Alexander Dubcek University of Trencin. Študentská, Trenčín, Slovak Republic
Volume 2022,
Article ID 692971,
Journal of Human Resources Management Research,
11 pages,
DOI: 10.5171/2022.692971
Received date: 23 September 2021; Accepted date: 24 August 2022; Published date: 13 October 2022
Cite this Article as:
Sergej Vojtovic and Emilia Krajnakova (2022)," Trends in Physician Remuneration and Issues with Physician Staffing in Healthcare ‘, Journal of Human Resources Management Research, Vol. 2022 (2022), Article ID 692971, DOI: 10.5171/2022.692971
The lack of physicians in the healthcare system of the Slovak Republic is a long-term problem. In order to provide the health sector with the necessary personnel, the economic instruments of government and departmental policies are focused on the total financial expenditure on the health sector and, above all, on salaries. Several analyzes and studies of the given problem indicate that remuneration for work in healthcare is one of the most important factors, which is characterized by high indicators in the assessment of working conditions by physicians themselves. At the same time, remuneration has a relatively low impact on providing medical facilities with the necessary number of physicians. Therefore, the explanation and justification of this dilemma becomes the main task of the given study. At the same time, this means that the subject of our analyzes and investigations are primarily trends in remuneration, and the state of physician staffing in the Slovak healthcare system. For these purposes, we collect and analyze data on the following issues: trends in salary levels over the last decade, number of physicians in healthcare facilities in individual years, and number of physicians in healthcare facilities in different age categories. Based on these analyses, the degree of influence of changes in wage levels in the named years on the number of physicians of individual age categories in healthcare facilities is justified.
Keywords: Healthcare, remuneration, salary level, shortage of physicians.
Introduction
In the countries of Central and Eastern Europe, the shortage of healthcare workers appears after the expansion of the European Union, the liberalization of labor markets and the subsequent migration of healthcare workers for work in the countries of Western Europe. Over time, the extent of migration flows for work abroad keeps growing, furthered by making university students of medical and secondary health schools aware of new possibilities for work as well as for the way of life. Since the older generation of physicians did not have these opportunities, there was no need to orientate themselves towards work and life abroad and to adequately prepare for potential move for work abroad. This is primarily about language knowledge and skills, without which it is impossible to work in the healthcare facilities of selected target countries. Knowledge of the culture of another nation and country, art and the ability to adapt in a new geographical and social environment are also important in such case.
Even before the mentioned period, labor markets in the countries of Western Europe had been experiencing a chronic shortage of workers for a long time. The health sector and the medical personnel were no exception. This situation in the labor markets of the Western European countries preceded the events and processes triggered by the global financial crisis of 2008. The initial response of the governmental migration policies of the Western European countries was primarily to protect the labor markets for domestic workers, to target the scope of migrant workers, to limit their immigration mood and encourage return migration. However, only countries with a large number of immigrants pushed for relatively tough measures against the new wave of migration. At the same time, the financial crisis revealed previously invisible problems of the labor market, which required a different perception and evaluation, as well as different current economic and social processes. As a result, immigrants who were perceived as a social security threat came to be seen as an economic asset. And the government’s measures and policies create space for exercising its protective role towards immigrant workers. [Kuptsch, 2011: 269].
After the end of the financial and economic crisis of 2011-2012, progress in economic development is observed in all countries. The growth in the scale of investment in economic competition, especially in innovative industries, creates new jobs, which causes an even greater shortage of workers compared to the pre-crisis period. At that time, healthcare was one of several rapidly developing sectors of the world economy. According to OECD data, employment in the healthcare sector of European countries during this period expanded by an average of 12–15% [OECD, 2019]. That is why there is a chronic shortage of healthcare workers in most European countries [Skills, 2020]. The migration of medical personnel to the countries of Western Europe did not manage to fully solve this problem, but in addition it also caused a significant shortage of physicians and nurses in such Central European countries as Latvia, Poland, Hungary and Slovakia [Hardy, et al., 2014a].
Theoretical Background
Staffing medical facilities with the necessary number of physicians has become a pressing problem for Slovakia after its entry into the European Union. This means that the origin of this problem is not related to the local economic and social conditions of the Slovak Republic and has wider European dimensions. The chronic shortage of healthcare workers was observable in the countries of Western Europe even before the expansion of the European Union to include the countries of Central and Eastern Europe. Therefore, the shortage of medical personnel in the countries of Western Europe remains unsolved to this day, despite the regular migration flows of medical personnel from Eastern European countries. The problem with the shortage of medical personnel is largely exacerbated by the aging of the population and the growing demand for medical care. This applies equally to the countries of Western as well as Central and Eastern Europe. The fact that medical facilities in the countries of Western Europe from the time of the named migration waves, although not to the full extent, are regularly replenished with the necessary personnel from the number of immigrants makes the composition different. The departure of medical personnel regularly occurs in the countries of Central and Eastern Europe and, for this reason, their shortage is felt to a greater extent.
