic wall in relation to the costal cartilage during physical examination;
b- CT scan of the thorax due to another type of clinical investigation;
c- Age ranging from 1 to 40 years and patients excluded were with any affection that might interfere in the normal morphology of the thoracic cage (Rebies., 2007).
Discussion
Since changes of chest wall constitute the main anatomical component of chest wall deformities, radiological chest examination enables the assessment of chest condition, deformation, degree and shape. It also allows planning the operation, predicting its results and treatment outcome (Haller, 1987). Computed tomography has become a very useful tool in current diagnostics with an advantage of repeatability and the possibility of high resolution and multi-dimensional images (especially including bone structures), enabling measurements in unlimited planes (Given et al 2004, Grimby et al., 1968 and Howard., 1949). To our knowledge, internal thoracic dimension measurement in the Indian population has not been investigated so far, either with traditional radiograms or with the use of computed tomography.
Manubrium and the body of sternum along with the ribs and the vertebral column are among the key components, which provide chest the contour, which was rounded during infancy and changes to oval or reniform shape in adults (Openshaw, 1984). Apart from the positional variation of sternum during the normal aging process of chest wall, even during the development of pectus anomalies the sternum is usually regarded as the culprit. The advocates of this hypothesis believe that the displacement of the sternum occurs first, followed by changes in the costal cartilages, which have no option but to follow the sternum in its displaced position. In Pectus excavatum, sternal depression usually begins at the junction of the manubrium and sternum (gladiolus) and becomes progressively deeper toward the xiphoid process. The costal cartilages are elongated, distorted, and sometimes fused together. If the sternum is pushed inward, the result is pectus excavatum, if it is pushed outward, pectus carinatum develops (Francis et al., 1974).
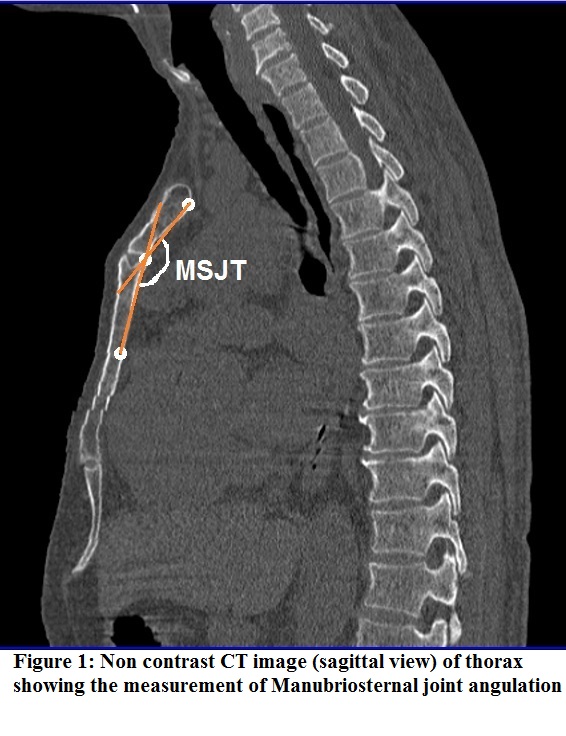
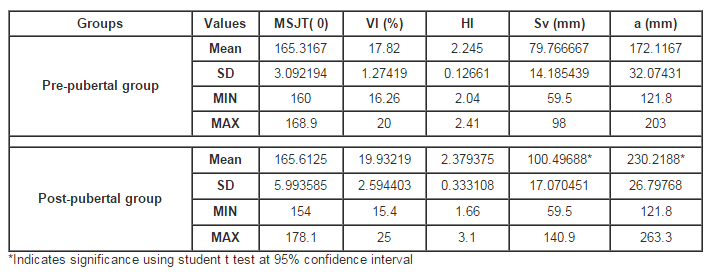
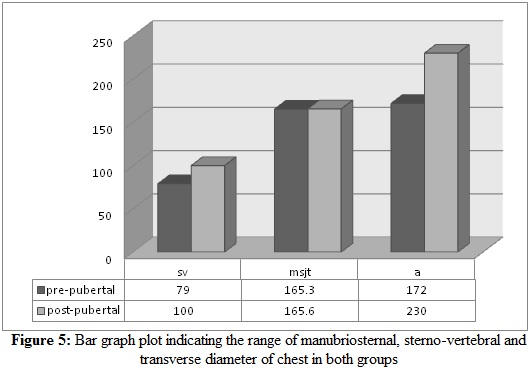
With the evidence supporting the importance and involvement of manubriosternal joint in normal and deformed chest wall, we have begun by measuring the joint angulation in individuals with normal chest wall, so as to provide a baseline range for manubriosternal joint angulation in two important age groups, pre-pubertal and post-pubertal age groups. Scanty yet vital literature was retrieved to support the present article; the article by Constantine (1974), measuring the Manubriosternal joint movements during respiration in young athletes which showed an angulation of 165.30±7.19 in females, 166.35±7.38 in males. Our reports showed a range of 155 — 175 (0) and average of 165 (0) in controls, manubriosternal joint angulation in children (pre-pubertal) and adults (post-pubertal group) showed almost similar angulation, indicating the early positioning between manubrium and sternebrae which remains unaltered with aging except in conditions with affected chest wall such as pectus carinatum and excavatum (Willtal, 2011). Manubriosternal joint angulation between both sexes showed almost similar values which was not significant.
