Riyazuddin Shamsul Haq Ansari and Hany Murtada Al Hasan
King faisal hospital, Intensive care department, Holy Makkah, Kingdom of Saudi Arabia
Volume 2013 (2013),
Article ID 624655,
International Journal of Case Reports in Medicine,
5 pages,
DOI: 10.5171/2013.624655
Received date: 28 July 2013; Accepted date: 6 September 2013; Published date: 30 September 2013
Academic Editor: Pedro Braga-Neto
Cite this Article as:
Riyazuddin Shamsul Haq Ansari and Hany Murtada Al Hasan (2013), "Parkinson’s Disease with Sigmoid Volvulus," International Journal of Case Reports in Medicine, Vol. 2013 (2013), Article ID 624655, DOI: 10.5171/2013.624655
PARKINSON’s disease is a disorder of somatic motor activity, due to degenerative changes in the basal ganglia. It is a chronic and progressive disorder. Chronic constipation and loss of intestinal tone is the visceral outcome of this disease. These gut manifestations tend to be further aggravated by the drugs used to decrease the somatic muscular rigidity and tremor. The outcome sometimes turns into sigmoid volvulus. The exact etiology of sigmoid volvulus in Parkinson’s disease (PD) remains unclear. Early recognition and treatment of constipation in PD patients may alter complications like sigmoid volvulus. Treatment of sigmoid volvulus in PD patients ranges from endoscopic detorsion to sigmoid colectomy with colostomy.. Herein, we describe an elderly patient with Parkinson’s disease who presented with sigmoid volvulus and underwent colectomy and colostomy.
The Sigmoid colon is the frequent site of volvulation and presents with symptoms of constipation, severe abdominal pain, and a distended abdomen. The incidence of Sigmoid volvulus ranges from 5% to 7%. Motility disorders like swallowing disorders, bowel dysmotility, gastro paresis, and anorectal dysfunction are common in PD2. The premotor phase of PD includes autonomic dysfunction, sleep disorders, and neuropsychiatric disturbances. Autonomic dysfunction like constipation can precede the motor symptoms by many years. Constipation can be explained by Lewy bodies and α-synuclein deposits in the dorsal vagus nucleus and enteric plexus before involving the substantia nigra. Neuropsychiatric disorders are associated with 71% of patients of sigmoid volvulus3. Many cases are self-limiting and around 50% of patients provide history of past episodes3. We describe a patient known to have PD with past two times of recurrent bowel dilatation associated with sigmoid volvulus, but he was treated conservatively, and now again presented with sigmoid volvulus. We reviewed the literature regarding volvulus in patients with PD and treatment of this condition. Our aim in presenting this article is to make the physicians aware that gastrointestinal complications of PD should be kept in mind while patients are in treatment. Case Report
A 72 year old male patient with known case of Parkinson’s disease on Anti-parkinsonian medication (Pramipexole -0.5 mg TID, Amantadine -100 mg BID, Sinemet -25mg/100 mg TID and Citalopram -10 mg OD,) since 10 years, presented with history of severe abdominal pain with distension and constipation since 2 days. The patient had the same complaint 3 years as well as 3 months before. His vital signs were as follows: Temperature 37ËšC, pulse 96/min, blood pressure 140/80 mm Hg, and respiration 22/minute. Laboratory investigations were as follows: white blood count -5230/cmm, hemoglobin – 16.5 g/dL, platelets – 1.52 lacs/cmm, random blood sugar – 104mg/dl, urea – 12 mg/dl, creatinine – 0.7 mg/dl, sodium – 140 mEq/L, potassium – 4.5 mEq/L, Aspartate aminotransferase – 57IU/L, alanine aminotransferase – 25 IU/L, alkaline phosphatase – 66 IU/L. Coagulation profile was within normal range (prothrombin time — 13.5 s, partial thromboplastin time — 57.0s, INR — 1.30). Cardiovascular examination was as follows: S1, S2 present with normal sinus rhythm. Respiratory examination was as follows: bilateral equal air entry, and normal vesicular breath sounds. His abdomen was markedly distended, more on the right side. There were increased bowel sounds. The CNS examination showed÷ the patient to be conscious, with Cogwheel rigidity at the wrist joints and lead pipe spasticity at the elbow joints. He was able to walk with a festinating gait. Resting tremors were present in the hands bilaterally, but more in the right side. There was Jaw tremor with increased salivation. There was no gaze palsy. As per Hoehn and Yahr, the patient was having stage 4 of disease. X-ray of the abdomen showed hugely dilated sigmoid colon (Figure 1).
