1Sydney Head & Neck Cancer Institute and Department of Otolaryngology, Royal Prince Alfred Hospital, Camperdown, Australia
2Sydney Head & Neck Cancer Institute, Royal Prince Alfred Hospital, Camperdown, Australia
Volume 2013 (2013),
Article ID 224147,
International Journal of Case Reports in Medicine,
4 pages,
DOI: 10.5171/2013.224147
Received date: 7 May 2013; Accepted date: 23 May 2013; Published date: 24 June 2013
Academic Editor: Jonathan W. Serpell
Cite this Article as:
Tsu-Hui (Hubert) Low and Anthony Clifford (2013), "Non-Recurrent Laryngeal Nerve and Aberrant Vasculature," International Journal of Case Reports in Medicine, Vol. 2013 (2013), Article ID 224147,
DOI: 10.5171/2013.224147
Background: The incidence of non-recurrent laryngeal (RLN) nerve is around 0.5%. Injury to the nerve results in significant morbidity. Methods and Results: A case of a 63-year old lady with a non-RLN and an aberrant subclavian artery was described. A successful thyroidectomy was performed with subcapsular dissection and identification of the RLN medially. Embryogenesis and anatomical variations of the non-RLN were reviewed, and their clinical importance was discussed. Conclusions: It is important for surgeons who regularly perform thyroidectomies to be aware of the association between aberrant subclavian artery and the presence of non-RLN.
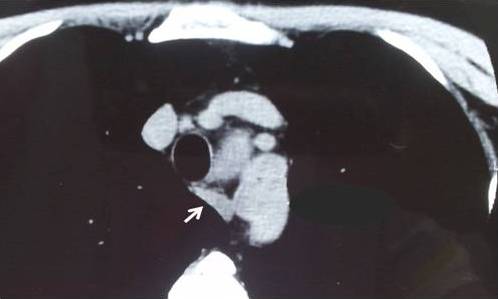
A healthy 63 year old lady presented with obstructive symptoms from a multinodular goitre. Preoperative CT of the neck confirmed a retrosternal multinodular goitre (Figure 1), as well as an aberrant right subclavian artery (Figure 2).
Figure 1: Coronal CT Showing the Retrosternal Extension of Multinodular Goitre (Arrow).
Figure 2: Axial CT Showing an Aberrant Right Subclavian Artery (Arrow).
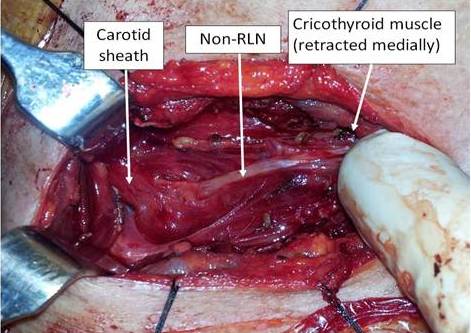
A careful subcapsular total thyroidectomy was performed after division of strap muscles. A right non-recurrent laryngeal nerve (RLN) was identified medially, near the cricothyroid muscle, and traced laterally. The nerve was noted to emerge deep to the carotid artery (Figure 3). Four parathyroid glands were identified and preserved. On postoperative day one, the PTH was 5.2pmol/L with corrected calcium of 2.28 mmol/L. The recovery was uneventful and the voice was normal. The patient was discharged on day 2 after drain removal. Histopathology confirmed benign multinodular goitre measuring 103x68x 52mm and 98x36x52mm for both left and right lobes, respectively.
Figure 3: Intraoperative Photo Showing the Right Non-Recurrent Laryngeal Nerve, Arising Deep to the Carotid Sheath and Coursing toward the Cricothyroid Muscle.
Discussions
Injury to the RLN from thyroidectomy occurs in about 1% of cases, resulting in significant morbidity. The incidence of non-RLN is reported to be 0.54%; this leads to increased risk of inadvertent injury to the nerve in inexperienced hand (Toniato et al., 2004).
This case highlights the fact that when an aberrant vasculature is noted amongst patients undergoing thyroid surgeries, the surgeon needs to be prepared for the possibility of a non-RLN.
Embryologically, right subclavian artery is formed from the 4th arch structure and RLN is formed from the 6th arch structure. During embryogenesis, the heart descends, dragging the 6th arch structure (including RLN). Anomaly of subclavian artery on the right side leads to the failure of the right RLN to descend (Defechereux et al., 2000 and Abboud and Aouad, 2004). Right subclavian artery in these cases often courses behind the oesophagus, the incidence of which is reported to be around 0.5%—2% (Campbell et al., 1991, Casal et al., 2010, and Toniato et al., 2004). It is also important to note that a small proportion of these patients with retro-oesophageal subclavian artery (with normal-sized thyroid gland) will complain of symptoms of dysphagia (Cannon, 1999 and Casal et al., 2010). Therefore, clinicians will also need to counsel their patients appropriately in regard to the possibility of persistent dysphagic symptom amongst patients with concurrent retro-oesophageal subclavian artery and multinodular goitre.
Toniato et al. (2004) reviewed their series of 6000 thyroidectomies (where 31 have non-RLN). They reported three variations of the non-RLN; the non-RLN could be closely related to the superior thyroid vessels (type 1), parallel and over the trunk of the inferior thyroid artery (type 2a), or parallel but under or between the branches of the inferior thyroid artery (type 2b) as seen in Figure 4 (adapted from Nakatani et al., 1998, Toniato et al., 2004, and Abboud and Aouad, 2004).This schematic drawing also highlights the point that despite all the known variations, the position of the non-RLN is constant in its medial position, close to the cricothyroid muscle; therefore, routine identification of the RLN medially where the anatomy is more constant could minimize the risk of injuring the non-RLN during dissection.
Figure 4: Schematic Diagram of the Three Variations of Non-RLN. The Course of the Non-RLN is Variable Lateral to the Thyroid Gland but Remains Constant at Its Medial Position (Red Circle).
In conclusion, surgeons and trainees who regularly perform thyroidectomy should understand the association between vascular anomaly and non-RLN. By adhering to the technique of subcapsular dissection and identification of the RLN close to the cricothyroid muscle, the risk of injuring the non-RLN could be minimized.