A. L. Hemalatha, N. S. Nayana, Deepthi B. Ramesh and Neelima P. Chamarthy
Department of Pathology, Mysore Medical College and Research Institute, Affiliated to RGUHS, Mysore, India
Volume 2013 (2013),
Article ID 459201,
International Journal of Case Reports in Medicine,
5 pages,
DOI: 10.5171/2013.459201
Received date: 11 June 2013; Accepted date: 11 July 2013; Published date: 23 September 2013
Academic Editor: Chandrasekhar Sekhar Bal
Cite this Article as:
A. L. Hemalatha, N. S. Nayana, Deepthi B. Ramesh and Neelima P. Chamarthy (2013), "Hunt for the Primary–A Diagnostic Drive in Reverse Gear!!!," International Journal of Case Reports in Medicine, Vol. 2013 (2013), Article ID 459201, DOI: 10.5171/2013.459201
Skeletal metastasis from primary hepatocellular carcinoma is rare ranging from 03 to 20% and is mostly seen in autopsy cases. Patients presenting with symptoms of bone metastasis are still rarer. Only a few cases of metastasis to bone from hepatocellular carcinoma have been reported as per literature review. Other cancers like breast, prostate, and lung carcinomas show an increased incidence of metastasis to bone. The most favored sites for extrahepatic metastasis from hepatocellular carcinoma are lung, central nervous system, and lymph nodes. The most common sites for metastasis to bone from hepatocellular carcinoma are cranium and pelvic bones while the long bone (femur), as in the present case, is the most uncommon site for metastasis from hepatocellular carcinoma. A case of asymptomatic primary hepatocellular carcinoma presenting with pathological fracture due to tumour metastasis to femur is presented here for its rare and unique features.
Skeletal metastasis in a patient with hepatocellular carcinoma (HCC) is rather uncommon, and hence liver is the most overlooked site during investigation of patients presenting with clinical features of metastasis to bone [1]. Though HCC is one of the more common cancers in the world with an early and frequent lethal intrahepatic spread, distant hematogenous metastases are infrequent. Primary HCC is often diagnosed only at a late stage where surgical resection is not possible [7]. The incidence of metastasis from HCC associated with symptoms at presentation accounts for less than 5% of cases. The majority of HCC cases reveal the evidence of metastasis at autopsy mainly to the lungs, central nervous system (CNS), and lymph nodes [4,5]. Hepatocellular carcinoma (HCC) metastasizing to bones is rare ranging from 3% to 20% and is mostly seen in autopsy cases [1,2]. The more common primary cancers which metastasize to the bone are from the breast and the lung [9]. The more common sites for metastasis to bone from HCC are flat bones like cranium and pelvis [2], but metastasis to long bones as in the present case is very rare accounting for less than 0.5% incidence [7]. This case is presented for its unique features which include a solitary metastatic bone lesion, an unusual involvement of long bone by secondary deposits, and a reverse diagnostic exercise which revealed an unusual location of primary carcinoma in the liver.
Case History
A 60-year-old male, a chronic smoker and an alcoholic, presented with pain in the left hip of 7 days duration, following a trivial fall. General examination showed no significant abnormalities. Local examination revealed tenderness in the left hip and in the upper part of left thigh. Radiograph revealed a sub-trochanteric fracture of left femur with an extensive lysis of bone and absence of periosteal reaction.