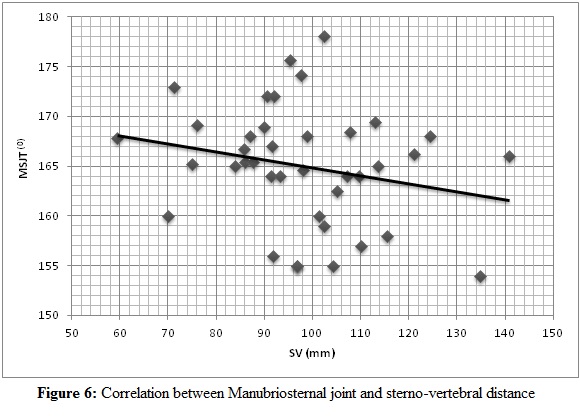
Change in the manubriosternal joint angulation does alter the internal thoracic dimensions. To understand the influence of the positional variation of the manubrio-sternal joint on chest wall, components of internal thoracic dimensions like sterno-vertebral distance and transverse diameter were included. As the four sternebrae fuse to form a single body of sternum, the position of manubrium in relation to first sternebrae usually remains unaltered, but the lower portion of the body of sternum changes from convex forwards to a straight segment, gives a better understanding of the change in the shape of thoracic wall in adults when compared to children; thoracic wall in pre-pubertal age undergoes changes in a slower pace until pubertal growth spurt. There was a positive correlation between the two components, i.e. increase in sterno-vertebral distance also changes the transverse diameter of the chest wall.
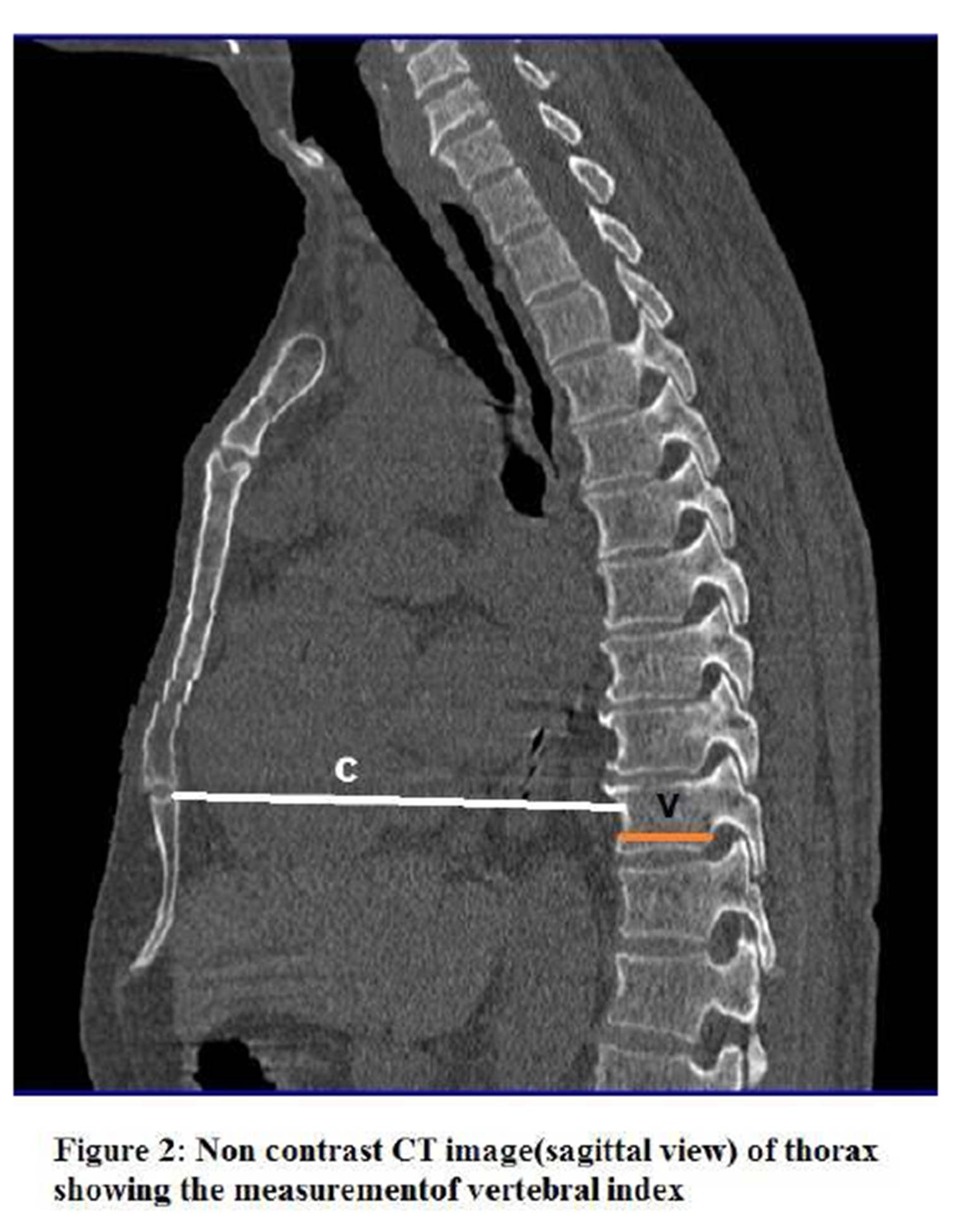
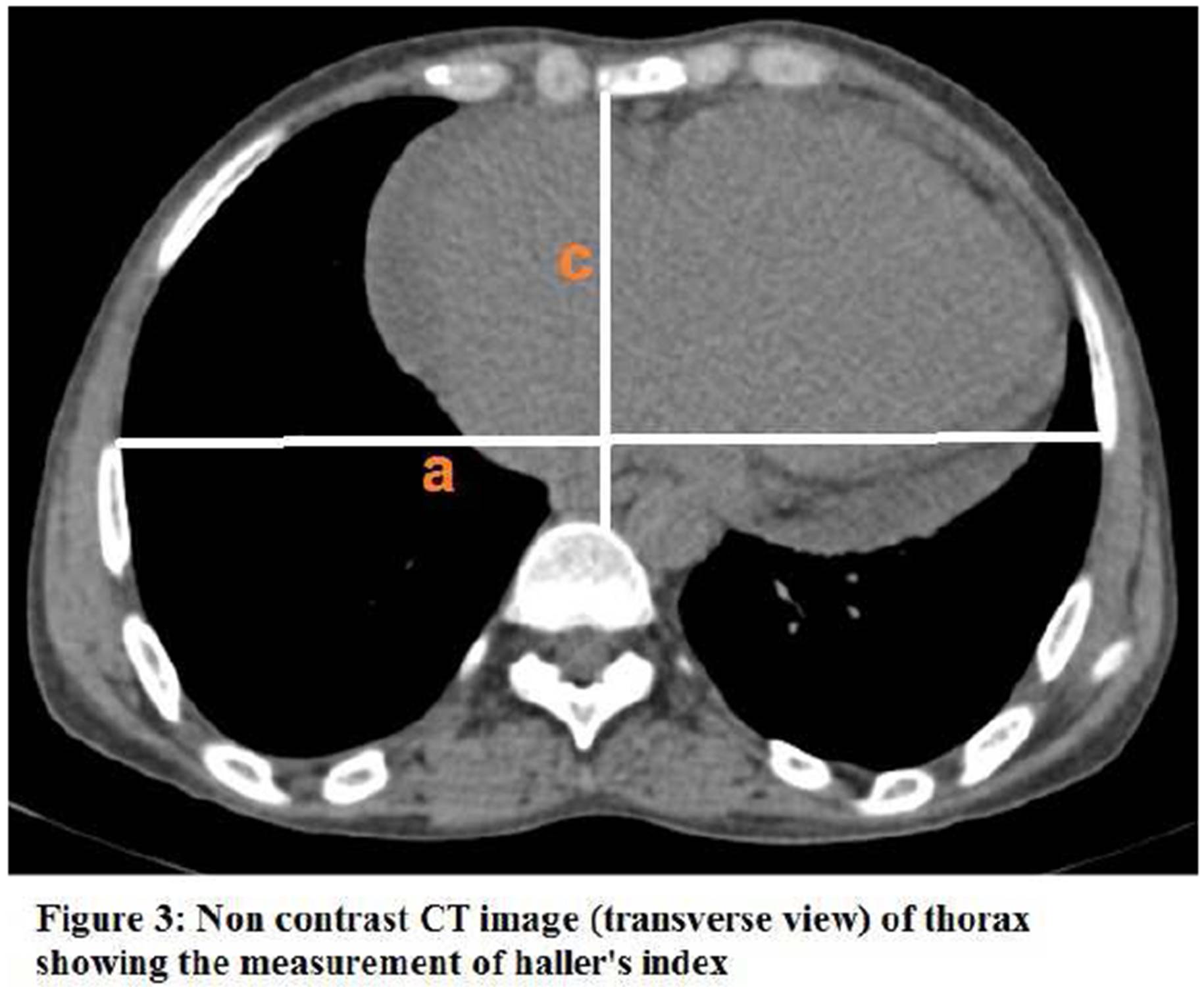
Radiological indices like vertebral index and Haller’s index was also included in the present report so as to complete the overall involvement of all the components forming and affecting the contour, shape of the chest wall and its dimensions. In the present study, internationally accepted Haller’s index and vertebral index were measured in individuals with normal chest contour, so as to provide the range to classify or categorize the chest wall as normal or deformed, and if deformed to classify it as mild, moderate or severe deformed chest wall. Haller’s index showed wider range of 1.6 to 3.1 with mean of 2.3 in post pubertal group and vertebral index around 15.4 to 25 with average of 19% in subjects whose chest wall contour was normal on physical examination. Haller et al (1987) have mentioned that the severity of the pectus deformity can be assessed by the pectus index. A pectus index greater than 2.5 is significant and an index greater than 3.2 is generally regarded as a severe deformity. Klida et al (2007) has mentioned about the pre—operative CT and x ray assessment of chest deformation and has provided radiological indices ; VI ≥26, HI ≥ 3.1 as the indications for the surgical corrections .