Despite this, the growing emigration flows of healthcare workers from the countries of Central and Eastern Europe did not solve the problem of healthcare staffing in the countries of Western Europe. This has been caused by the population aging processes in the countries of Western Europe that have lasted for more than half a century. For this reason, one of the most frequent key concerns in several Western European countries is to meet the growing demand for healthcare for the elderly. Therefore, the problems related to financing the provision of healthcare for the elderly and its support are constantly growing and becoming current and important topics of social gerontology [Khan, et al., 2013]. Even the aging of the population in the academic and professional communities is recognized as a global phenomenon that has become a multidisciplinary object of interest for scientific and professional analyzes in both Western and Central and Eastern European countries.
In contrast, the aging of the population in the countries of Central and Eastern Europe is a phenomenon of only recent decades. Nevertheless, the resulting increase in healthcare costs is recognized in most European countries. However, the perception and evaluation of these problems and the subsequent creation of adequate policies, which are considered suitable for their solution, are different in the countries of Central and Western Europe. The creation and implementation of the named policies is largely influenced by the available economic and social potential, the quality and balance of the policies themselves and the planned measures. In addition, the influence of the views of “new institutionalism” is visible, when feedback processes play an important role in the creation and implementation of reform policies in the provision of healthcare [Taylor-Gooby, 1996].
Healthcare systems that take into account data on financing, expenditure, provision and access to healthcare are currently in place in most European countries. These healthcare systems have been institutionalized to allow targeted access to health services. Therefore, when analyzing the effectiveness of healthcare systems in individual countries, as a rule, the focus is usually on their differences and on institutionally specific approaches to health services. Based on these characteristics of healthcare systems using cluster analysis, Claus Wendt [2009] created and justified the relevance of three types of healthcare systems. The first of them is distinguished by a large number of health service providers and a free access of patients to the provision of healthcare. The second type, which Claus Wendt named universal, provides healthcare based on the legal status of social citizenship with adequate control mechanisms. And lastly the third type, where financial resources for healthcare are limited and patients’ access to health services is regulated by high private payments, which Claus Wendt called low-budget.
Since the 1990s, various reform measures and balanced financial policies have been implemented in the countries of the European Union, which force healthcare systems to privatize healthcare facilities and reduce expenditures on the provision of healthcare from public sources. These reform measures were a response to long-term population aging processes, growth in the scope of healthcare provision and funding sources. In professional studies, these measures were divided into three categories and named unhealthy European health policy [Vos, et al., 2004]. The first category included measures associated with the growing influence of government structures on the organization of healthcare in order to enable the restructuring of healthcare facilities. Another category included measures aimed at reducing public spending, including higher financial contributions from patients and limiting the scope of provided health services. The measures of the third category were aimed at introducing competition, privatization of health services and insurance systems. And this provided opportunities for the businesses of large corporations and companies, as well as for small and medium-sized and especially family businesses [Srovnalikova, et al., 2018]. It was expected that the results of the implementation of the named measures will contribute to the reduction of public expenditures, the growth of financial resources for private healthcare and, at the same time, the growth of the profits of private healthcare providers. As stated by the authors of the study, “Ongoing European healthcare reforms thus struggle with the contradictions between responding to growing collective needs and securing or increasing private profits” [Vos, et al., 2004: 255].
In this context, it is necessary to emphasize that the reason for the expansion of private activities in the provision of healthcare is the inability of national health systems to handle the growing costs, especially in terms of co-financing and the growing demand for health services. The introduction of private health insurance reduces payments from private sources and in the long term leads to the development of a broader system of social health insurance. [Sein, 2021]. There are opinions that the shortest path to respect for human dignity, the common good, subsidiarity and solidarity in the health sector, is the establishment of a free market for the provision of healthcare. And interfering with the patient-physician relationship and the economics of centrally planned healthcare “harm patients and physicians, and create morally evil outcomes and economic structures.” [McKalip, 2016: 423].
In European countries, healthcare is provided in the form of two systems – national and social security. These healthcare systems differ considerably in terms of ongoing processes, reform measures, structural elements, sources of financing, and the scope and quality of provided healthcare. At the same time, it also has an important impact on the nature and severity of the problems that occur in these types of healthcare systems. The advantage of the national system is the greater efficiency of healthcare provision processes, more effective cost control and fairness in the distribution of funds. Nevertheless, the analysis and investigations of this issue indicate that client satisfaction in this system is lower than in social security systems. As the author further emphasizes, the effort to overcome these differences in these healthcare systems is the main goal of the implemented reforms [Elola, 1996: 239].
