1Haematology, Department of Pathology, Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
2Department of Pathology, Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
Volume 2014 (2014),
Article ID 165588,
International Journal of Case Reports in Medicine,
4 pages,
DOI: 10.5171/2014.165588
Received date: 31 January 2013; Accepted date: 25 February 2013; Published date: 9 January 2014
Academic Editor: Sudipta Sekhar Das
Cite this Article as:
Dammika Gunawardane and Chamani Gamakaranage (2014), "A Case of Warm Autoimmune Haemolytic Anaemia Presenting with Intravascular Haemolysis," International Journal of Case Reports in Medicine, Vol. 2014 (2014), Article ID 165588, DOI: 10.5171/2014.165588
Warm type autoiune haemolytic anaemia is mediated by IgG and complements; although rare, it may be mediated by IgA immunoglobulin as well. It causes extravascular haemolysis (EVH) in contrast to intravascular haemolysis (IVH) in cold AIHA. Intravascular haemolysis is extremely rare in warm type. We report a case of intravascular haemolysis in a 37-year-old Sri Lankan lady, who was successfully treated with steroid therapy.
Autoimmune haemolytic anaemia (AIHA) is rare (0.2—1.0 per 100000 population) but a potentially fatal condition (1,3). Diagnosis of AIHA is based mainly on Direct Antiglobulin Test (DAT/Coomb’s test) (2). AIHA is classified into warm (optimal autoantibody reactivity at 37°c) and cold (optimal autoantibody reactivity at 4°C) types, and based on the presence or absence of an underlying cause, it is classified into primary (idiopathic) and secondary (secondary to lymphoproliferative disorders, autoimmune disease, drugs, and nonhaematological malignancies). Warm type accounts for about 80%—90% of cases with AIHA. It can occur at any age, but mostly after 40 years of age (5).
Haemolysis in warm AIHA is mediated by IgG alone or with complements. Once immunoglobulins are bound, the red cells are taken up by the macrophages of the reticuloendothelial system with receptors for the Fc fragments of the immunoglobulins. This occurs mainly in the spleen, thus they are haemolysed extracellularly. Intravascular haemolysis is unusual in warm AIHA, although it is expected to occur as warm fixing-complements autoantibodies (4, 5).
We report a case of warm AIHA in an adult with an evidence of IVH.
Case History
A 37-year-old mother of two children was seen in the haematology clinic, for investigation of anaemia, 3 months after her second delivery. She complained of fatigue and headache (otherwise asymptomatic). The anaemia was detected during the antenatal period of her second pregnancy in routine checkups in the obstetric clinic.
She is a patient diagnosed with diabetes mellitus and hypothyroidism for 10 years. She had undergone thyroidectomy for Hashimoto’s thyroiditis, and her medications include thyroxine and metformin. However, she was on insulin (Humulin 70/30) during her pregnancy and the postpartum period. She did not have a significant family history of known haematological disease or recurrent blood transfusions.
At presentation to the obstetric clinic, she had been pale, icteric, and afebrile. There had been a tender hepatomegaly (4 cm) but no palpable splenomegaly or lymphadenopathy was noted.
Her haemoglobin had been 2.82 g/dl warranting urgent blood transfusions.
Investigations
The investigations are summarized in Table 1 and are given in the following.
Discussion
Warm type comprises 80%-90% of all cases of AIHA and can occur in all ages but mostly above 40 years with a peak around 70 years of age (5). The clinical presentation may be of insidious onset (most commonly) or acute and can have life-threatening fulminating haemolysis (4). The haemolysis is mediated by IgG antibodies which react optimally at 37 °C. The haemolysis is mainly extravascular, primarily in the spleen and to some extent in the liver as well. Although many warm antibodies fix complement, intravascular complement mediated haemolysis and haemoglobinuria are unusual in warm AIHA (5). But, complement mediated intravascular haemolysis sometimes occur in warm AIHA, resulting in haemoglobinuria and haemosiderinuria (4). Autoagglutination of red cells can occur in some patients with warm AIHA, which can be differentiated from cold autoagglutination that occurs in cold AIHA by the reversal of agglutination by warming to 37°C in the latter, but not in the warm type (6).