This study has provided base line values for important radiological indices like sterno-vertebral distance, transverse diameter, Vertebral Index and Haller’s Index, so as to objectively categorise chest wall as normal or deformed based on the findings in the Indian population.
To conclude, alterations in the geometric dimensions and shape of thoracic wall, change in the pattern and the mechanism of respiration are influenced not only due to change in the inclination of the rib and the curvature of the vertebral column, even the position of the sternum plays a pivotal role. Awareness of the basic anatomical changes in the thoracic wall and respiratory physiology with aging would help clinicians in better understanding and interpreting the deformity, thereby differentiating between the normal changes of an aging chest and the chest wall deformation.
Conflict of interest: none declared
References
1. Constantinescuo, A. (1974). “Biomechanical Study on Joint Range of Motion of Manubriosternal joint in adults”. Arch Ana, 57:153-199
2. Datta, A K. (1994). “Essentials of human anatomy. Thorax and abdomen”. 3rd edn. Current Books International, Calcutta, pp 80—86.
3. Francis Robicsek, Harry, K. Daugherty, Donald, C. Mullen. (1974) “Technical Considerations in the Surgical Management of Pectus Excavatum and Carinatum”. Ann thorac surg; volume 18: number 36
Publisher – Google Scholar
4. Givens, M.L. Ayotte, K. Manifold, C. (2004). “Needle thoracostomy: implications of computed tomography chest wall thickness”. Academic Emergency Medicine 11(2): 211-213
Publisher – Google Scholar
5. Grimby, G. Bunn, J. Mead, J. (1968). “Relative contribution of rib cage and abdomen to ventilation during exercise”. J Appl Physiol. 24:159—166.
Google Scholar
6. Haller, J A. Kramer, S S. Lietman, A. (1987). Use of CT scans in Selection of Patients for Pectus Excavatum Surgery: A prelminary report. J Pediatr Surg; 22:904-906
Publisher – Google Scholar
7. Howard, P. Bauer, A. (1949). “Irregularities of breathing in the newborn period”. Am J Dis Child 77:592-609
Google Scholar
8. Kilda, A. Basevicius, A. Barauskas, A. (2007). “Radiological assessment for the children with pectus excavatum.Indian” .j. pediatric , feb;74(2);143-7
9. Luc Derveaux, Ignace Clarysse. (1989). “Preoperative and Postoperative Abnormalities in Chest X-ray indices and in Lung Function in Pectus Deformities”. Chest journal;95:850-56
Google Scholar
10. Openshaw, P. Edward, S. Helms P. (1984). “Changes in rib cage geometry during childhood”. Thorax 39:624-627
Publisher – Google Scholar
11. Rebeis, E B. Campos, J R. Fernandez, A. Moreira, L F. Jatene, F B. (2007). “Anthropometric index for pectus excavatum”. Clinics, 62 (5):599-606
Publisher – Google Scholar
12. Wachtel, F W. Ravitch, M M. Grishman, A. (1956). “The relation of pectus excavatum to heart disease”. Am Heart J; 52: 121-37.
Publisher – Google Scholar
13. Willital, G.H., Saxena, A.K., Schütze, U, Richter W. (2011). “Chest-deformities: a proposal for a classification”. World J Pediatr ;7(2):118-123
Publisher – Google Scholar
14. Williams, L. (2000). “Gray’s anatomy, 38th Edn. Chruchill Livingstone”, pp 510-450