The reforms implemented in healthcare systems fulfill another important role – they affect the integration of these systems into a larger whole. An important tool of this integration is the privatization of health services according to the restrictions of the Maastricht economic convergence and EU accession criteria. Another tool of the so-called integration is the mobility of healthcare workers and patients as a form of free movement of workers and services within the single European economic area. And the third important tool of the named integration processes are the new EU laws and regulations on the management of economic affairs. These legislative standards are issued by the EU for individual countries after the financial crisis of 2008. It was these measures that influenced the creation of the European healthcare system, which is uneven in terms of patient access to services, working conditions and salaries of health workers in all EU member countries [Stan, Erne, 2021]. Other authors also emphasize that even before the word pandemic became part of the communication lexicon, pressures resulting from institutional changes called for policymakers and healthcare providers to rethink the basic ways in which healthcare is provided. At the same time, these pressures pointed to the need to reform the healthcare system in terms of its obvious shortcomings [Agar, et. al., 2020; James, 2021].
The differences in the provision of healthcare in the countries of Central and Western Europe can be explained by their institutional characteristics, which means lower funding, higher payments and higher direct costs for the provision of healthcare, and a lower offer of primary healthcare services [Popic, Schneider, 2018]. For example, since the end of the 1990s in the countries of Central Europe, a mixed, so-called solidarity health system has been applied, which is financed primarily from the national fund and compulsory health insurance [Riklikiene, et al., 2014]. In addition, similar reform measures are also starting to be implemented in the healthcare systems of Central European countries during this period. Differences in the approach to healthcare provision between the health systems of Eastern and Western European countries are often explained in terms of the legacy of socialism. However, already during the last two decades, the provision of healthcare in the countries of Central Europe is primarily influenced by the specifics of its institutional arrangement. The problems in the European healthcare systems based on the analyzes and findings are emphasized from the time of the implementation of the first reform policies in the Western European health sector.
The processes of labor market liberalization in the healthcare as a result of the enlargement of the European Union in 2004 and 2007 significantly influenced the transformation of this sector throughout Europe and at the same time increased the mobility and migration of healthcare workers. The migration of healthcare workers from Eastern European countries is relatively low compared to the number of healthcare workers in Western European countries. Nevertheless, this movement of experts in the field of healthcare primarily has an impact on the healthcare systems of Central European countries. For example, approximately 203 Slovak physicians work in the United Kingdom, which is slightly more than one percent of the total number of physicians in Slovakia (N=19178). Compared to the total number of physicians (N=196784) in the United Kingdom, this number is negligible and represents only 0.1%. [OECD, 2019]. This pattern also applies to Central European countries such as Romania, Hungary, the Czech Republic, Poland and the Baltic countries [Hardy (b), et al., 2014].
The shortage of workers in the healthcare system in the European Union is still a pressing problem related to new social and political dilemmas as well as migration flows of healthcare workers [Lozano, et al., 2015]. This primarily means that, for example, Spain, for which the United Kingdom was the destination country of migration, has today become the destination country of migration for the countries of North Africa and Latin America. Just as, for example, the target countries for Slovakia were the countries of Western Europe, today it is the target country for Ukraine, Romania and Serbia. Named migration flows of healthcare workers are for several countries an additional source of providing healthcare facilities with the necessary staff. At the same time, for the developed countries of Western Europe, immigrants “provide an essential source of cheap labor and their use has always been an important part of cost reduction and rationalization in the provision of healthcare” [Doyal, et. al., 1981: 54]. Traditionally this is justified as a form of “aid” to the Third World, in the form of training healthcare workers who then return to their home countries. However, several analyzes and studies of this problem indicate that the majority of such workers do not return home as a rule [Lundholm, 2012; Gaillard and Gaillard, 2015; King, et al., 2017].
Analyzes of healthcare expenditure and healthcare financing in Western European countries are carried out primarily in terms of patient interests and access to health services using diverse institutional systems of health and social insurance. Despite the generally recognized and widely declared problem of the shortage of healthcare workers, only in rare cases professional publications and scientific studies emphasize that the provision of healthcare “directly depends on the availability of workers willing to provide this type of care” [Pearlman, et. al., 1991]. Analyzes of healthcare expenditures and healthcare financing in most cases are not connected with the provision of healthcare with the necessary personnel and do not move towards finding the nature and causes of the lack of healthcare workers.