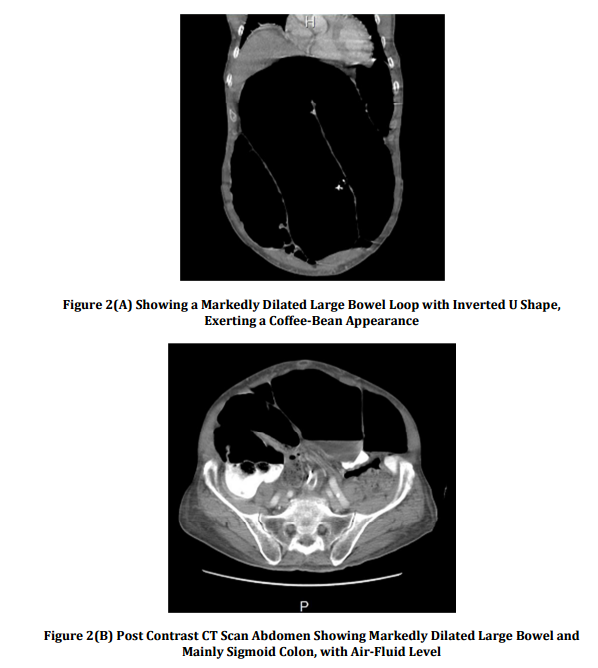
The patient underwent CT scan of the abdomen, which showed (figure 2a) a markedly dilated large bowel loop with inverted U shape, exerting a coffee-bean appearance. Post contrast CT scan abdomen (figure2b) showed markedly dilated large bowel and mainly sigmoid colon, with air-fluid level.
The patient was diagnosed with sigmoid volvulus, and he underwent colectomy with colostomy. He was weaned from ventilator and later on discharged from the hospital.
Discussion
Several reports have shown that constipation is present in 50% of patients and may develop at the pre-motor phase of PD4. The severity is more in long standing duration of PD. Decreased physical activity with a decrease in swallowing saliva may play a role in constipation and medications used to treat PD like anticholinergic drugs, and COMT inhibitors can give rise to diminished bowel motility. In PD, colonic transit time is prolonged in all segments of the colon5. Constipation may result from both peripheral and central nerves. Constipation can be explained by Lewy bodies and α-synuclein deposits in the dorsal vagus nucleus and enteric plexus before involving the substantia nigra. Depletion of dopamine in the central nervous system and dopaminergic myenteric neurons is present in PD. Vomiting occurs late, but if present from the start, then it is associated with high mortality6. In sigmoid volvulus there is twisting of the sigmoid around its mesenteric axis with ot without associated strangulation of the blood vessels at the base of the mesentery. Chronic constipation leads to elongation and redundancy of the colon. It can be a life -threatening condition with high mortality rates of up to 50%. The diagnosis of volvulus is based on physical examination and an abdominal X-ray showing a typical “coffee bean” shaped sigmoid. If in doubt, an abdominal CT scan must be ordered, which will show a dilated colon with air-fluid level. But, colonoscopy remains the best intervention to visualize the obstructive colonic moments. Endoscopy allows immediate treatment. If constipation is the main cause, the primary focus should be on medical prophylactic treatment with laxatives. However, if patients with PD have recurrent sigmoid volvulus, surgery remains the first choice of treatment. Early aggressive treatment of constipation with dietary adjustments, physiotherapy, prostaglandins, bulk-forming agents, and laxatives should be the aim in all PD patients. Ropinirole, a dopamine agonist, is a better alternative than pramipexole, which has the least incidence of constipation. In sigmoid volvulus, due to occlusion of both of the ends, the bowel gas is unable to escape, resulting in further dilation with ischemia and perforation3. In patients with possibility of gangrenous bowel or perforation, immediate surgical intervention is needed. If the symptoms are mild endoscopic detorsion should be considered. It is a safe procedure with mortality rates of 1% – 3%7, but with a recurrence rate between 3.3% and 60%. Percutaneous endoscopic colostomy is another modality of treatment for patients, if surgical intervention is not possible8. The differential of sigmoid volvulus includes ileosigmoid knotting (ISK), which is an emergency. In ISK there is vomiting but the radiographic findings are that of colonic distension9. ISK is often mistaken for simple sigmoid volvulus. However, unlike sigmoid volvulus, trials to deflate the distended colon by a sigmoidoscope or a flatus tube, often fail. Also, endoscopic reduction is contraindicated in ISK. Conclusion
The manuscript highlights the importance of constipation as a non-motor symptom in patients with Parkinson’s disease and its possible complications. Treatment of this condition may decrease morbidity and mortality in those patients. A rectal tube should be inserted in the preoperative period. Endoscopic detorsion should be performed in stable patients. This should be followed by sigmoid colectomy if the condition of the patient allows for surgical intervention. References
1.Drelichman, E. R. & Nelson, H. (2004). ‘Colonic Volvulus,’ In: Cameron JL, Editor. Current Surgical Therapy. 8th ed. St. Louis (MO): C.V. Mosby.