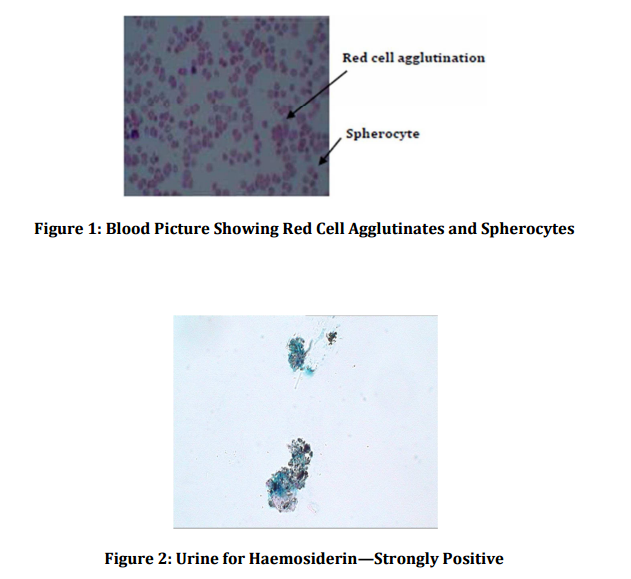
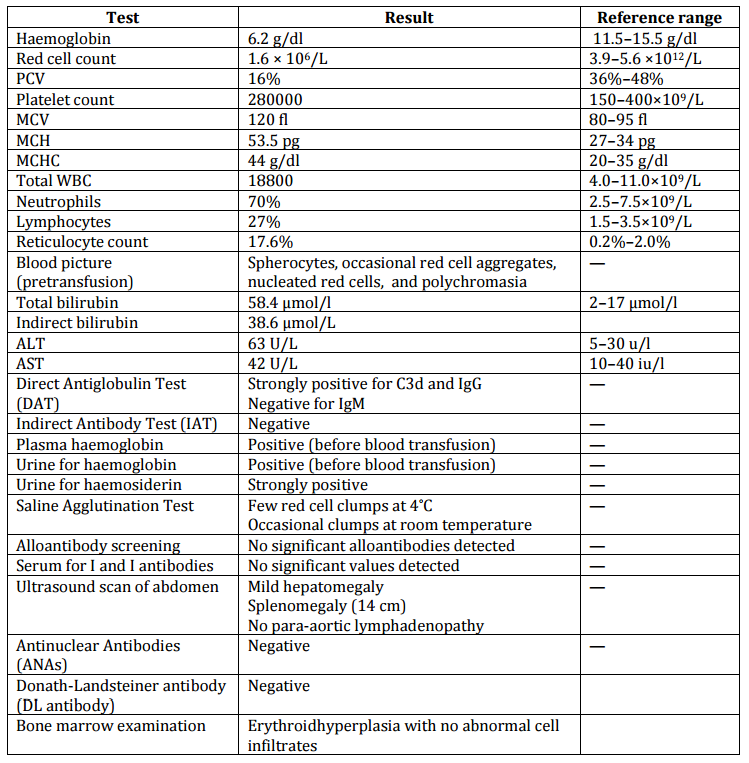
As shown in her investigations, she has presented with a severe spherocytic haemolytic anaemia with a positive haemolytic screen, that is, reticuloculocytosis, indirect hyperbilirubinaemia, and erythroid hyperplasia in the bone marrow. This Direct Antiglobulin Test is positive for both C3d and IgG, compatible with the warm type of AIHA. However, unexpectedly, her urine was strongly positive for haemosiderin and also demonstrated haemoglobinuria (confirmed with repeat testing) indicating the presence of IVH.
Rarely, there could be mixed (both warm and cold types) type of AIHA, where there could be intravascular haemolysis coexisting with EVH. Negative IgM antibody test makes this unlikely although it is difficult to exclude as there could be an undetectable amount of IgM antibody activating complements to cause IVH in this patient. We did not check for IgA antibodies due to technical difficulties, which anyway regarded as a mediator of warm AIHA which results in IVH though the mechanism is not yet understood (4). The haemolysis may be more intense with the presence of more than one subclass of IgG, which can result in IVH; the detailed analysis of antibody subclasses and their characteristics were not assessed due to the resource restrains (4). Alloantibody screening was negative, excluding the possibility of alloantibody-mediated haemolysis in this multiparous lady.