As a rule, the professional community considers the main component of the healthcare system to be the institutional system of patient access in connection with the method of payment for the provided healthcare. And the medical staff in such a case is “perceived” more as a technical component of the processes of providing healthcare, as a medical device for which it is necessary to create a named institutional system. Under the conditions of the availability of financial resources, the healthcare facility will acquire the named “device” (medical personnel) and then create an institutional system of access to it and a method of payment for the provided healthcare service. In the absence of a given “medical facility”, it does not automatically require the creation of an institutional system of access to it and the method of payment for the provided medical service.
When providing healthcare with material or equipment, it is sufficient to have the necessary financial resources. When ensuring that medical facilities are staffed with the necessary personnel, it is insufficient to have only finances. In addition to financial resources, it is necessary to ensure working conditions that are acceptable for health workers. Therefore, we cannot perceive the medical staff as a material or technical component of the healthcare system. These are human beings who are able to evaluate, reason and make decisions based on raw stimuli. Expenditure on healthcare and the financing of healthcare affect medical personnel not only in the form of remuneration for work. Physical, hygienic working conditions, material, equipment of workplaces, which are not directly related to remuneration and the amount of wages, also fundamentally influence the decisions and willingness of healthcare workers to work at jobs in the healthcare system.
While the global shortage of workers in the health sector of the countries of both Western and Eastern Europe continues to be relevant issue. Nevertheless, the exact and comprehensible causes of this phenomenon are not universally explained. In addition to the remuneration for work, which affects employment in the health sector, organizational, social, hygienic and other conditions of work in the health sector are important. And these are not determined by the amount of wages and are directly related to healthcare spending and healthcare financing. Based on this, the goal of this study is to determine the connection between the amount of physicians’ remuneration and healthcare expenditures and the objective state of ensuring that medical facilities are staffed with the necessary personnel.
Methodology and Data
Investigating the connection between healthcare financing and healthcare staffing is a relatively complex and extensive methodological problem. Methods, tools, principles and research approaches used are diverse and unique both in terms of their applicability and difficulty, as well as in terms of the final epistemological results. Findings that are based on the description of facts – statistics will always be different from findings obtained on the basis of subjective data – expressions, evaluations, behavior of subjects, etc. We can find out what we are changing with the help of a system of statistical data about facts, phenomena, processes; we can ask the actors about these processes and facts. As a rule, the results of the named research methods will be different, but equally important and valuable.
Our analytical activities are focused on the relationship between the state of healthcare staffing (the number in individual time periods, changes in the number and their intensity) and objective indicators of the wage levels, their dynamics, etc. However, such a task would be beyond the scope of a single study. That’s why we limited ourselves to finding the connections between the indicators of healthcare expenditures and, above all, the level of wages and the state of staffing of healthcare facilities in Slovakia with the necessary number of only a single category of healthcare workers, namely physicians. This means that the main goal of the given study is to define the degree of dependence between the indicators of healthcare expenditure and the level of salaries and the indicators of securing an adequate staffing of physicians for the Slovak healthcare system.
The realization of this goal requires the fulfillment of the following tasks and analytical activities – obtaining the necessary information and data, statistical data, accepting certain principles and tools for their collection and generalization, choosing and using adequate methods of analysis and processing of the obtained information. An important indicator of our analyzes is the state of healthcare staffing in Slovakia by physicians, expressed by indicators of their number in individual years, indicators of the number in individual age categories and interannual dynamics. The second subject area of our analyzes are indicators of wages in the healthcare sector and their year-on-year dynamics.
Another task of our analyzes is to determine the correlation dependence between the mentioned variables. For this purpose, we use the Pearson correlation coefficient. In such case, the use of indicators of salary dynamics and migration decisions of physicians over a larger period of time is required. In our case, we determined a ten-year time span – from 2012 to 2021. That is primarily because this decade saw significant changes in the remuneration of physicians in the Slovak healthcare system.
At the same time, in this period, a shortage of physicians is observed in healthcare facilities in Slovakia, caused by a general growth in the scope of healthcare provided due to the aging of the population. The lack of physicians in healthcare facilities is exacerbated by the retirement of the physicians and also their leaving to work abroad as a result of the liberalization of labor markets in the European social space after Slovakia’s entry into the EU. We drew data on the named indicators from the Slovak Medical yearbook, which provides comprehensive statistical data on the Slovak healthcare system, and the statistical data collected and published by Organization for Economic Co-operation and Development (OECD).