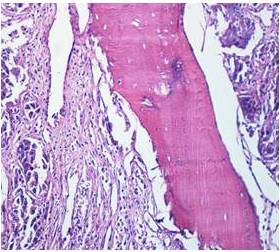
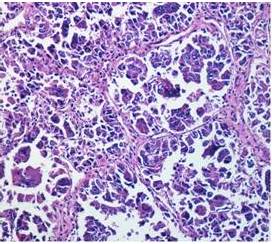
During open reduction and internal fixation, curetting from the fracture ends were obtained and submitted for histopathological examination. Histopathology showed massive destruction of the native architecture and replacement by a malignant epithelial tumour (figure 1) The tumour cells were arranged predominantly in trabecular patterns with intervening seams of native lamellar bone. These cells were large, and they had abundant eosinophilic granular cytoplasm, pleomorphic nuclei, prominent nucleoli, and intra-nuclear pseudo-inclusions (figure2)
Figure 1: Histopathology Section from Bone Curetting (H&E (10x)). Lobules of Epithelial Tumour Cells with an Intervening Fragment of Native Lamellar Bone
By correlating the classical histopathological features with the history of chronic alcoholism, the diagnosis of metastatic deposits to the bone from primary hepatocellular carcinoma was offered while a differential diagnosis of metastasis from renal cell carcinoma was also considered. And then began a wild hunt for the primary. A thorough clinical evaluation ruled out the possibility of primary in the lung, prostate, and breast.
Figure 2: Histopathology Section from Bone Curetting (H&E (40x)). Large Epithelial Tumour Cells with Abundant Eosinophilic Granular Cytoplasm Pleomorphic Nuclei, Prominent Nucleoli, and Intranuclear Pseudo-Inclusions
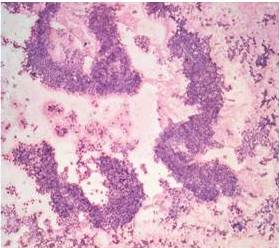
Ultrasound examination revealed a well-defined echogenic lesion in the right lobe of the liver. Simultaneously, a guided FNAC was performed. CT scan of abdomen and pelvis confirmed a hypodense lesion with areas of necrosis in the right lobe. Serum alpha-fetoprotein titer up to 563.3 ng/ml was recorded (normal values range from 2 to 10 ng/ml). Fine needle aspiration cytology findings (from hepatic lesion) revealed pleomorphic tumour cells arranged in trabecular and microacinar patterns. The cell clusters had a smooth edge, and some of them showed an endothelial wrapping (Figure 3).
Figure 3: FNAC Smear (H&E (10x)). High Cellularity, Epithelial Tumour Cells in Large Solid Sheets, and Trabecular Patterns
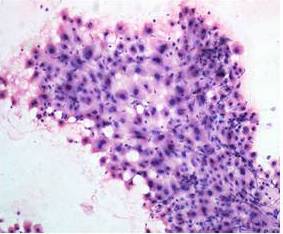
The tumour cells showed high nucleo-cytoplasmic ratio with large nuclei and macro-eosinophilic prominent nucleoli. Also seen were the intra-nuclear cytoplasmic inclusions (Figure 4). Cytological diagnosis of primary hepatocellular carcinoma was arrived Correlative cyto-histological final diagnosis was hepatocellular carcinoma with metastasis to the left femur.
Figure 4: FNAC Smear (H&E (40x)). Pleomorphic Tumour Cell Cluster with Smooth Edge and Endothelial Wrapping. Tumour Cells with High N: C Ratio, Large Nuclei, Prominent Nucleoli, and Occasional Intranuclear Inclusions
Discussion
The majority of the HCCs present with clinical manifestation of hepatic disease and are thus easily identified. Occasionally, a primary hepatic tumour may remain quiescent and may present much later with extra hepatic manifestations due to metastasis by hematogenous route to lung, bone, CNS, and adrenal gland and rarely to the bone as in the present case [7].
There are case reports in the literature of patients presenting initially with symptoms of bone metastasis from HCC. In this event, the most common presenting feature is the pathological fracture which is similar to that of the present case[6].
Most often, the metastatic deposits in bone are multifocal. In contrast, the unique feature of the present case is the presence of a solitary metastatic lesion in the bone. Another outstanding feature in the present case is metastasis to the long bone. Metastases to flat bones (pelvis or cranial bone) are more common but are rarely encountered in the long bones. The incidence of HCC metastasis to femur is less than 0.5% [3]. The prognosis is better when the initial presentation is with symptoms of bony metastasis without clinical manifestations of primary carcinoma as in the present case [1]. Conclusion
In the hunt for an occult primary carcinoma, however circuitous and tumultuous the drive, being even in the reverse gear, it seems like the exercise is worthwhile when the destination is promptly reached. References