Results and Discussion
When approaching the shortage of physicians in the health facilities of the Slovak Republic, we started from the assumption that this problem is largely influenced by the funding of the healthcare sector. The influence of financing on the number of physicians in healthcare facilities is actualized through several mechanisms, such as remuneration for work, expenses for material or equipment of healthcare facilities, improvement of hygienic, safety or social working conditions. Due to the vastness of this issue and the complex mechanisms of the impact of financing on the healthcare staffing, we focused on only one category of medical personnel, namely physicians, and on the remuneration for their work. The first variable is expressed in the interannual dynamics of the total number of physicians in individual age categories, and the second in the interannual dynamics of average salary indicators in the period from 2011 to 2020. This means that we want to find out whether the interannual changes in the average salary of physicians are correlated with their overall number and also with their number in individual age categories.
Of course, wages and other working conditions in medical facilities do not have the same meaning for individual age categories of physicians. In the case when the level of wages and other working conditions in medical facilities are not attractive, younger age groups of physicians have the opportunity to look for employment in other sectors and spheres. These may include, for example, state and public health institutions, insurance companies, science and research, or ultimately migration for work abroad. At the same time, to a certain extent, this pattern of behavior can be effective for other categories of physicians who are already employed in medical facilities, but are not satisfied with the remuneration or other working conditions. Changes in working conditions in the healthcare sector may attract post-productive age physicians for whom working abroad is no longer an option. Or, on the contrary, under the deteriorating conditions of employment, physicians in post-productive age will try to end their work in medical facilities and retire.
The development of year-on-year indicators of the average salary for physicians and their overall number in healthcare facilities in the monitored decade is shown in Tab. 1. In 2011, the average monthly wage was the lowest for the entire analyzed period and regularly grew from year to year – by the end of the monitored period it had grown by 83.1%. The total number of physicians also grew (with an exception of a decrease in 2017) and in 2020 reached 20026, which was 11.3 percent more than in 2011.
Table 1: Total number of physicians and their average salary in the healthcare sector of the Slovak Republic for the period 2011-2020
Source: NCZI: Zdravotnícka ročenka, 2018, 2021.
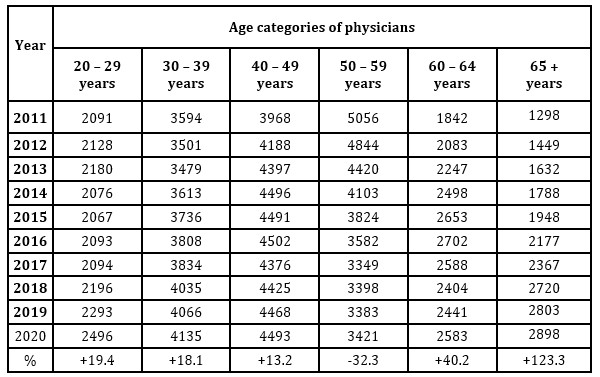
The number of physicians in the age category 20-29 grew by almost the same 19.4 percent during the monitored period (see Table 2). In this case, it is mainly about graduates of medical faculties and universities. For example, only 4% of the total number of university graduates graduated in health sciences in Slovakia in 2010, and in 2020 this indicator was at the level of 8% of all graduates (after deducting foreigners). If we look only at medical sciences, the 1.5% share of medical graduates in 2010 grew to 2.7% in 2020. The number of physicians in the 30-39 and 40-49 age categories increased by 18.1 and 13.2 percent, respectively. At the same time, a significant decrease in the number of physicians in the 50-59 age category was recorded by 32.3 percent. However, the number of physicians aged 50-59 grew by 40.2 percent and by an extreme 123.3 percent in those aged 65+. However, this simple statistical overview reveals a certain regularity – an almost proportional regular growth of the average salary (by 83.1%) and an 11.3 percent growth in the total number of physicians, as well as from 13.2 to 123.3 percent in individual age categories, with the exception of age category 50-59 years.
Table 2: Total number of physicians, their number in individual age categories and average wage in healthcare in Slovakia for the period 2011 – 2020
Source: NCZI: Medical Yearbook 2021; Statistical yearbook 2020.
We will take a closer look at these data through the prism of correlations (Tab. 3). The average annual salary of physicians in the studied period grew regularly without fluctuations and grew by 83.1 percent. In contrast, the number of physicians grew much more moderately and with a decrease in 2017. Over the entire ten-year period, the number of physicians in health facilities grew by 11.3 percent, which in absolute terms means 2,177 persons. The value of the correlation coefficient between the growth of the number of physicians in the monitored period and the growth of the average salary is 0.9415. It is a strong positive correlation between the named variables, which rather expresses the direction of changes in the indicators, but not their intensity. The average salary grew by 83.1 and the number of physicians by 11.3 percentage points. In such a case, one could agree that the increase in the number of physicians was influenced by the growth of the average salary, provided that the number of physicians reached its absolute possible ceiling. However, the situation is still different today. Even before the onset of the COVID-19 pandemic, the country’s healthcare facilities experienced an acute shortage of healthcare workers, including physicians. And at the height of the second wave of the pandemic, Slovakia was forced to invite physicians from other countries for help. Therefore, in the given case, it can only be identified with the fact that the evidently significant growth of the average salary evidently had a certain influence on the growth of the number of physicians. However, such a significant increase in the average salary of physicians did not solve the given problem – it did not attract the necessary number of physicians to health facilities.
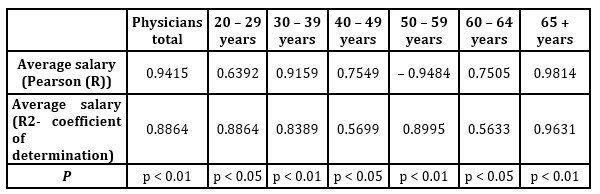
Table 3: Correlation matrix of indicators of change in average wage, total number and number of physicians in individual age categories
A different regularity is observed between the indicators of the number of physicians and the average salary in individual age categories of physicians. There is a slight positive correlation between the average salary and the number of physicians in the 20-29 age category, indicating that there is a tendency to score high on these variables. The value of the correlation coefficient is 0.6392. These indicators do not provide conviction for the claim that the growth of the average salary also influenced the growth of the number of physicians in the given age category. In the category of physicians aged 30-39, the value of the coefficient is 0.9159. This is a strong positive correlation of the variables. In the next category of 40-49-year-old pharmacists, the value of the correlation coefficient (0.7549) indicates a strong positive correlation, which means that a high score of the variables of average salary is associated with a high score of the variables of the number of physicians of the given category over a ten-year period. However, as in the case with the total number of physicians, the value of the correlation rather reflects the direction of changes – the regular growth of the number of physicians and the average salary, rather than their intensity.
The category of physicians aged 50-59 shows the opposite tendency of dependence between the named variables. The regular year-on-year growth of the average wage was accompanied by a regular year-on-year decrease of healthcare workers in the given age category. There is a strong negative correlation with a correlation coefficient value of -0.9875 and a high (0.9752) coefficient of determination value. For this category of physicians, the regular and significant increase in the average salary for the conditions of Slovakia was irrelevant. At the same time, this does not mean that the growth of the average salary influenced the departure of physicians of the given age category from the healthcare sector. The explanation of this phenomenon must be sought in certain demographic changes and above all in the so-called “demographic jump” in the 1960s in the former Czechoslovakia.
Indicators of the value of the correlation coefficients of the other two age categories of physicians, namely 60-64 and 65 years old and older, show that the increase in their number in the Slovak healthcare system can be influenced by the growth of the average salary. This cannot be claimed in relation to the total number of physicians and also to the previously analyzed age categories. The correlation coefficients of the two categories of physicians show a strong positive correlation with a high value: 0.7505 for 60-64 years old and 0.9814 for 65+. older ones. This regularity is also confirmed by the absolute indicators of regular growth in the number of physicians in these categories and the average salary, with the exception of a three-year (2017-2019) decrease for 60-64-year-old physicians.
The specificity of these two categories is that they are primarily retirement categories, people in post-productive age. In conditions of an acute shortage of physicians, there are no obstacles to employment. Moreover, for physicians who were of retirement age in 2016-2018, when the average salary exceeded two and a half thousand euros and long-term previous work below the level of one and a half thousand, it becomes very attractive for them to stay at work. In such a case, older categories of physicians choose the alternative of being employed or continuing to work upon reaching retirement age. Only for the given categories of physicians, we can claim that the growth of the average salary in the observed decade attracted a larger number of physicians, although most of them were in their post-productive age, and thus contributed to solving the problem of ensuring the healthcare system with the necessary number of physicians only in a short-term horizon.
We cannot evaluate this regularity of the growth of the number of physicians as universal and suitable for solving the global problem of the shortage of medical workers. This source of healthcare staffing is limited by age. Those physicians who work abroad could contribute to the solution of this problem, of course not on a global scale, and only for the needs of Slovakia. Their return migration would be the appropriate mechanism that would contribute to solving the problem of the lack of physicians in healthcare facilities in Slovakia. Another category of physicians for solving this problem could be physicians aged 20-29. years. Basically, these are recent graduates of universities and faculties. But in principle, this category almost does not “react” to a significant increase in the salaries of physicians. The correlation between the growth of their number and the growth of the average wage is not high. The relatively larger increase in them over the analyzed decade, apart from the above-mentioned categories in the post-productive age, can be explained by the fact that they are in the decision stage – where, in which facility to get a permanent job, in which place or region, to stay in Slovakia or to look for work abroad.
The creation and implementation of perfect institutional policies for the provision of healthcare and improving the availability of health services are insufficient to solve the global problem of providing health facilities with the necessary number of personnel [Hardy, et al., 2014a]. Medical personnel are one of the important parts of the provided health services. At the same time, the services are made up of medical personnel. Therefore, in addition to other institutional activities and the creation of health policies [Taylor-Gooby, 1996], it is necessary to pay important attention to personnel policies and their financing [Khan, et al., 2013; Agar et al. al., 2020; James, 2021].
Conclusions
As our analysis and findings indicate, direct financing of healthcare in the form of compensation for work and wage rates is an effective mechanism for solving the global problem of shortage of health workers, including physicians, but only to a certain degree. Our findings show that only physicians in the post-productive age mainly responded to remuneration and wage growth in the analyzed period. For this reason, this category of physicians cannot be an effective resource for solving the global problem of shortage of health workers. Therefore, it is necessary to research and look for other effective resources and mechanisms that could be a more universal tool for solving this global problem. For example, it would be beneficial for the solution of the given problem to find out other forms of healthcare financing, such as percentage expenditures from GDP and financing of material, hygienic, social working conditions, healthcare equipment, the prestige of the medical profession, etc. Organization of work, overtime, urgent cases and their financing are important for physicians. These job characteristics are as important as direct forms of funding and could evidently be an effective mechanism for addressing the global problem of shortage of medical personnel in health systems.
Acknowledgments
This work was supported by the Slovak Research and Development Agency under the contract No. APVV-19-0579.
References
Avgar, A. C., Eaton, A. E., Givan, R. K. and Litwin, A. S. (2020), ‘Paying the Price for a Broken Healthcare System: Rethinking Employment, Labor, and Work in a Post-Pandemic World,’ Work and Occupations, 47(3), 267-279.
Doyal, L., Hunt, G. and Mellor, J. (1981), ‘Your Life in Their Hands: Migrant Workers in the National Health Service,’ Critical Social Policy, 1(2), 54-71.
Elola, J. (1996), ‘Healthcare System Reforms in Western European Countries: The Relevance of Healthcare Organization,’ International Journal of Health Services, 26 (2), 239-251.
Gaillard, A-M. and Gaillard, J. (2015), ‘Return Migration of Highly Skilled Scientists and Engineers to Morocco: Return or Circulation?’ Science, Technology and Society, 20 (3), 414-434.
Hardy, J., Calveley, M., Kubisa, J. and Shelley, S. (2014a), ‘Labour strategies, cross-border solidarity and the mobility of health workers: Evidence from five New Member States,’ European Journal of Industrial Relations, 21(4), 315-333.
Hardy, J., Shelley, S., Calveley, M., Kubisa, J. and Zahn, R. (2014b), ‘Scaling the mobility of health workers in an enlarged Europe: An open political-economy perspective,’ European Urban and Regional Studie, 23 (4), 798-815.
James, J. H. (2021), ‘Healthcare Financing for the Under-Served: UK,’ Journal of the Royal Society of Medicine, 94 (9), 462-465.
Kaminska, M. E. and Wulfgramm, M. (2018), ‘Universal or commodified healthcare? Linking out-of-pocket payments to income-related inequalities in unmet health needs in Europe,’ Journal of European Social Policy, 29 (3), 345-360.
Khan, H. T. A., Leeson, G. W. and Findlay, H. (2013), ‘Attitudes towards Bearing the Cost of Care in Later Life across the World.’ Illness, Crisis & Loss, 21 (1), 49-69.
King, R., Lulle, A., Parutis, V. and Saar, M. (2017), ‘From peripheral region to escalator region in Europe: Young Baltic graduates in London,’ European Urban and Regional Studies, 25 (3), 284-299.
Kovacheva, V. and Grewe, M. (2019), ‘Migrant workers in the German health-care sector,’ Hamburg Institute of International Economics, (HWWI). [Online], [Retrieved November 15, 2020]. Available at: http://www.imabe.org/index.php?id=2267
Kuptsch, Ch. (2011), ‘The Financial and Economic Crisis and Migration Policy in European Countries: A Revival of Labour Issues?’ European Labour Law Journal, 2 (3), 269-281.
Lozano, M., Meardi, G. and Martín-Artiles, A. (2015), ‘International Recruitment of Health Workers: British Lessons for Europe? Emerging Concerns and Future Research Recommendations,’ International Journal of Health Services, 45 (2), 306-319.
Lundholm,E. (2012), ‘Return to where? The geography of elderly return migration in Sweden.’ European, Urban and Regional Studies, 22 (1), 92-103.
McKalip, D. (2016), ‘Achieving Moral, High Quality, Affordable Medical Care in America through a True Free Market,’ The Linacre Quarterly, 83 (4), 423-444.
(2020), OECD Health Statistics – Definitions, Sources and Methods,[Online], [Retrieved May 14, 2022]. Available at: http://www.oecd.org/health/health-data.htm
Pearlman, D. N., Mahoney, D. F. and Callahan, J. J. (1991), ‘A shortage of long-term care workers: Effects on clients with dementia,’ American Journal of Alzheimer’s Care and Related Disorders & Research, 6 (5), 9-15.
Popic, T. and Schneider, S. M. (2018), ‘An East–West comparison of healthcare evaluations in Europe: Do institutions matter?’ Journal of European Social Policy, 28 (5), 517-534.
Riklikiene, O., Jarasiunaite, G. and Starkiene, L. (2014), ‘Informal patient payments in publicly financed healthcare facilities in Lithuania,’ Scandinavian Journal of Public Health, 42 (6), 488-496.
Sein, T. (2021), ‘Generating Financial Resources for Health,’ Journal of Health Management. 23 (1), 47-53.
Skills for care (2017), State of the adult social care sector and workforce. [Online], [Retrieved July 18, 2021]. Available at: http://sciencev1.orf.at/news/46665.html
Srovnalikova, P., Kordos, M. and Haviernikova, K. (2018), ‘Students’ Engagement into Family Business in terms of Cluster Cooperation within Family Businesses, Vision 2020: Sustainable Economic Development and Application of Innovation Management,’ Conference of the International-Business-Information-Management-Association (IBIMA), ISBN: 978-0-9998551-1-9, 15-16 November 2018, Seville, Spain, 5079-5088.
Stan, S. and Erne, R. (2021), ‘Time for a paradigm change? Incorporating transnational processes into the analysis of the emerging European health-care system,’ Transfer: European Review of Labour and Research, 27 (3), 289-302.
Štatistická ročenka Slovenskej republiky. (2018), VEDA, 2018. ISBN 9788022417006.
Štatistická ročenka SR 2021. (2022). [Online]. [Retrieved May 14, 2022]. Available at: https://slovak.statistics.sk/wps/portal/!ut/p/z1/tVJNU8IwEP01PabZNKFNvRVh-BAdARHIxWnSUCr0g1Ko_HtTx4OoMOPBHDLJztvd9_YtFniBRRYekziskjwLt-a_FO7L2BvwdpsEAF6rA4PhrDPuTX0CDPD8HMAfJl0YPAWPvcmQGUALi-v5z1hgobKqqNZ4mct9uEb7DSoO0gJzbZNNqBJtwfEkyzDT6GtMuZJwL1JIciUR05IhP6Ir5EQRaxEWUulCU71QSYSXroky4hPkeRFBjLgEyZBTBNqPwFfK9aX7Xc1Puo0auHCCZhriA3LbC_rMGwHwUa8Fg6A_m_hjSiGgn4ArNZaGg3eRw52D58dE13iW5WVqHJr-UWIf8BCLRKZ2rVIbbOJwz2UOYdx3qHk3lievu50IjC95Vum3Ci_-wRjTJsgk5TEWpV7pUpf2oTQLt66qYn9jgQV1Xdtxnsdbbas8tX5NWed7Q-8ciYt0lnJ6QpvVfZcyIU90G78DOrcY_g!!/dz/d5/L2dBISEvZ0FBIS9nQSEh/
Vlachynsky, M. (2021), ‘Chýbajúci zdravotníci: 21 zlepšení.’ [Online], [Retrieved July 7, 2022], Available at: https://www.humanisti.sk/2022/04/23/chybajuci-zdravotnici-21-zlepseni/
Vos, P. D., Dewitte, H. and Van der Stuyft, P. (2004), ‘Unhealthy European Health Policy,’ International Journal of Health Services, 34 (2), 255-269.
Wendt, C. (2009), ‘Mapping European healthcare systems: a comparative analysis of financing, service provision and access to healthcare,’ Journal of European Social Policy, 19 (5), 432-445.
Zdravotnická ročenka. 2020. [Online], [Retrieved May 17, 2022]. Available at: https://www.nczisk.sk/Documents/rocenky/2020/Zdravotnicka_rocenka_Slovenskej_republiky_2020.pdf